Sternocostoclavicular hyperostosis (SCCH) is a chronic osssifying diathesis affecting mostly juxtasternal structures and the inflammatory osteitis is mostly part of the synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome. we presented a case of 62-year-old woman with polyarthritis in bilateral hands, who had experienced swelling of anterior chest wall sinse she was 30 years old. we decided to treat her with an anti-TNF α antibody biologics, golimumab, after failure of conventional disease-modifying antirheumatic drugs (Cs DMARDs). Although clinical remisson had been successfuly induced, rapid progression of SCCH and skin menifestation were confirmed without recurrence of the peripheral arthritis.
Results of the bone biopsy and the culture study indicated the relapse of SCCH was not caused by infection or neoplasma and, postoperatively, the chest pain was gradually decreased and along with an improvement of the skin erruption.
Sternocostoclavicular hyperostosis, SAPHO syndrome, Anti-TNF-α therapy, Golimumab, Polyarthritis
Sternocostoclavicular hyperostosis (SCCH) is a chronic osssifying diathesis affecting mostly juxtasternal structures that was initially described in the Japanese medical literature in 1967 [1]. Clinical features of SCCH are pain and swelling of the affected bones and the inflammatory osteitis is mostly of part of the synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome, which was reported first by a group of French researchers in 1987 [2]. As genetic, infectious, and immunological factors have been implicated, the etiology remains unclear and the isolated skeletal manifestation of SCCH is recognized as a distinct medical and diagnostic term publishable in the literature [3]. The peripheral artiritis of SCCH may occur in up to 22% of patient [4], knee and ankle are involved most frequently, followed by the wrist and less commonly the proximal interphalangeal joints [5].
While there is overlap between SAPHO syndrome and SCCH, it is recognized that the SAPHO syndrome is a heterogeneous disorder, thus, its diagnosis maybe challenging esepecially when specific cutaneous menifestation are absent. In SAPHO syndrome, the course is usually prolonged and recurring and standardized treatment protocols are not available currently. In general, multi targeting drugs are used, iccluding, non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids (GCs), antiniotics, bisphosphonates, conventional disease-modifying antirheumatic drugs (Cs DMARDs), biologic DMARDs, and recently Janus kinase inhibitors.
Here, we presented a rare case of SCCH with polyarthritis of bilateral hands, suddenly relapsed with painful exacerbation of SCCH and skin erruption after clinical remisson, which had been successfuly induced by anti-tumor necrosis facor (TNF)-α therapy.
A woman, aged 62, presented with swelling and pain in metacarpal phalangeal (MP) and wrist joints of bilateral hands. She experinced swelling of anterior chest wall since she was 30 years old. However, she did not have any episode of severe anterior chest pain. Plain radiograph and computed tomography (CT) scan of her chest showed enlargement and hyperostosis of the left clavicle (Figure 1). Although there were no signs of bony erosions or destructive changes in MP, radio-carpal, midcarpal, and distal radio-ulnar joints of her bilateral hands (Figure 2), ultrasonography examination revealed hypoechoic synovial thickening associated with power Doppler signals in the bilateral radio carpal joints (Figure 3).
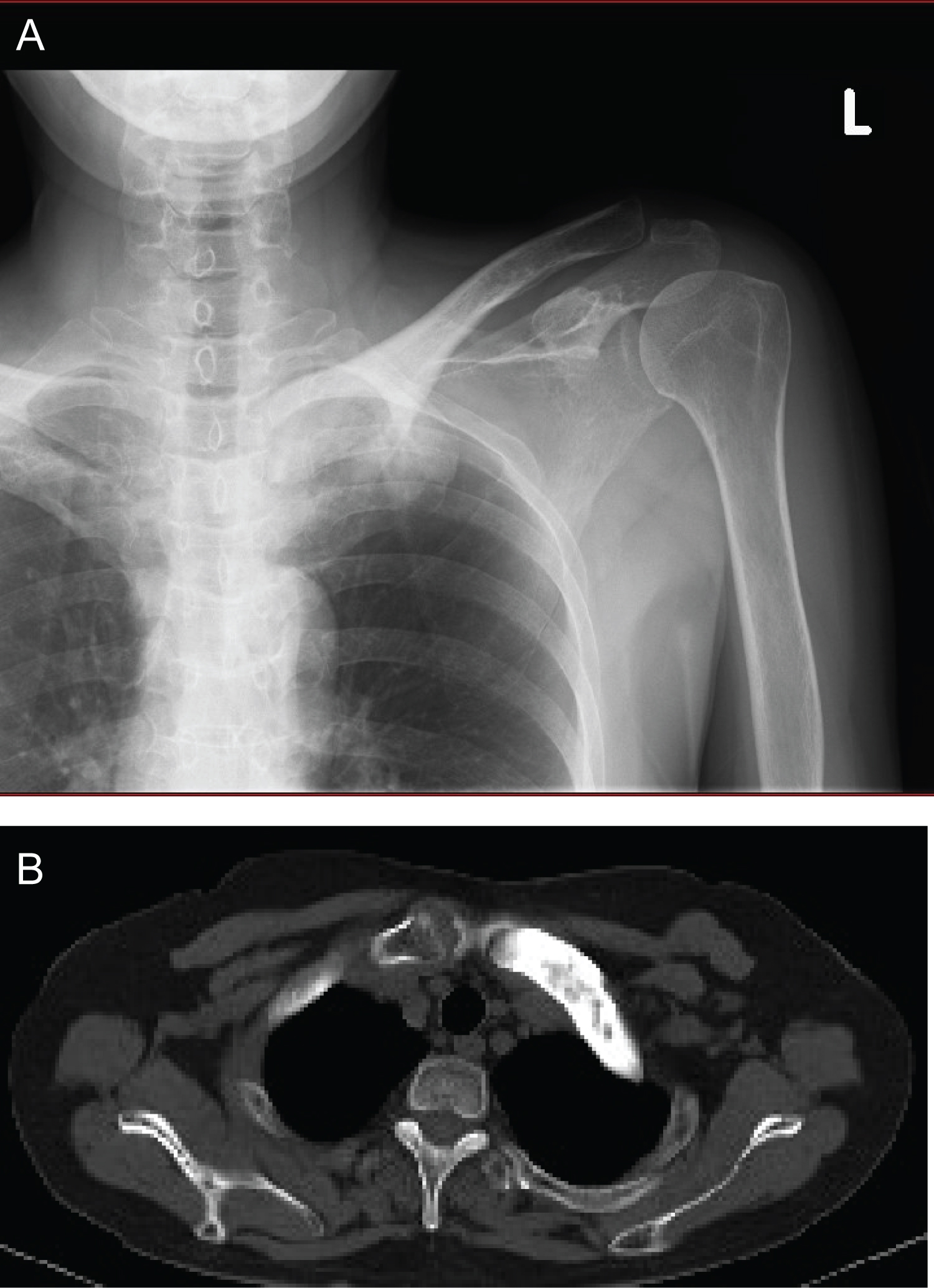 Figure 1: (a) Plain radiograph and (b) axial CT image of her chest showed enlargement and hyperostosis of the left clavicle.
View Figure 1
Figure 1: (a) Plain radiograph and (b) axial CT image of her chest showed enlargement and hyperostosis of the left clavicle.
View Figure 1
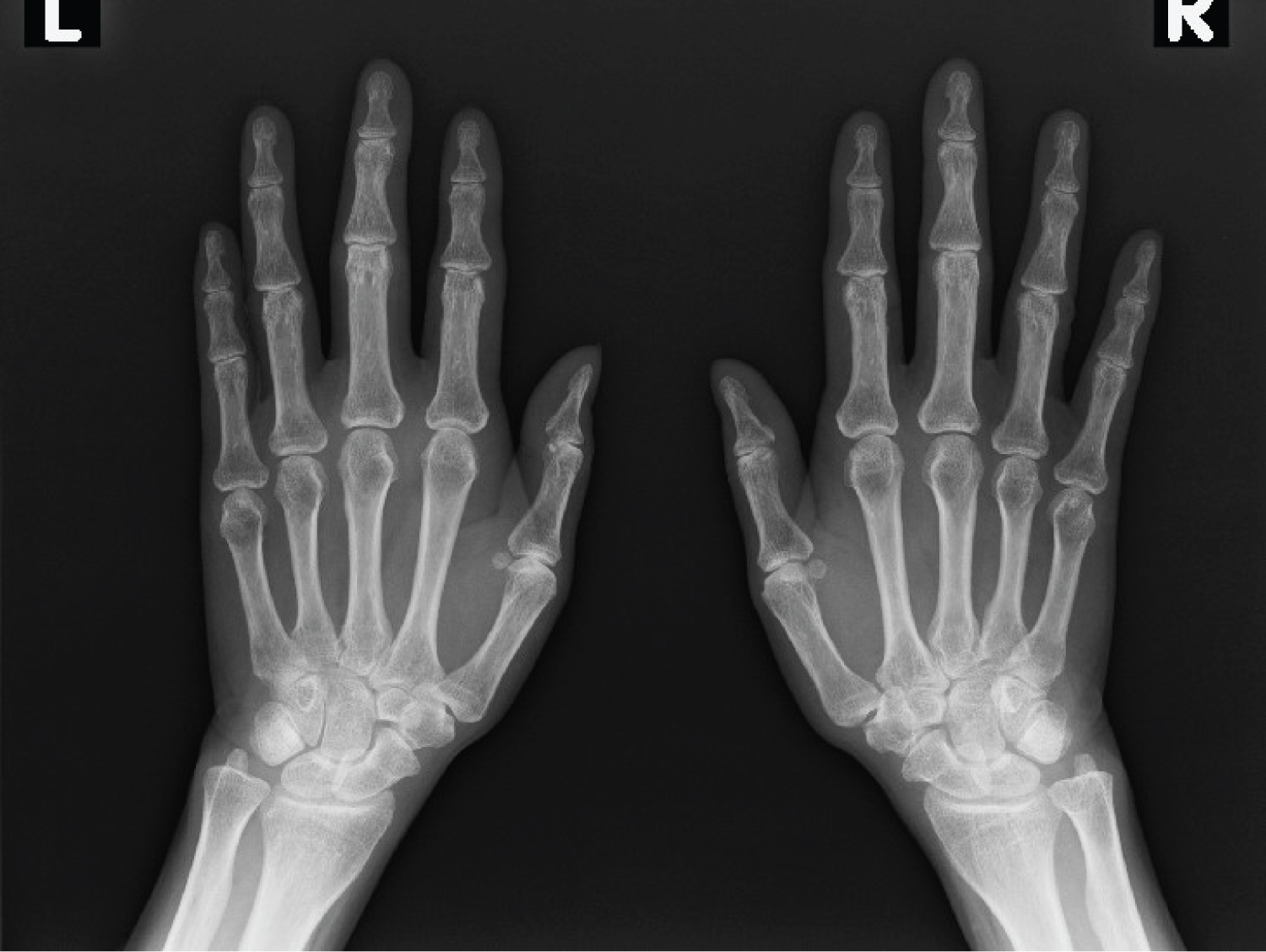 Figure 2: Anteroposterior radiograph of the bilateral hands showed no erosion and destructive change.
View Figure 2
Figure 2: Anteroposterior radiograph of the bilateral hands showed no erosion and destructive change.
View Figure 2
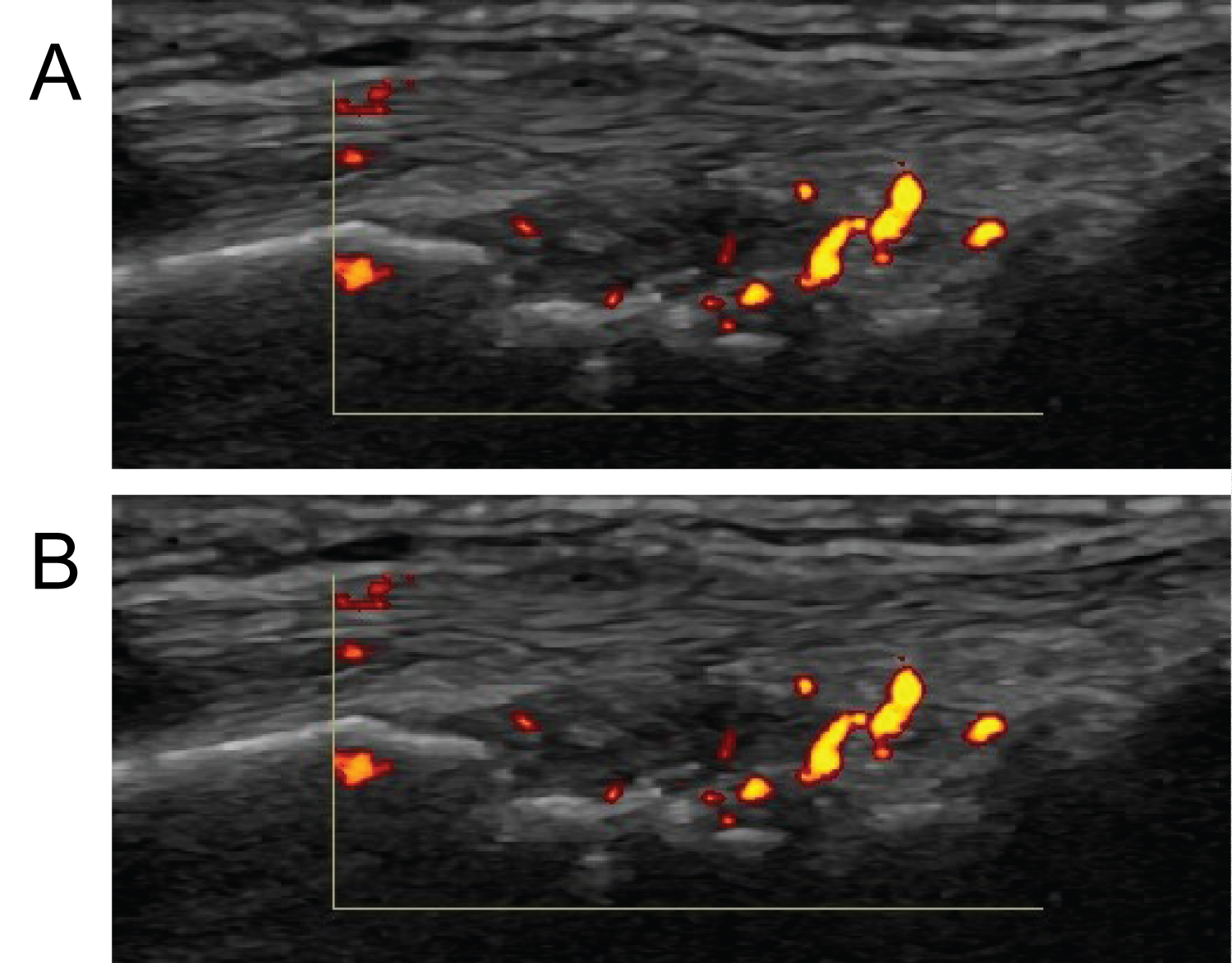 Figure 3: Longitudinal ultrasonography of the (a) right and (b) left radio carpal joints revealed hypoechoic synovial thickening associated with power doppler signals.
View Figure 3
Figure 3: Longitudinal ultrasonography of the (a) right and (b) left radio carpal joints revealed hypoechoic synovial thickening associated with power doppler signals.
View Figure 3
The results of laboratory tests on initial day include: WBC 7870/μl (Neutrophilst 66.2%), ESR 85 mm/h, CRP 2.56 mg/dl, AST 21 IU/l, ALT 17 IU/l, ALP 443 IU/l, LDH 176 IU/l, CPK 81 IU/l, Cr 0.85 mg/dl, RF 6.5 U/ml, MMP-3 77.1 ng/ml, Anti CCP antibody < 0.5 U/ml, Anti N antibody < 40. Although she has no skin menifestations and SCCH was asymptomatic during the course, she experienced prolonged poly arthritis longer than 6 weeks. As more than 10 joints were involved in the absence of autoantibodieds, she fulfilled the 2010 ACR/EULAR classification criteria (six points) [6]. Therefore she was diagnosed as Rheumatoid arthritis and we started treatment with non-steroidal NSAIDs and CsDMARDs, including Salazosulfapyridine, Bucillamine, and Methotrexate (MTX). As these durgs were not effective for her symptom, we decided to treat her with an anti-TNF α antibody agent. She received subcutaneus 50mg of golimumab every 4 weeks with 6 mg of MTX every week, which improved her peripheral arthritis without exacerbation of SCCH. As the disease activity was significantly relieved, the anti- TNF-α therapy was discontinued after the 12th shot and the dose of MTX was reduced gradually from 6 mg to 0 mg.
Although there was no evidence of recurrence for several months, she suddenly experienced severe anterior chest pain accompanied with eczima in her bilateral postero-lateral thighs (Figure 4). On physical examination, swelling of her left sternostoclavicular lesion was observed with local heat and tenderness and she was not able to elevate her left shoulder due to chest pain. However, there was no signs of recurrence of peripheral arthritis. CT scan of her left clavicle showed exuberent enlargement and hyperostosis of the left clavicle and ossification of the left sternoclaviclar and bilateral first costchondral joints (Figure 5). In addition, magnetic resonance imaging (MRI) revealed sclerotic lesion and edematous change in the bone marrow of the left clavicle (Figure 6).
 Figure 4: (a) Acne in right (b) and left lower limbs, which spread over postero-lateral thighs.
View Figure 4
Figure 4: (a) Acne in right (b) and left lower limbs, which spread over postero-lateral thighs.
View Figure 4
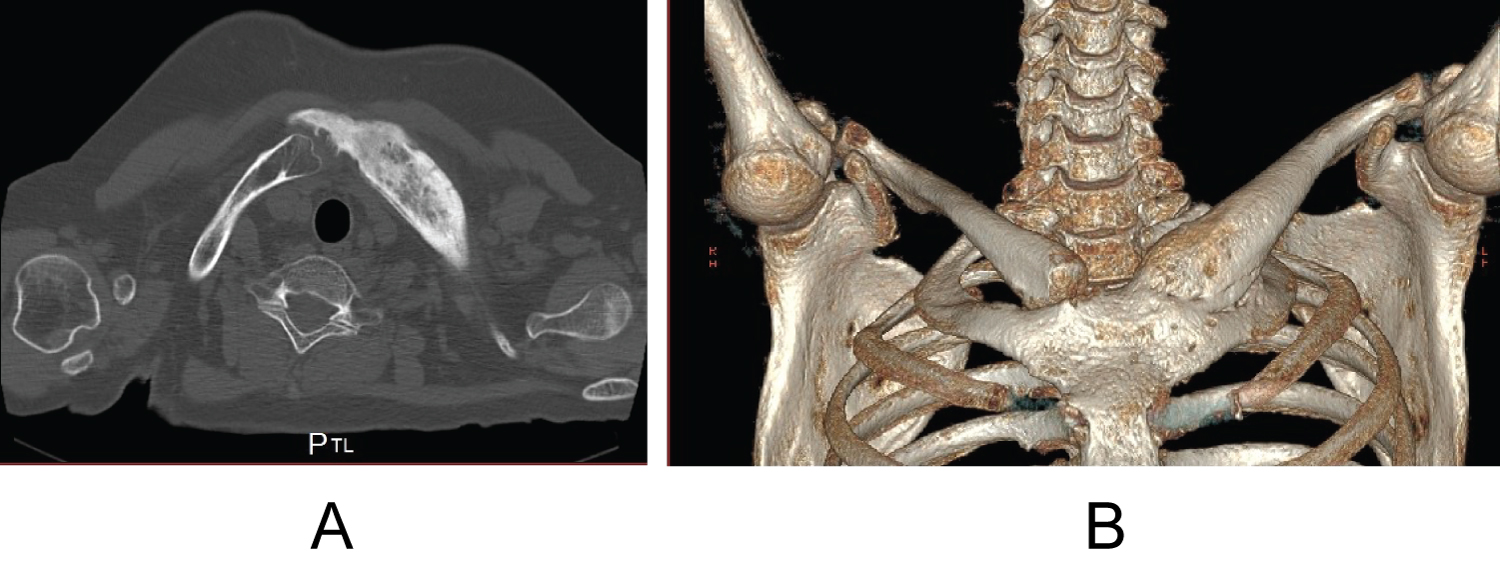 Figure 5: (a) Axial CT image (b) and 3D reconstruction image of her chest showed exuberent enlargement and hyperostosis of the left clavicle and ossification of the left sternoclaviclar and both of first costchondral joints.
View Figure 5
Figure 5: (a) Axial CT image (b) and 3D reconstruction image of her chest showed exuberent enlargement and hyperostosis of the left clavicle and ossification of the left sternoclaviclar and both of first costchondral joints.
View Figure 5
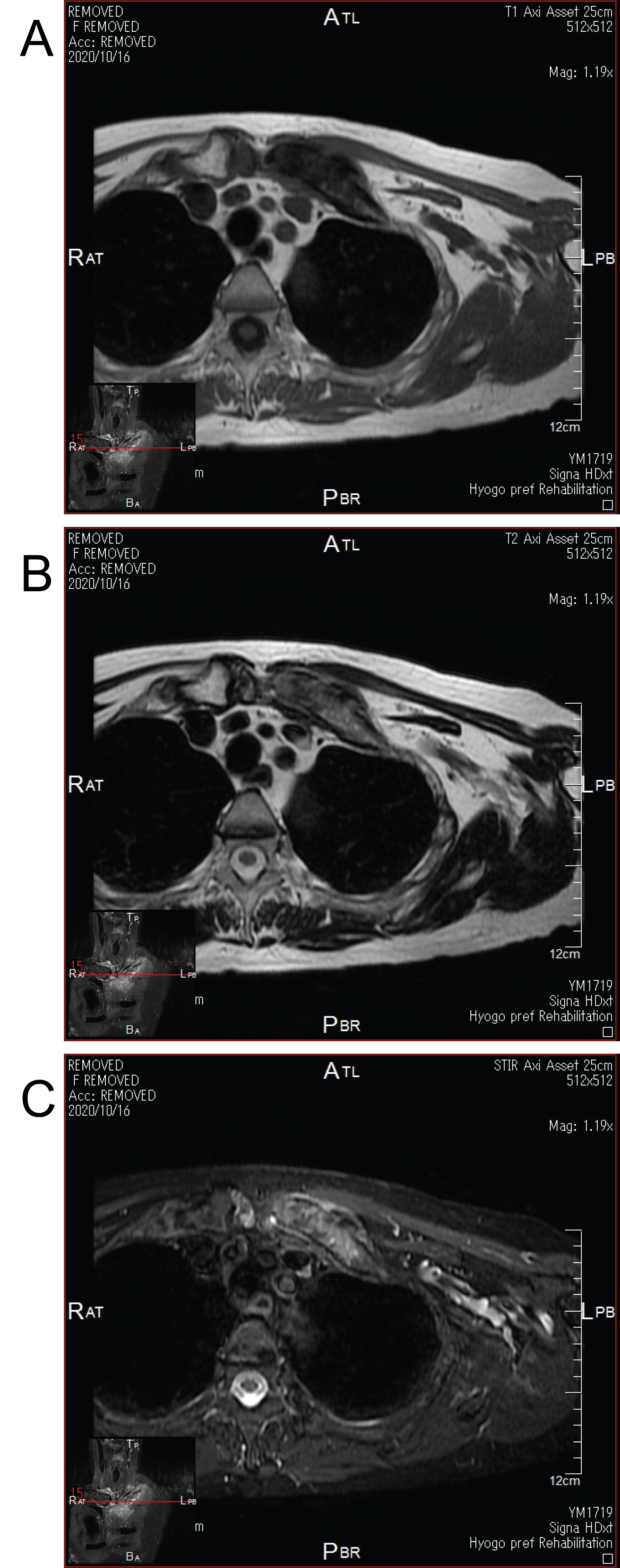 Figure 6: Axial MRI images of the left clavicle revealed sclerotic lesion associated with edematous change in the bone marrow; (a) T1 intensified image, (b) T2 intensified image, and (C) STIR image.
View Figure 6
Figure 6: Axial MRI images of the left clavicle revealed sclerotic lesion associated with edematous change in the bone marrow; (a) T1 intensified image, (b) T2 intensified image, and (C) STIR image.
View Figure 6
The results of laboratory tests include: WBC 9500/μl (Neutrophilst 71.9%), ESR 103 mm/h, CRP 13.73 mg/dl, AST 28 IU/l, ALT 44 IU/l, ALP 692 IU/l, LDH 147 IU/l, CPK 25 IU/l, Cr 0.76 mg/dl, RF 5.7 U/ml, MMP-3 60.1 ng/ml. In addition, HLA B27 antigen was negative.
As these results indicated the possibility of an infectious inflammatory condition or tumor pathology other than autoimmune diseases, open biopsy was required for the purpose of definitive diagnosis. Histopathological analysis of bone biopsy specimen showed chronic inflammation in fibrous tissue with no sign of neoplasm (Figure 7) and results of bacterial, fungal, and acid-fast bacilli culture studies were all negative. Based on these assessments, pyeogenic osteomyelits and bone tumor were excluded, thus we speculated that the relapse of SCCH was due to SAPHO syndrome.
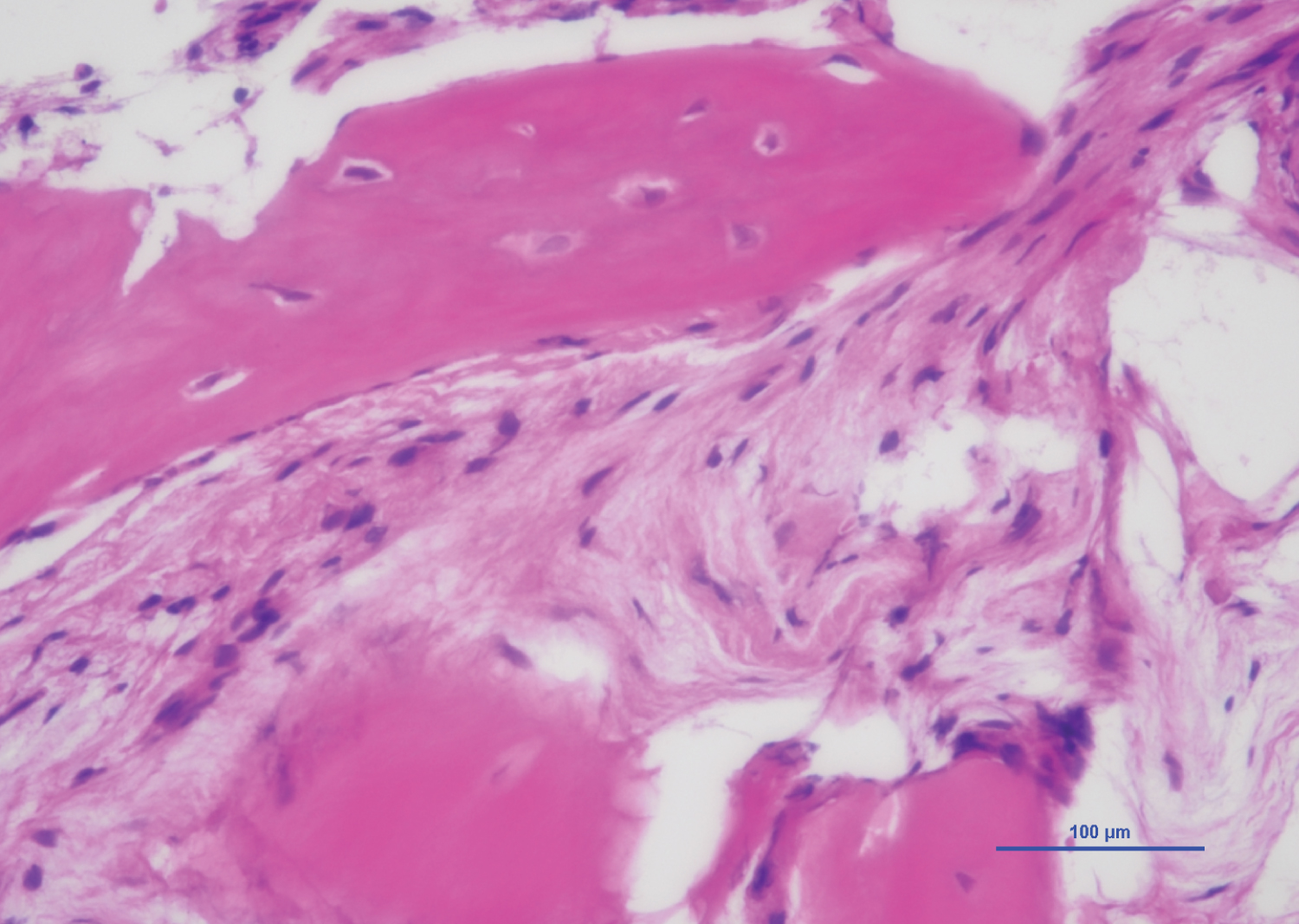 Figure 7: Photomicrograph of the excised bone on the haematoxylin and eosin staining revealed chronic inflammation in fibrous tissue with no sign of neoplasm (×100).
View Figure 7
Figure 7: Photomicrograph of the excised bone on the haematoxylin and eosin staining revealed chronic inflammation in fibrous tissue with no sign of neoplasm (×100).
View Figure 7
Before admission, she received NSAIDs initially, which were not successful in improving her anterior chest pain and skin menifestation remained. However, postoperatively, severe chest pain was gradually decreased and swelling and local heat improved along with an improvement of the skin erruption. During a 1-mouth follow-up, her skin erruption completely diappeared and levels of ESR and CRP decreased to 56 mm/h, 0.09 mg/dl, respectively. Although MMP-3 level was increased to 182.2 ng/ml postoperatively, the level decreased to 51.0 ng/ml at 3-mouth follow-up and administration of NSAIDs was discontinued. At the final follow-up visit, no clinical symptom was confirmed suggesting relapse of the disease.
SCCH causes progressive hyperstosis, fusion of the sternocostoclavicular joint, and soft tissue ossification, in most cases, associated with pain and palpable tenderness. The diagnosis of SCCH is confirmed radiographically by hyperstosis and sclerosis of the sternum with involvement of the first rib on CT [7] and a variety of conditions can produce the clinical or dadiographic findings typical of SCCH.
Recently, SCCH is more commonly considered part of SAPHO syndrome. The signs and symptoms of SAPHO syndrome are nonspecific and SCCH is 1 of the 4 inclusion criteria, which is suffcient to diagnosis of SAPHO syndrome, the most widely applyied diagnostic criteria proposed by Benhamou et al [8]. Another diagnostic critation was proposed by Kahn [9], in which isolated sterile hyperstosis/osteitis is also 1 of the 5 inclusion criteria. These criterias indicated the current case of SCCH could be diagnosed as part of SAPHO syndrome.
Although, in 70% cases of SAPHO, skin of involvement occurred within an interval of 2 years before and after the onset of rheumatological symptoms [10], our case has no history of cutaneous menifestation and SCCH was asymptomatic for long period, thus, she initially had been treated as seronegative polyarthritis due to predominant symptoms of prolonged peripheral joints.
Therefore, we started treatment with Cs DMARDs, however, they were not sufficient to improve peripheral arthritis. Although the pathogenesis of SCCH spectrum remains unknown, previous report suggested that bone lesion are caused by pathogen such as Propionibacterium acnes [11]. In our case, antibiotics were not try to be used as there were no signs of symptom related to infectious etiology during the course.
TNF alpha is a pro-inflammatory cytokine and play a critical role in several immune-mediated disorders. Various case reports described the use of anti-TNF alpha agents as a therapeutic option for the case refractory to conventional drugs and have shown efficacy on osteoarticular and cutaneous involvement [12-14]. Golimumab is a human monoclonal antibody and is indicated for treatment of rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis [15]. Comparing with other anti-TNF alpha agents, administration of golimumab is a monthly subcutaneous injection, which were preferred by our patient. In our case, combination therapy of goimumab and MTX showed significant improvement of joints menifestations, thus, halted after 12 months due to clinical remission without adverse effects.
The natural history of SCCH usually shows a relapsing-remittimg course, with relatively good prognosis. However, our patient experienced severe anterior chest pain with rapid progression of SCCH and newly appeared skin lesions without flare of peripheral arthritis. Considering the risk of infection due to immunosuppresive effct of anti-TNF alpha agents and highly elevated inflammatory markers, the differential diagnosis requires through examinations, including tissue culture and histopathological analysis. From previous reports, salmonellosis, brucellosis, tuberculosis, staphylococcas could be a cause of infection related to SCCH [16] and naoplasmas also should be considered, such as lymphoma, metastatic breast cancer, or a pancoast tumor. In the present case, these etiology were excluded and newly appeared skin cutaneous menifestation suggested that the symptom were more likely typical menifestation due to SAPHO syndrome.
It is known that the paradoxical flares of palmoplantar pustulosis or hindradentitis suppurativa irrespectively of SAPHO induced by anti-TNF alpha agents [17] and the incidence of induced psoriaris by TNF alpha inhibitors was estimated at 2.3-5% [18]. The pathophysiology of the paradixical reaction remain unknown, however, several hypothesis have been addressed, one of wich is activation of interferon gamma induced by -TNF alpha antagonist [19]. In our case, rapid progression of SCCH and skin involvement were confirmed several months after the last shot. Therefore, it is not certain whether the phenominon was related to induction or discontinue of anti-TNF alpha thearpy.
In conclusion, we heve presented a rare case of a women with rapid progression of Sternocostoclavicular hyperostosis (SCCH) after induction of clinical remission by anti-TNF-α therapy for polyarthritis. We could not provide critical information regarding curative treatment of SCCH and validity of anti-TNF alpha thearpy, which is the major limitation of the report, thus, longer follow- up period may be necessary to clarify the prognosis of the disease.
The patient provided written informed consent for publication of her data.
Not applicable.
None.