Introduction: Merkel cell carcinoma of the upper eyelid is a rare and aggressive tumor. It develops from Merkel cells present in areas with glabrous skin. It touches females more than males.
Presentation of case: A 42 years old female patient presented with a nodular painless and purplish lesion of the left upper eyelid. The diagnosis of Merkel cell carcinoma was made on histopathological examination and immunohistochemical analysis.
Discussion: Large resection in free margins associated with radiotherapy allow control of the tumor at 6 months after treatment. Propeller flap, free tarsal graft and tarsoconjonctival flap are used for full recovery of form and function of the left upper eyelid.
Conclusion: Aggressive surgical approach is mandatory to control extension of localized MCC of the eyelid which is a lymphophilic and potentially metastatic lesion.
Merkel cell carcinoma, Upper eyelid, Facial surgery, Propeller flap, Functional surgery
Merkel cell carcinoma (MCC) is a rare neuroendocrine tumour with potential aggressiveness [1]. Its mortality rate is up to 40% [2]. The basal layer of the epidermis contains Merkel cells, supposedly cells of origin for Merkel carcinoma. These cells are concentrated in touch-sensitive areas with glabrous skin.
It is known that Merkel cells are functionally linked to touch receptors for mechanical stimuli, but their exact function is not yet clearly defined. Although it is considered as a neuroendocrine tumor, no hormonal syndromes in relation to MCC have been reported [3]. Ultraviolet radiation exposure may play a role in the genesis of this type of tumor as well as polyomavirus infection [4]. Females are more prone to develop MCCs with a ratio of 2/1 [5]. The following study describes a Merkel cell carcinoma case of the palpebral region, with the clinical presentation, histopathological findings, management and follow-up characteristics.
Patient A.F., 42 years old, presented six months before a bulky and purplish nodular lesion of the left upper eyelid, with associated ptosis. Clinical examination found a swelling of 5.5 cm in diameter, consistent and solid, painless to palpation (Figure 1).
 Figure 1: Macroscopic lesion: Preoperative view of our patient presenting a nodular, purplish and exophytic mass producing mechanical ptosis.
View Figure 1
Figure 1: Macroscopic lesion: Preoperative view of our patient presenting a nodular, purplish and exophytic mass producing mechanical ptosis.
View Figure 1
No pathological lymphadenopathy was accessible to palpation especially in the cervical territories. Extension assessment (cranio-orbital and thoraco-abdominal scans) did not objectify any extension to the orbit, neck (no lymphadenopathy), chest and brain. MRI showed an hypervascularized lesion of the left upper eyelid probably of tumoral origin. There was no antecedent of cancer in her clinical history, no diabetes nor cardiovascular disease (Figure 2).
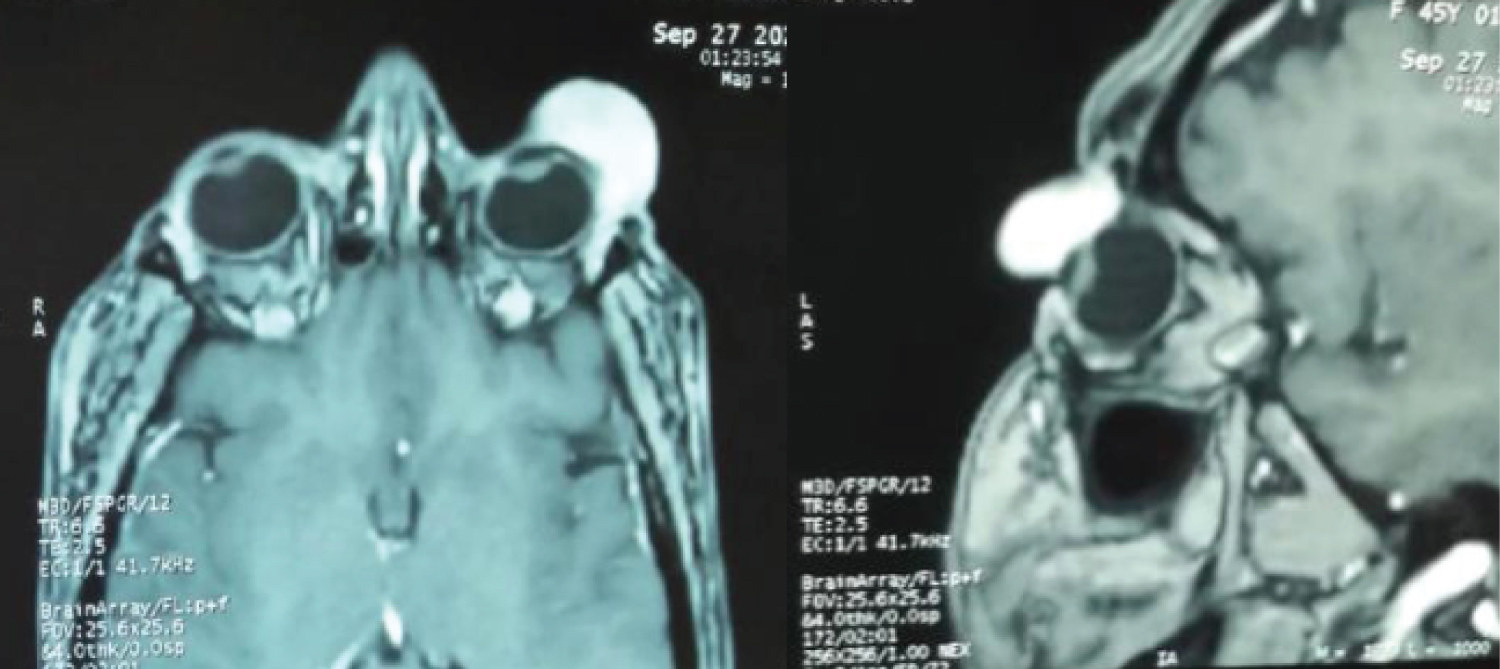 Figure 2: Horizontal and sagittal IRM: Horizontal and sagittal sections showing a hyper vascularized lesion of the left upper eyelid with suspicion of neoplastic origin.
View Figure 2
Figure 2: Horizontal and sagittal IRM: Horizontal and sagittal sections showing a hyper vascularized lesion of the left upper eyelid with suspicion of neoplastic origin.
View Figure 2
Diagnostic was made on the analysis of biopsy samples of the mucocutaneous margins of the lesion under local anesthesia. Histopathologic findings were in favour of round tumoral cells with scanty cytoplasm and hyperchromatic nuclei, surrounded by vascular septas. An immunohistochemical analysis revealed positivity for CK20, chromogranin and synaptophysin. Surgery was realized under general anesthesia. The lesion was resected extensively (1 cm of healthy macroscopic margins) with free margins (lateral, medial and deep ones) in intraoperative histopathological examination (Figure 3).
 Figure 3: Apres resection: Resection in free margins of the tumor and free tarsal graft.
View Figure 3
Figure 3: Apres resection: Resection in free margins of the tumor and free tarsal graft.
View Figure 3
The orbicularis muscle was incised with sacrifice of the superior canaliculis nasolacrimalis and preservation of the inferior canaliculis. Intraoperative examination of biopsies of the left lacrimal gland showed no sign of malignancy.
The defect area measured 4×0.5 cm in size and involved the whole surface of the upper eyelid. We used a propeller flap for reconstruction, based on the temporal superficial artery (Figure 4). Skin harvest was processed from distal to proximal with de-epidermization at its base and tunnelling. Size and limits of the lesion were marked with sterilized thread. Using a template, the flap was designed in order to fit the defect.
 Figure 4: Propeller flap based on the supratrochlear and superficial temporal arteries.
View Figure 4
Figure 4: Propeller flap based on the supratrochlear and superficial temporal arteries.
View Figure 4
The flap was spread out to the temporal area, relying on the anastomoses between supratrochleal and the frontal branch of superficial temporal arteries. The flap was entirely rotated to fill in the defect area, the donor site was directly sutured. We also used a free tarsal graft for reconstruction of the upper eyelid as a posterior lamellar replacement by sampling it from the contralateral eyelid. Leaving a 3 mm margin of tarsus along the lid margin allows to prevent entropion occurring.
As the free tarsal graft does not have a blood supply, it must be recovered by a myocutaneous flap. We used a tarsoconjontival flap from the left inferior eyelid to cover the defect. After surgery, our patient has benefited of local radiotherapy. Six months after treatment, the patient is free from disease with no clinical or radiological sign of recurrence and the eyelid has fully recovered its function (Figure 5).
 Figure 5: Postoperative view after fixing the flaps and suturing the skin in the frontal area.
View Figure 5
Figure 5: Postoperative view after fixing the flaps and suturing the skin in the frontal area.
View Figure 5
Eyelid and periocular tumors constitute about 3% of all cases of MCC. Main differential diagnosis is represented by chalazia and basal cell carcinomas [6]. This carcinoma occurs most of the time in patients over 65 years of age, Caucasians mostly and immunodeficient ones (transplanted patients, HIV infection...). The age of our patient (42 years) is under the average age at presentation.
Clinical presentation reveals a hard mass growing progressively, painless and unique, located near the palpebral margin, with a purplish color and telangiectasia. Ptosis is a common symptom [7]. This is in correlation with clinical findings in our case.
In 20-50% of the patients, preauricular and neck lymph nodes are affected at first consultation (N0 after extension assessment in our description) [8]. Distant metastases are revealed in 70% of cases, usually beneath 2 years of evolution and involve mainly bone, skin and brain [5]. Merkel carcinoma remains an aggressive tumour, its mortality surpasses that of melanoma (44% to 16% at 5 years follow-up) [9].
Several studies showed that this carcinoma expresses more often in the upper eyelid instead of the lower one (71%/21%), this is confirmed by the findings of our study. Histologically, this carcinoma present growth patterns in diffuse sheets, cells having a diameter of 15-20 μm with poorly defined contours, constituted of scanty cytoplasm, round nuclei and inconspicuous nucleolus.
The gold standard to make the diagnosis is biopsy with immunohistochemical analysis. The analysis is generally positive for low molecular weight cytokeratins such as CK20, with a perinuclear dot-like staining appearing in 85% of cases. Neuroendocrine markers such as neurofilament proteins, chromogranin is also positive. They are negative for S100 protein and high molecular weight cytokeratins [10].
Large localised excision with 5-mm free margins is recommended to control any tumor tumor when interesting the periocular region [11]. This method of resection has demonstrated to be as effective as one with 2.5 to 3 cm margins, which is used for MCCs situated elsewhere on the body [12]. Sentinel lymph node biopsy can be used for accurate staging of head and neck MCC.
Routine sentinel lymph node biopsy (SLNB) is not actually the standard of care for MCC management; however, considering the high risk for spread, achieving locoregional control is possible to achieve survival for the patients. A systematic review of SLNB in patients affected with MCC of the head and neck showed positive results in 30% of patients, and regional control was reached in 87.1% of the cases [13].
No parotidectomy was performed in this case to control local extension as the tumor was classified N0M0. Multiple studies proved improvement in locoregional control when using adjunctive radiotherapy even if surgical margins are free and in particular for large primary tumors [14]. Our patient received radiotherapy after the surgical resection. Chemotherapy for eyelid MCC is mainly used for metastatic disease [15].
MCC of the eyelid is a rare but potentially invasive tumour, even when it is non-metastatic. An aggressive surgical approach is necessary when dealing with localized MCCs of the eyelid. Adequate eyelid reconstruction allows eye protection and full recovery for the patient.
The authors do not have any commercial or proprietary interest in the products used in this study.