Epidermolysis bullosa (EB) is a mucocutaneous disorder characterized by fragility of skin and mucosal membranes to the mechanical stress resulting formation of blisters, erosions and scarring. Their vulnerability needs certain attention and anesthetic management plan to perform anesthesia requiring procedures and surgeries without complications. In our case, a patient with EB had undergone an esophageal dilatation procedure. We present an anesthetic management strategy for these patients.
Epidermolysis bullosa, Anesthetic management, Difficult airway, Trauma
Epidermolysis bullosa (EB) is a mucocutaneous disorder of dermoepidermal or intradermal disruption characterized by fragility of skin and mucosal membranes to the mechanical stress resulting formation of blisters, erosions and scarring later in certain subtypes. EB can be classified into four major subtypes based upon the level of disruption: EB simplex, Junctional EB, Dystrophic EB, and Kindler EB [1]. Dystrophic subtype is caused by mutations in the COL7A1 gene which is responsible of coding alpha-1 chain of type VII collagen that anchors epidermal basement membrane to the dermis [2]. Its distinctive feature amongst the group is scarring healing of blisters and erosions. This leads to scarring-related deformities such as pseudo-syndactyly, esophageal webs and strictures, microstomia etc.
Anesthetic management of these patients can be challenging as all the practices done perioperatively (transporting, positioning, monitoring, airway management etc.) may cause harm to patient. To minimize this harm, all these steps should be optimized to patient's needs.
Herein, we present a case report of anesthetic management of an esophageal dilatation procedure for an 18-year-old female with dystrophic EB.
An 18-year-old female diagnosed with dystrophic EB consulted for esophageal dilatation procedure. She was suffering from dysphagia due to upper esophageal stricture which had been confirmed by esophagography. Her weight was 42 kg with height of 157 cm. She had history of multiple esophageal dilatations between ages of 6 and 14, microstomia operation. Both of her hands had pseudo-syndactyly deformities (Figure 1). Her mouth opening was narrow (Figure 2). Mallampati score was 4. Since laboratory studies showed iron deficiency anemia, she was consulted to hematology. After her intravenous (IV) iron replacement therapy, operation was scheduled. Her oral and written consent was obtained.
 Figure 1: Pseudo-syndactyly deformities on both hands.
View Figure 1
Figure 1: Pseudo-syndactyly deformities on both hands.
View Figure 1
 Figure 2: Narrowed mouth opening.
View Figure 2
Figure 2: Narrowed mouth opening.
View Figure 2
In operating room, she moved from sketcher to operating table without assistance. All contact points were padded. Her right arm was wrapped with cotton gauzes and a blood pressure cuff was placed over it. Soft silicone adhesive dressings (Mepitel® One) were used with caution to secure monitoring units including the pulse oximeter probe, the ECG electrodes. All vital signs were normal. After a tourniquet applied just below left knee over a cotton gauze, a 24-Gauge IV cannula inserted under guidance of ultrasonography and secured with the silicone dressing (Figure 3).
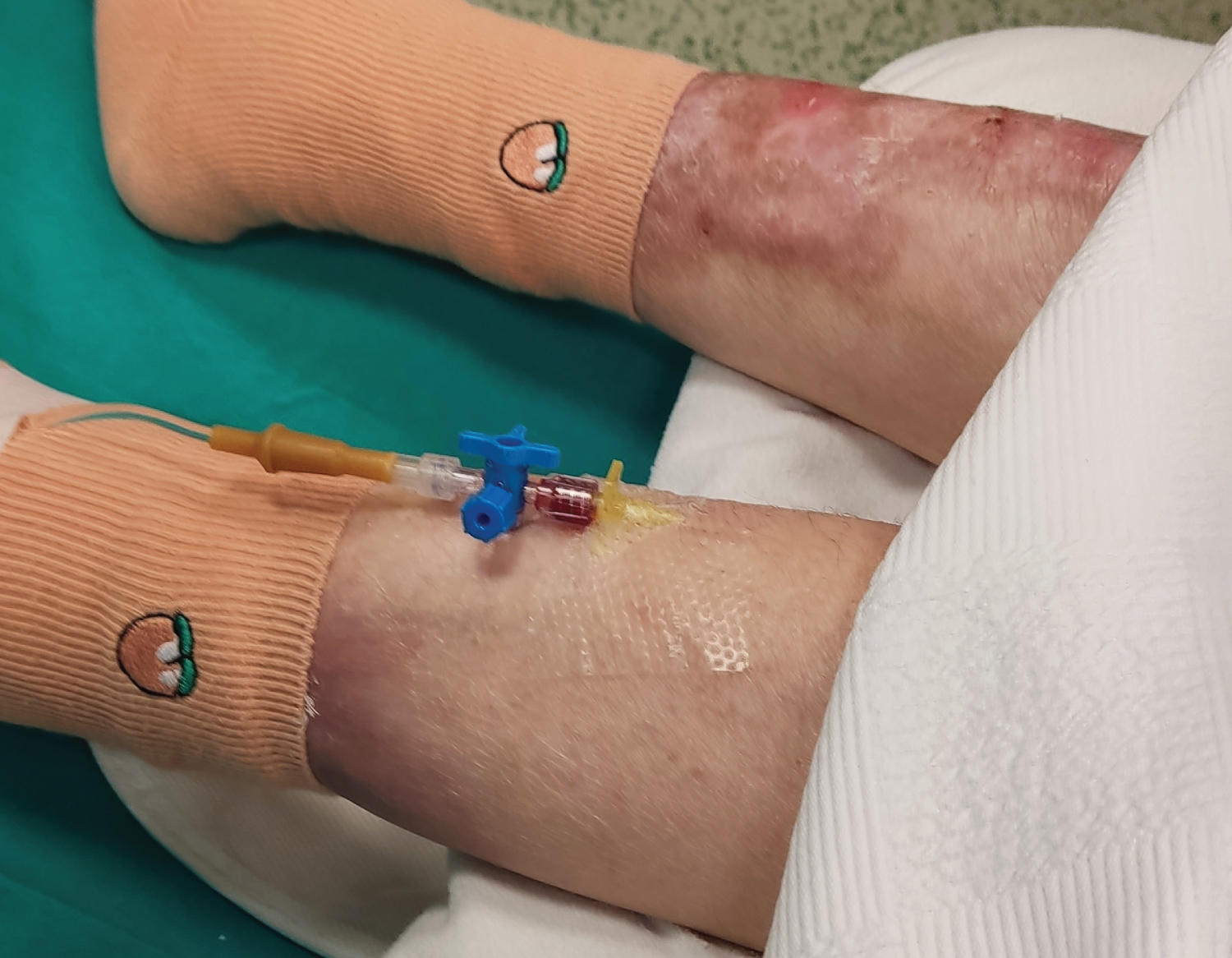 Figure 3: 24-Gauge IV cannula inserted and secured with silicone dressing.
View Figure 3
Figure 3: 24-Gauge IV cannula inserted and secured with silicone dressing.
View Figure 3
Since her mouth opening was narrow due to repeating peroral erosions healing with scarring, fiber optic intubation preparation was done and kept ready in operating room. After induction with Propofol 2 mg/kg, Lidocaine 1 mg/kg, Fentanyl 1 mcg/kg and Rocuronium 0.9 mg/kg; here, eyes were applied ophthalmic ointments. After 3 minutes of preoxygenation with a face mask, video laryngoscopy was used for intubation. The blade was lubricated with Vaseline. A 6.0 mm endotracheal tube with stylet inserted into trachea under the guidance of video laryngoscopy (Figure 4). To achieve glottic view and sufficient mouth opening, manipulations of laryngoscope caused pressure on the hard palate resulting hemorrhage which then controlled with applying pressure over a gauze. Endotracheal tube was secured with the silicone dressing (Figure 5). Maintenance of anesthesia was provided with sevoflurane administration and remifentanil 0.05-0.1 mcg/kg/min IV infusion. Methylprednisolone 1 mg/kg was given.
 Figure 4: Insertion of endotracheal tube with stylet into trachea.
View Figure 4
Figure 4: Insertion of endotracheal tube with stylet into trachea.
View Figure 4
 Figure 5: Silicone dressing.
View Figure 5
Figure 5: Silicone dressing.
View Figure 5
A mouthpiece for endoscopy insertion was placed. The procedure was done without complications. After discontinuation of sevoflurane and remifentanil, Sugammadex 2 mg/kg was given for reversal of neuromuscular blockade. Oropharynx was suctioned carefully. As return of spontaneous breathing achieved in 5 minutes, she was extubated awake after following commands and transported to the post-anesthesia care unit. Her vital signs were normal. There were no signs of airway edema, obstruction. She was discharged from hospital on the same day.
Anesthetic management of these patients possess certain risks to these patients and need modifications to our ordinary practices. Due to their fragile skin, special care begins with transport and positioning of patients. While being moved between stretchers/operating table, care should be taken to avoid friction on skin, wrinkle/fold formations under the patient. If suitable, it may be safer to move themselves to the table without assistance [3]. All pressure contact points should be padded. With extensive erosions on skin, they're prone to hypothermia. Underbody blankets and forced-air warming devices can be used without direct contact to maintain normothermia.
Monitoring can also be challenging. There might be no suitable fingers or toes to place a pulse oximeter due to deformities. Adhesive extensions may cause harm. Choosing of probes and fixation method vary by patient. Clip-on pulse oximeters are preferrable [4]. ECG lead electrodes should be placed without direct contact of their adhesives to the skin. After removing adhesives, they can be placed under patient to be held in place with weight. Noninvasive blood pressure cuffs can be applied over cotton gauzes [5].
As the skin has extensive erosions all over the extremities, vascular access may be difficult to obtain. To avoid multiple attempts and further injury, the best available peripheral veins should be cannulated by experienced ones. Tourniquets can be applied over a cotton padding. Occasionally, central venous access may be required. Catheters, cannulas can be secured with special tapes, sutures.
Airway management can also be challenging in these patients. In severe cases, peroral and intraoral lesions heal with scarring which then results with microstomia, ankyloglossia (caused by lingual frenulum tethering tongue to floor of mouth). Oral deformities, esophageal strictures lead to dysphagia, poor and painful oral intake resulting with malnutrition and anemia as it was for our patient [4]. Since mucosal membranes are prone to injury as well, any trauma can cause serious complications both intraoperatively and postoperatively. Mucosal damage can be resulted as blister formation, hemorrhage, edema causing airway obstruction. For minimal friction all airway instruments should be well lubricated. Airway manipulations including firm face mask application, jaw thrust, oro/nasopharyngeal airway insertion can lead to frictions and erosions [5].
Airway management strategies for sedation or general anesthesia cases vary based upon surgery type and duration, anticipated complications, risk of aspiration. Facemask ventilation with measures taken to reduce friction can be sufficient for short procedures not involving airway or upper gastrointestinal tract. Well lubricated, one size smaller laryngeal mask airways (LMA) are of reliable choice for most procedures. When endotracheal intubation indicated, endotracheal tube size should be half or one size smaller than formulas' suggestion. As mouth and neck contractures may dictate, all available difficult airway strategies like fiberoptic, video laryngoscope should be ready to use in operating room. From positioning patient's head to laryngoscope manipulations to achieve glottic view may cause skin and mucosal damages. (Bowen, Nandi) These should be minimized by lubricating all possible interfaces and changing into less manipulation needed than direct laryngoscope techniques such as fiberoptics and video laryngoscopes.
Patients with EB may need surgeries or procedures for various reasons whether related to the disorder. Their vulnerability to any kind of mechanical stress needs certain attention and anesthetic management plan to perform these procedures without major complications. Beginning with decision to procedure, every anticipated mechanical interaction with environment, personnel, equipment, application to be foreseen and thoroughly optimized to avoid injury.
Conflict of interest: None.
Financial disclosures: None.
The authors declare no competing interests.
EK, BG, DK read and sorted out the relevant literature, and collected the medical records. EK wrote the article. FL, NC supervised and revised the paper. All authors read and approved the final manuscript.
This research received no external funding.