• Cutaneous squamous cell carcinoma (cSCC) is the second common non-melanoma skin cancer and primarily treated with surgical resection [1]
• Patients with locally advanced (LA) or metastatic cSCC may not be candidates for curative surgery or radiation, and long-term prognosis is poor for metastatic disease [1-3]
• Pembrolizumab monotherapy is approved in certain countries, including the US, for treatment of LA or recurrent/metastatic (R/M) cSCC not amenable to surgery based on results from the open-label phase 2 KEYNOTE-629 trial (NCT03284424) [4]
○ Objective response rate (ORR) was 50.0% (95% CI, 36.1-63.9) with 9 (16.7%) complete responses (CRs) in the LA cohort and 35.2% (95%CI, 26.2-45.2) with 11 (10.5%) CRs in the R/M cohort
○ 69.2% of patients in the total population experienced a treatment-related adverse event (AE) and 11.9% experienced a grade 3-5 treatment-related event
• Present updated efficacy and safety results for pembrolizumab in LA and R/M cohorts of KEYNOTE-629 with an additional 38 months of follow-up
Figure 1
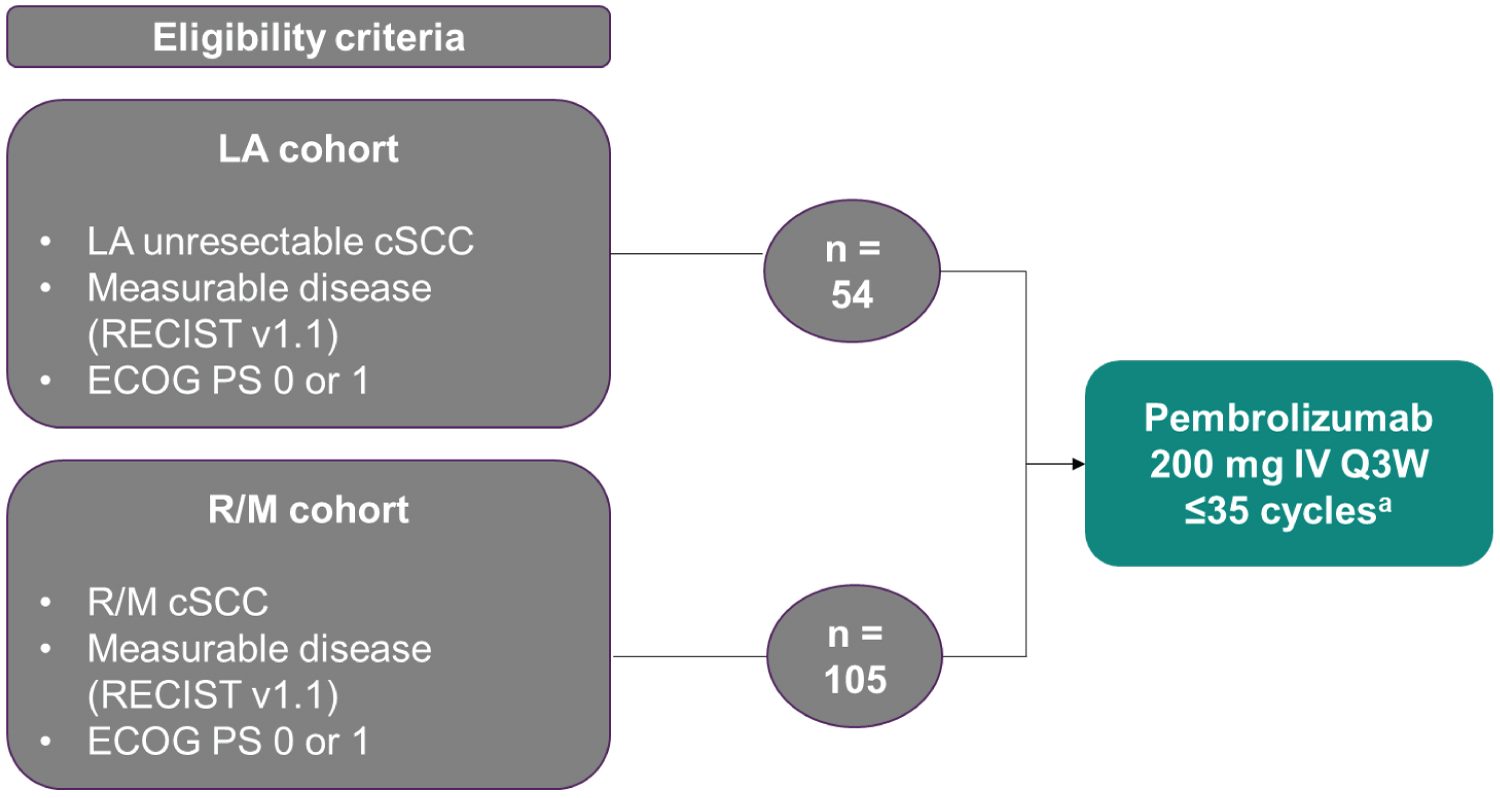 Figure 1: Study design.
Figure 1: Study design.
ECOG PS: Eastern cooperative oncology group performance status; IV: Intravenously; Q3W, every 3 weeks.
aPatients who discontinued treatment after achieving complete response may be eligible to receive an additional 17 cycles of pembrolizumab if disease progression occurred.
View Figure 1
• Efficacy and safety were assessed in all patients who received ≥ 1 dose of study treatment
• The primary end point was ORR per RECIST v1.1 by blinded independent central review (BICR)
• The secondary end points were disease control rate (DCR; defined as CR + partial response (PR) + stable disease ≥ 12 weeks), duration of response (DOR) and progression-free survival (PFS) per RECIST v1.1 by BICR, overall survival (OS), and safety
• DOR was assessed in all patients with a confirmed CR or PR
• 95% CIs for ORR and DCR were calculated using the exact binomial Clopper-Pearson method
• Event rates over time for DOR, PFS, and OS were estimated using the Kaplan-Meier method
• Median time from first dose to the data cutoff date of September 13, 2023, was 52.4 months (range, 47.6-56.9) for the LA cohort, 64.7 months (range, 62.1-69.5) for the R/M cohort, and 63.1 months (range, 47.6-69.5) in the total population (Figure 2, Figure 3, Figure 4, Figure 5, Table 1, Table 2 and Table 3).
 Figure 2: Patient disposition.
Figure 2: Patient disposition.
PD: Progressive Disease
View Figure 2
 Figure 3: Kaplan-Meier estimates of DOR in patients with a confirmed response per RECIST v1.1 by BICR in the LA cSCC cohort, R/M cSCC cohort, and total population.
View Figure 3
Figure 3: Kaplan-Meier estimates of DOR in patients with a confirmed response per RECIST v1.1 by BICR in the LA cSCC cohort, R/M cSCC cohort, and total population.
View Figure 3
 Figure 4: Duration of treatment and time to response in patients with a confirmed response per RECIST v1.1 by BICR in the (A) LAcSCC cohort and the (B) R/M cSCC cohort.
View Figure 4
Figure 4: Duration of treatment and time to response in patients with a confirmed response per RECIST v1.1 by BICR in the (A) LAcSCC cohort and the (B) R/M cSCC cohort.
View Figure 4
 Figure 5: Kaplan-Meier estimates of (A) PFS per RECIST v1.1 by BICR and (B) OS in the LA cSCC cohort, R/M cSCC cohort, and total population.
Figure 5: Kaplan-Meier estimates of (A) PFS per RECIST v1.1 by BICR and (B) OS in the LA cSCC cohort, R/M cSCC cohort, and total population.
NR: Not Reached
View Figure 5
Table 1: Baseline characteristics. View Table 1
Table 2: ORR per RECIST v1.1 by BICR. View Table 2
Table 3: AE summary. View Table 3
• With an additional 38 months of follow-up (median follow-up 63.1 months in the total population), pembrolizumab monotherapy continued to demonstrate durable antitumor activity in patients with LA or R/M cSCC
• In the current analysis, ORR, median PFS, and median OS are consistent with the initial analysis at a median time from first dose to data cutoff of approximately 15 months [4]
• One additional patient in the LA cohort achieved a CR since the last data cutoff
• Responses were durable, with a median DOR of 52.5 months and 61.2% of responders in the total population having extended responses that lasted ≥ 36 months
• The safety and tolerability of pembrolizumab remained manageable
• These findings continue to support the use of pembrolizumab monotherapy in patients with LA or R/McSCC
The authors thank the patients and their families and all investigators and site personnel. Medical writing and/or editorial assistance was provided by Maxwell Chang, BSc Hons, and Robert Steger, PhD, of Apothe Com (Yardley, PA, USA). This assistance was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Funding for this research was provided by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Contact the author at emunoz@vhio.netfor questions and comments.
Copies of this poster obtained through Quick Response (QR) Code are for personal use only and may not be reproduced without permission from ASCO ® and the author of this poster.
Presented at the ASCO Annual Meeting; Chicago, Illinois; May 31-June 4, 2024.
Copyright © 2024Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.