Background: Disclosure has become an essential part of the care for HIV-infected children in antiretroviral therapy clinics. One of the greatest psychosocial challenges that parents and caregivers of infected children face is the disclosure of Human Immunodeficiency Virus positive status to their infected children.
Objectives: The aim of this study was to assess the magnitude of disclosure status and associated factors among caregivers of children on antiretroviral therapy in Addis Abeba, Ethiopia 2021.
Methods: A hospital based cross sectional study design was conducted at government hospital under A.A city administration from Nov to Feb 2021. Systematic random sampling technique was used to select, care giver/parents. Data was collected by interview using pre-test structured questionnaires. Descriptive statistics were used to illustrate the means, standard deviations, and frequencies of the study variables. Bivariate logistic regression was performed and those variables whose p-values less than or equal to 0.25 was fitted into multiple logistic regression and P-values less than or equal to 0.05 was considered as statistically significant.
Results: With 96.8% response rate, the disclosure status of this study is high with One hundred sixty-seven (53.9%) of the children knowing their positive HIV status. Factors which have showed to increase the likelihood of HIV disclosure status are children in age group 10-15 years were [AOR = 1.5 (3.071-5.256)], children who were on ART from 6 to 13 years were [AOR = 3 (1.093-1.501)], children with good treatment adherence AOR [2(1.241-3.487] and children who got adequate advice from health care provider were [AOR = 2.1 (5.728-6.527)].
Conclusion and recommendation: Although the prevalence of HIV-positive status disclosure to infected children in Addis Ababa is high (53.9%) and has shown an improvement compared to previous findings, it still indicates that there is still much work to be done. The main reasons for disclosure were because of repeated question from the child. Children's' young age and fear of discrimination was the main reason for non-disclosure of their HIV status. The study recommends that health care workers should give age-appropriate counselling, support, and work together with caregivers on the processes of disclosing their diagnostic result to infected children. It also recommends that Ministry of Health, stakeholders (NGO's) and policy makers to give special emphasis on health care institutions and health care workers that deal with these situations by providing them resources and guidelines.
Human immunodeficiency virus status disclosure, Children, Caregivers, Highly active anti-retroviral therapy, Ethiopia
AIDS: Acquired Immuno Deficiency Syndrome; ART: Anti-Retroviral Therapy; AOR: Adjusted Odds Ratio; DHS: Demographic and Health Survey; ETB: Ethiopia Birr; FMOH: Federal Ministry of Health; HAART: Highly Active Anti-Retroviral Therapy; HCW: Health Care Workers; HIV: Human Immunodeficiency Virus; MOH: Ministry of Health; MTCT: Mother to Child Transmission of HIV; NGOs: Non-Governmental Organizations; PMTCT: Prevention Mother to Child Transmission; UNAIDS: United Nation for HIV AIDS; VCT: Voluntary Counselling and Testing; WHO: World Health Organization
Human immunodeficiency virus Acquired immune deficiency syndrome has created an enormous challenge to mankind since its recognition; People living with HIV (PLWH) account 36.7 million worldwide; of this 32.1 million are adults and 3.3 million Children under 15 years of age in 2015 [1]. Almost 91% of all HIV infected children live in sub-Saharan Africa [2] and about 160,000 living in Ethiopia; around 21,686 are taking ART treatment [3]. Although there has been significant improvement in ART coverage among children, it is still low compared to adults. At the end of 2016, it was estimated that only 43% of children aged < 15 years living with HIV/AIDS were receiving ART [4].
As highly active antiretroviral therapy (HAART) becomes increasingly available in low resource settings, infected children are living longer [5]. With increased survival, one of the greatest challenges that parents and caregivers of HIV-infected children face is the disclosure of HIV-positive status to their infected children, among these difficult issues that families with HIV infected children face are when and how to talk about HIV to their children. Disclosure is contingent on the caregiver’s acknowledgement of the illness, the readiness to disclose, and child’s cognitive skills and emotional maturity [6].
Human immunodeficiency virus Acquired immune deficiency syndrome disclosure becomes more significant because of the multiple benefits for the children and their caregivers [7]. Disclosure is related to good or improved adherence to ART medications and influences children's participation in healthcare decision-making. It also enables children to understand HIV infection and make sense of their disease-related experiences as well as the importance of adherence [8]. Children have the right to know their HIV status and disclosure of it after diagnosis is crucial for their wellbeing. Factors affecting lack of disclosure include the depth of information to be shared, the manner and time of disclosure, which caregivers and healthcare workers should consider [9]. Early disclosure is more appropriate than immediate and unplanned disclosure upon entrance into the adult clinic, and also helps to reduce HIV transmission [10].
In 2011, WHO released a guideline on HIV status disclosure in children recommends that disclosure process should start when the child is 6-years-old and be completed at the age of 12 years [11]. The prevalence of disclosure of HIV status to children in sub-Saharan Africa is not well described. The limited existing studies from low- and middle-income countries suggest that disclosure is still relatively rare. Evidence from a recent systematic review shows that the majority of the children less than 18 years living with HIV in resource limited settings, including sub-Saharan Africa, are not aware of their own HIV status [12]. In Ethiopia, studies showed that the prevalence of disclosure among caregivers’ of children varies from 16.3 to 39.5% [13-15]. In addition to the low frequency of disclosure in Ethiopia, little is known about the associated factors of HIV disclosure in school-aged children.
HIV status disclosure improves children's health and disease progression, enables them to understand their HIV infection, improves adherence to ART medications, and enhances long-term care quality. Understanding caregivers' reasons and experiences during HIV diagnosis disclosure is crucial for preventing non-disclosure to children [8,16,17].
There is a general consensus among researchers that caregivers especially in developing countries remain reluctant to disclose the HIV diagnosis to HIV infected children and the frequency of disclosure of HIV status to infected children has been found to be low in resource-limited settings, only a few children with PHIV+ know their HIV-positive status furthermore, little is known about pediatric HIV disclosure about the complex issues of when and how to tell a child about the HIV diagnosis. Caregivers are also presented with set of challenges including deciding on what is in the child’s best interest and when, why and how information about his/her HIV positive status should be shared with him/her. They are also reluctant to disclose the HIV positive status to their children for fear of social rejection and isolation, parental sense of guilt, and fear that the child would not keep diagnosis to themselves [18-20]. Understanding magnitude and associated factors of HIV status disclosure to HIV/AIDS infected children may therefore help in preparation of implementation strategies to improve disclosure processes and the quality of life of children living with HIV/AIDS in Addis Ababa.
Even though the growing evidence of the benefits of disclosure from developed countries disclosure to HIV infected children in developing countries continues to be delayed until older childhood, Paediatric HIV providers generally believe that disclosure is important for helping children understand the need for ART and for creating trusting relationships that facilitate adherence. Thus, this study assessed the magnitude of HIV status disclosure and its associated factors among caregivers of children on follow up of HAART at selected governmental hospital in Addis Ababa.
A hospital-based cross-sectional study design was conducted from the 1st of December to the 20 th of February 2021 in two public hospitals providing pediatric ART services in the Addis Ababa city administration. Addis Ababa is the capital of the Addis Ababa city administration's health bureau, which provides pediatric ART. Addis Ababa is the capital city of Ethiopia and the diplomatic capital of Africa. It is located in the central part of the country. Addis Ababa covers an area of 527 km 2 . Based on the 2007 National Census and using population projections for 2017, Addis Ababa has an estimated total population of over 4 million. There are a total of 99 health centers, 12 governmental hospitals, 36 private hospitals, 700 clinics, and 35 nongovernmental organizations currently serving the 2715 children under 15 on HAART in Addis Ababa. From November to February 2021, this research was carried out in Addis Abeba. All caregivers of HIV-positive children aged 6 to 15 years are receiving ART services at the pediatric ART clinics of four (4) Addis Abeba city administration hospitals. Caregivers of children infected with HIV aged 6-15 who were on care and support follow-up in a pediatric ART clinic during the study period were included in this study.
The sample size of study participants was determined using the single population proportion formula, and the following assumptions were used for sample size calculation: 40% of HIV/AIDS disclosure among children living with HIV/AIDS is taken as 0.4 [21], 5% of the marginal error finite population correction formula is applied after the initial n, 10% non-response rate, and considering the design effect. In a given year, 2415 patients attend chronic ART care follow-up, resulting in a final sample size of 320.
The four public hospitals in Addis Ababa City Administration were selected using simple random sampling techniques, and a systematic random sampling technique was used for care providers. The number of respondents was proportionally allocated to the selected hospitals, and all eligible caregivers were interviewed during their children's monthly follow-up visits at each hospital sampling technique from the records of each selected facility.
Disclosure refers to when the caregiver says that the child knows his or her HIV/AIDS diagnosis regardless of who told him or her.
Non-disclosure: When the caregiver stated that the child is unaware of his or her infection or when the caregiver was unsure whether the child was aware of his or her status.
Caregiver: A person who lives with the child, participates in the child’s daily care, and is the most knowledgeable about the child’s health. They were either the child's biological parents or guardians, such as an aunt, or an adoptive parent acting as surrogate parents.
Child: According to the Convention for Child Rights, to which Ethiopia is party, "as child means every human being below the age of eighteen years." But for this study, a child is defined as being between the ages of 6 and 15, in line with HIV/AIDS-related publications (e.g., the UNAIDS AIDS in Ethiopia report), which used 15 years of age as the cut-off point for children. Furthermore, people over the age of 15 can access voluntary counseling and testing with their own consent and do not need parental permission to learn their HIV status [3,22].
The data was entered and cleaned using EPI Info version 7.2.1.0 and then exported to SPSS version 25 statistical software for analysis. Statistical tests and measures of association were used as necessary. Binary logistic regression was performed, and those variables whose 𝑝-values were less than or equal to 0.25 were fitted into multiple logistic regression and P-values less than or equal to 0.05 were considered statistically significant. A P-value less than 0.05 was used for identifying statistically significant variables multivariate analysis. Thus, the independent effect of each explanatory variable on the outcome variable was determined while controlling for others.
Out of 320 sampled respondents in the selected hospitals during the study period, 310 agreed to participate, and the response rate was 96.8%. The respondents were from Yekatit 12 Hospital, 200 (64.5%), and Zewditu General Hospital, 110 (35.4%).
Approximately 62.9 percent of the 310 caregivers of children aged 6 to 15 who participated in the study were female. Most of the respondents (39.5%) were within the age range of 36-45 years. About 103 of the respondents had a secondary school educational status. One hundred forty-four of the respondents were married, and 132 of them were privately employed. Most of the respondents (57.1%) had a monthly income of $1,000-5,000 and 58.7% had a family size of 1-5, and nearly 71% of caregivers were the biological parents of the children for whom they provided detaining care (Table 1).
Table 1: Information on socio-demographic characteristics of caregivers', Addis Ababa, Ethiopia, 2021. View Table 1
The majority of HIV-positive children were boys (53.2%), 70.3% were between 10-15 years-old, 73.9% attended primary school, 69.7% were living with their biological parents, and one hundred twenty-four lost parents see details in Table 2.
Table 2: Socio-demographic characteristics of the child, Addis Ababa, Ethiopia, 2021. View Table 2
Among the caregivers, 189 (61%) are HIV positive. Among those, 127 (41%) of them have disclosed their status to their partner, and 183 (59%) of them have started ART. One hundred thirty-two (42.6%) of the children were referred from PMTCT, and 276 (89%) were between the ages of one and six when they were diagnosed. majority (64.8%) of them had stage one HIV, with 20 (6.5%) of the children having a recent > 500 CD4 count. From those who started ART, 261 (84%) started ART between the ages of 1 and 5, and 168 (54.2%) children had an additional medication of Bactrim. Sixty-nine percent have good adherence to the medication, 127 (41% of the children affected) have been affected by opportunistic disease, and 70 (22.6%) have been hospitalized. 238 (76%) of the participants have discussed disclosure issues with their health care providers, and 48 (15.5%) have received support from governmental and non-governmental organizations see details in Table 3.
Table 3: Clinical characteristics of caregivers and children in Addis Ababa, Ethiopia, 2021. View Table 3
According to the study's findings, 167 caregivers (53.9%) disclosed their HIV positive status to their child him/herself (Figure 1).
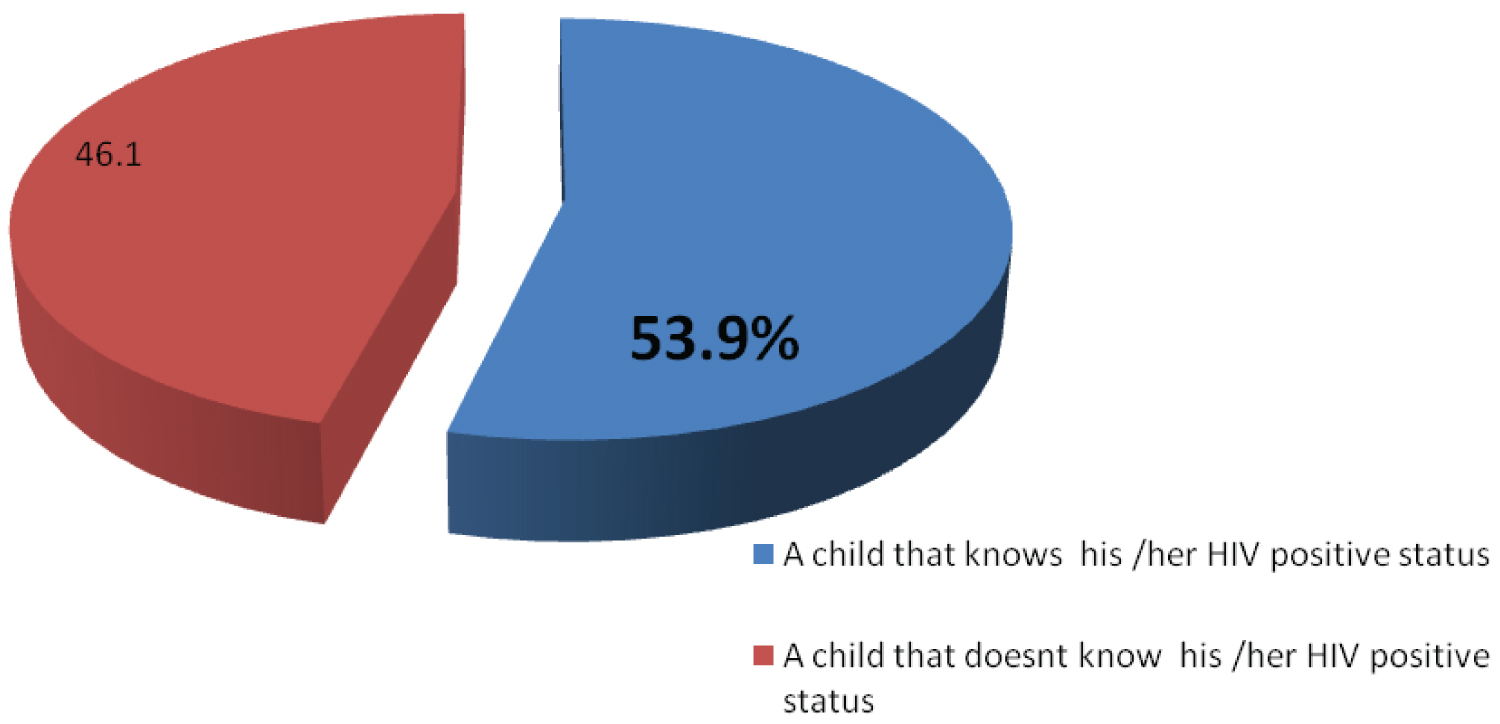 Figure 1: HIV positive status disclosure among HIV positive children, Addis Ababa, Ethiopia, 2021.
View Figure 1
Figure 1: HIV positive status disclosure among HIV positive children, Addis Ababa, Ethiopia, 2021.
View Figure 1
Forty-four percent were disclosed to them between the ages of seven and twelve. Seventeen percent were disclosed to them by a health professional. A total of 115 children whose status was not disclosed believed it should be disclosed after the age of 18, and 58 percent of caregivers believed or expressed concern that their child would be stigmatized (Table 4).
Table 4: HIV positive status disclosure among HIV positive children in AddisAbaba, Ethiopia, 2021. View Table 4
One hundred sixty-seven of the study participants have told them about the children's HIV status. Twenty-one percent disclosed it because of repeated questions from the child, while the rest (79%) disclosed it because the child was thought to be mature enough to take or adhere to medications, to know about his or her disease condition, to take care of him or herself and prevent disease transmission, to share responsibility, and to get relief (Figure 2).
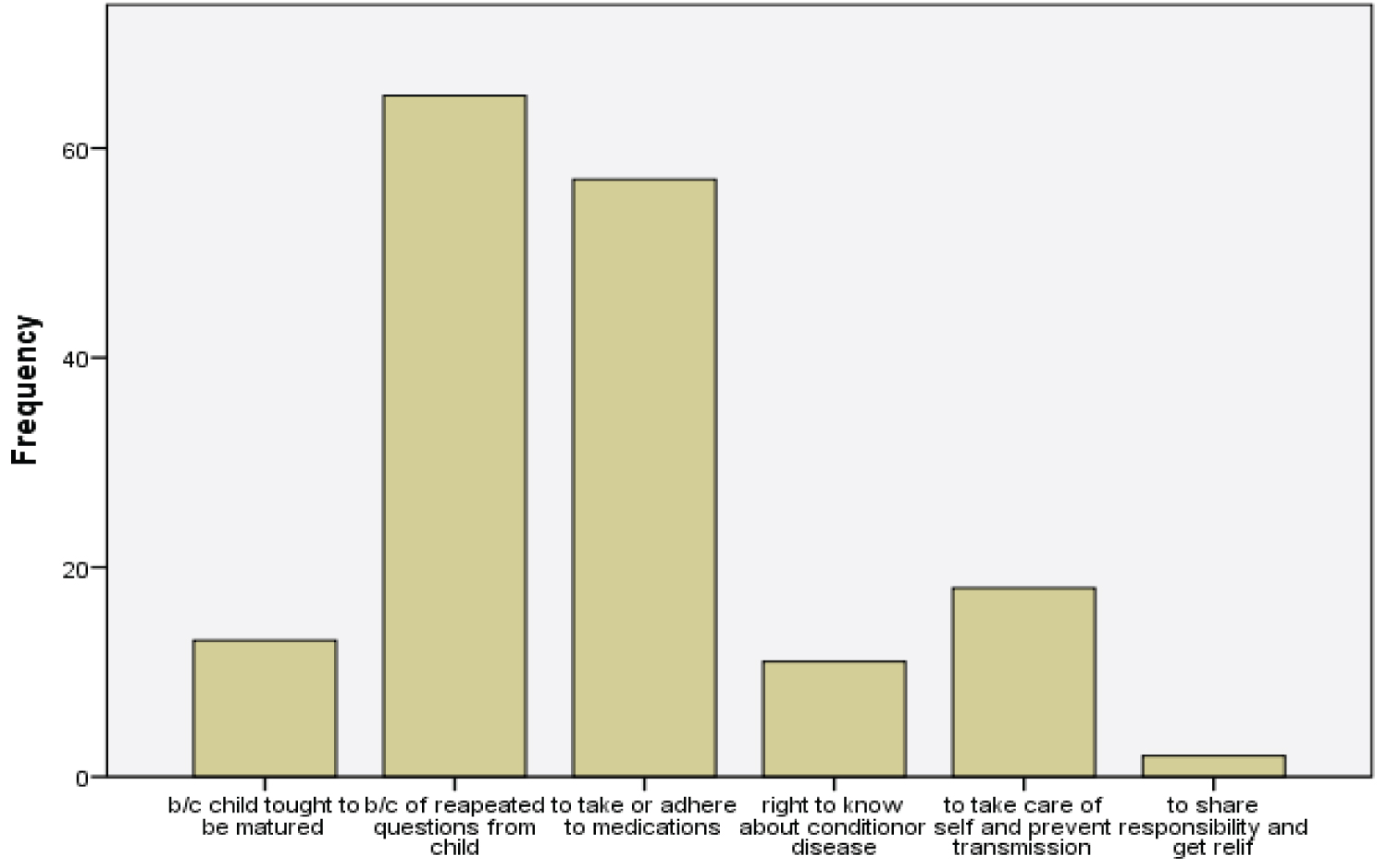 Figure 2: Reason for disclosure of HIV status to the child, Addis Ababa, Ethiopia, 2021.
View Figure 2
Figure 2: Reason for disclosure of HIV status to the child, Addis Ababa, Ethiopia, 2021.
View Figure 2
Out of the total study participants, one hundred forty-three of the caregivers did not disclose the diagnosis of HIV infection to their children. 35 percent of these participants delayed disclosure because they believed the child was too young to understand the diagnosis, and 21.7 percent feared social rejection (fear of stigma and discrimination).
From the participants 53.9% disclosed their HIV status to their children. The initial reaction was acceptance for twenty one percent one hundred fourteen of them had good adherence and sixty-six participants had a no change of CD4 count after disclosure ten precent says their child interaction felt that disclosure was important on and 17.4% had a relieved Feeling after disclosure see details in Table 5.
Table 5: Outcome of HIV positive status disclosure on HIV positive children, Addis Ababa, Ethiopia, 2021. View Table 5
Factors associated with disclosure of HIV-positive status to infected children were assessed by binary logistic regression. In univariate analysis, the age of the child and the caregivers with whom the children were living, the WHO clinical stage of the child, the age of the child at diagnosis, the duration of ART, the treatment adherence of the child, the disclosure issue with the health care provider, the health care provider adequately covering the disclosure issue, and support from other organizations had p-values less than 0.25, and the variables were selected for multivariable analysis. In multivariable analysis, age of children (AOR) [1.5 (3.071-5.256), duration of ART (AOR) [3.093-1.501], good treatment adherence (AOR) [1.241-3.487], and adequate advice from a health care provider (AOR) [2.1 (5.728-6.527)] were independently associated with disclosure of HIV-positive status to infected children; see details in Table 6.
Table 6: Factors associated with disclosure of HIV-positive status among care givers to children on highly active anti-retroviral therapy, Addis Ababa, Ethiopia, 2021. View Table 6
Disclosure has become an essential part of the care for HIV-infected children in antiretroviral therapy clinics. Disseminating HIV positive status to infected children is one of the most difficult psychosocial challenges that parents and caregivers face. The main reason for disclosure was the child's repeated questions, while the rest disclosed it because the child was thought to be mature enough to: take or adhere to medications; have the right to know about his or her disease condition; take care of him or herself and prevent disease transmission; share responsibility; and get relief. Several studies have shown the importance of disclosing the HIV positive status to children infected with HIV for psychological benefits (facilitating children's adjustment) and positive effects on the clinical course of the disease (increasing adherence to medications, treatment regimens, doctor visits, and hospitalizations) [21]. Despite concerns about the psychological and social consequences of HIV disclosure to children, some studies in developed countries show that HIV-infected children adopt and live well after disclosure, even better than children who are unaware of their HIV status.
The disclosure rate in this study was 53.9 percent. As previously stated, disclosing HIV status to children has several advantages for them. However, due to different factors, caregivers refrain from revealing their status. This study’s finding is higher compared with studies done in 2013 and 2014 in northern Ethiopia, which showed a prevalence of 31.5 and 33.3%, respectively [15,18]. In contrast to our findings, low disclosure rates were reported in Kenya (29) and Addis Abeba (17%) in 2012 [18]. The probable reason for the better prevalence of disclosure in this study could be due to the higher number of older primary school-aged children in the study. An increase in awareness might have been created over time as different stakeholders worked on areas to improve the disclosure status. But still, the disclosure in the study area can be greatly improved.
The age of the child was found to be one of the factors independently associated with HIV-positive status disclosure to infected children. Children aged 10-15 years were approximately one and a half times more likely to be informed of their HIV-positive status than those aged 6 to 9 years. This could be due to the older children repeatedly asking the reason why they were taking medication, or it might be the belief of the caregivers that the older they get, the more mature they will become, leading to better self-care and compliance with the medications given. This finding agreed with studies conducted in central and northwest Ethiopia, where children of the same age were more likely to be disclosed than their counterparts not in school [14,19]. Children in other African countries were more likely to know their HIV diagnosis result as they aged, according to similar findings [23,24].
Another factor associated with HIV status disclosure to children was the length of time on ART. Those children who were on ART from 6 to 13-years-old were about three times more likely to disclose their HIV status than their counterparts. This finding agreed with studies done in developing countries, including Ethiopia [18,19]. The study in Bahir Dar reported that children who had taken ART for more than five years were five times more likely to have their status disclosed [14]. This might be due to the fact that when the children stay on ART for a long period of time, their curiosity about why they are taking the medications will increase, and they will start to ask questions about their HIV medications more and more as time goes by. Another factor associated with the disclosure of HIV status to children was good adherence to treatment. Good adherence not only helps disclosure but also facilitates a good outcome after disclosure. Several studies have shown that disclosing HIV positive status to HIV-infected children has benefits. For instance, a study conducted in Brazil showed positive effects on the clinical course of the disease (increased adherence to medications, treatment regimens, doctor visits, and hospitalizations) [21]. Similar results were also shown in other studies conducted in Ghana and Ethiopia, which showed that the reason caregivers disclose an HIV diagnosis to children, is that HIV serostatus disclosure positively influences adherence to ART for some HIV-positive children. It also enables children to understand HIV infection and to make sense of disease-related experiences and the importance of adherence [25,26]. A good health care provider who provides adequate care was also found to have a positive association with disclosure. HCW play an important role in childcare and in providing psychological support to both the child and the caregiver. So, the more the caregiver and child get adequate care and information from the HCW, the more confidence and reassurance they get to disclose their status to the child. This study had limitations due to clinical characteristics not assessed, social desirability bias, and cross-sectional nature.
The prevalence of HIV-positive status disclosure to infected children in Addis Ababa is a little more than half (53.9%) and has shown an improvement compared to previous findings. Factors such as the age of the child, the duration of ART, good treatment adherence, and adequate advice from a health care provider were all increase the likelihood of disclosure. The main reasons for disclosure were repeated questions from the child, and the main reasons for non-disclosure were caregivers' thoughts that the child couldn't keep a secret, fear of self-discrimination, and the child being too young to handle the information. There is still room for improvement, and health care workers should give age-appropriate counselling and support and work together with caregivers in the process of disclosing their diagnostic results. The prevalence of the disclosure status is a little more than half, and further efforts should be made to increase it.
To do this, caregivers should be informed of their HIV status gradually, health care workers should have training guidelines for disclosing to children, and the Ministry of Health, stakeholders (NGOs), and Administration city health planners and policy makers should give special emphasis to health care institutions.
Additionally, research should be conducted to assess caregiver attitudes and associated factors regarding HIV status disclosure to an HIV-positive child, and additional studies should be done to assess ART service- and program-related factors.
Ethical clearance was obtained from Santé Medical College department of public health, Research ethics Committee. Following approval, an official letter of support was given to the city Administration Health Bureaus, and hospitals. Permission was obtained from each hospital management body. Participants were informed that participation was voluntary and that they could withdraw at any time if they were not comfortable about the questionnaire. Informed consent was obtained from all caregivers and assent was obtained from the age 13-15. Then, the interview was carried out privately in the private room. Names or personal identifiers were included in the questionnaires to ensure anonymity. Furthermore, all the basic principles of human research ethics (respect for persons, beneficence, voluntary participation, confidentiality, and justice) were respected. The respondents also had the right to refuse or terminate at any point in time. The information provided by each respondent was kept confidential. Confidentiality and privacy were ensured at all levels throughout the study by keeping the data and records in safe place.
Finally informed consent was obtained from all subjects and/or their legal guardian(s). The participants were assured that the information given was used only for the study and that confidentiality was to be kept. Authors had confirmed that all methods were carried out in accordance with relevant guidelines and regulations and confirmed that informed consent was obtained from all subjects and/or their legal guardian(s). Authors had confirmed that all experimental protocols were approved by a named institutional and/or licensing committee.
Not applicable.
Datasets used in the current study are available from the corresponding author upon reasonable request.
Authors declared that they have no competing interest.
Funding for this study was obtained from Santé Medical Colleges. The college had no role in the design of the study and collection, analysis, and interpretation of data.
YW& DBD, contributed to the conception, design, and conduct of the study, analyzed and interpreted the data, and prepared the manuscript contributed to the conception, design, and conduct of the study, analyzed and interpreted the data, and prepared the manuscript; DBD &YW contributed to the design and conduct of the study, analyzed and interpreted the data, and prepared the manuscript. All authors read and approved the final manuscript.
We would like to say thanks to Santé medical college of health science department of Reproductive health for giving me this chance to prepare this thesis and supports it rendered me in accomplishing this thesis. We want to thank my data collector, participant and beloved family, for their support during the whole process of this research. Our heartfelt thanks also go to all Addis Ababa University and their staffs for their cooperation and permission to conduct this study. Moreover, we want to thank all the study participants and the Data collectors for their cooperation and willingness to participate in this study.