The connection between sleep disorders and chronic musculoskeletal pain is bidirectional, as inadequate sleep can amplify muscle tension, whereas chronic pain can reduce sleep quality. Both disorders are highly prevalent in nurses. This article aims to evaluate the correlation between sleep quality and musculoskeletal symptoms in the nursing team of a university hospital. We designed a cross-sectional study that included 40 nursing practitioners who work exclusively in the emergency department. The Nordic Musculoskeletal Questionnaire was used to verify the prevalence of musculoskeletal symptoms and the sleep quality was assessed by the Pittsburgh Sleep Quality Index. Most of the professionals were overweight and had at least one chronic comorbidity. The highest prevalence of symptoms was at the lower back. There is a nine fold increased risk of presenting musculoskeletal symptoms for professionals with poor sleep quality (OR = 9.0 [95% CI, 1.5-53.9]) (Graphical Abstract).
 Graphical Abstract.
View Graphical Abstract
Graphical Abstract.
View Graphical Abstract
Sleep disorder, Musculoskeletal pain, Nurses practitioners
MSDs: Musculoskeletal Disorders; NMQ: Musculoskeletal Questionnaire; DLAs: Daily Life Activities; PSQI: Pittsburgh Sleep Quality Index; AIC: Akaike Information Criterion; BMI: Body Mass Index; ICU: Intensive Care Unit; OR: Odds Ratio; CI: Confidence Interval
Emergency departments are challenging workplaces owing to their high demand, inadequate infrastructure, and complex patients [1]. Nurses are an essential part of the workforce in these places and must deal daily with irregular shifts and overloaded work routines, which are characterized by complex, time-consuming, and stressful activities [2].
Nurses often suffer from musculoskeletal disorders due to unfavorable working conditions, which can greatly affect their quality of life and lead to absenteeism [2,3]. These disorders most commonly affect the lumbar, shoulder, and neck regions, with a prevalence of > 40% among healthcare professionals [4]. In addition, nurses often struggle with sleep disorders, particularly those working night shifts. These professionals experience low sleep quality and increased daytime sleepiness due to disruptions in their circadian cycles [5].
Studies have shown a significant correlation between sleep disorders and chronic musculoskeletal pain [6,7]. The connection between the two can be bidirectional, as inadequate sleep can amplify discomfort and muscle tension, whereas chronic pain can reduce sleep quality [8,9]. Emergency nursing practitioners are particularly vulnerable to both conditions, which can adversely affect their work and personal lives. Therefore, it is imperative to expand our scientific knowledge on this matter, considering the critical responsibilities of these professionals.
This study examined the relationship between sleep quality and musculoskeletal symptoms in a nursing team working in the emergency department of a university hospital. This study aimed to achieve three specific objectives: (1) Determine the prevalence and degree of musculoskeletal symptoms; (2) Evaluate the quality of sleep among these professionals; and (3) Investigate the link between symptom severities and sleep quality.
This observational study was conducted at Ribeirão Preto Medical School Hospital in Brazil between January and March 2022. To collect data, in-person interviews were conducted during intraday breaks. The study focused solely on nurses and nursing technicians working in the emergency department, excluding retired professionals, undergraduate students, and volunteer workers.
The study was conducted in accordance with the Declaration of Helsinki and the Brazilian National Health Council. The study protocol was approved by the Institutional Research Ethics Committee (CAAE: 3928.6220.9.0000.5440). All the participants who fulfilled the eligibility criteria and agreed to participate in the study provided written informed consent.
To maintain the quality of the data collection process, we implemented a standardized protocol. We gathered pertinent information regarding personal, occupational, and health characteristics, such as sex (male/female), age, body mass index (BMI), work shift (day/night), job position (nurse/nursing technician), duration of employment in the current position, and presence of any comorbidities (yes/no).
The Brazilian version of the Nordic Musculoskeletal Questionnaire was used to explore the occurrence of symptoms in various body regions, their impact on daily life activities, and whether medical attention was necessary [10]. The participants were requested to pinpoint the affected regions on a human body diagram. The questionnaire documented the symptoms encountered over the past 7 days and 12 months.
To evaluate sleep quality, we used the Pittsburgh Sleep Quality Index (PSQI), a comprehensive questionnaire comprising of seven components. These components were designed to assess subjective sleep quality, latency, duration, changes, habitual sleep efficiency, use of sleep medications, and daytime sleep dysfunction. The sum of the values assigned to each component ranged from zero to 20, with higher scores indicating poorer sleep. The creators of this tool indicate a score of five as the threshold between good and poor sleep quality [11,12].
Continuous data were presented as the mean ± standard deviation, or median [first, third quartile]. Categorical variables were presented as counts (percentages). To compare continuous variables, we employed either the Student’s t-test or the Wilcoxon-Mann-Whitney U test, while for categorical variables, Fisher’s exact test or Pearson’s chi-square test was used to compare the groups.
Logistic regression models examined the relationship between musculoskeletal symptoms and sleep quality. To ensure accuracy, ineffective or low-impact factors were eliminated using stepwise forward and backward regression methods, and the Akaike Information Criterion (AIC) was used to estimate the prediction error. In addition, we investigated how the same independent variables were associated with the number of affected areas. Negative binomial regression was used to model the data, given the counting nature of the dependent variable and its over-dispersed values. The same stepwise approach based on the AIC values was used to determine the most optimal model.
Statistical significance was assessed using a two-sided p-value of < 0.05. Analyses were conducted using the R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
The study participants were 16 nurses and 24 nursing technicians, all of whom worked exclusively in the emergency department. There were 40 participants, 34 of whom were women. Their ages ranged from 24 to 66 years, with a mean BMI of 25.7 ± 4.0 kg/m 2 . In addition, 23 participants reported at least one chronic morbidity. On average, the participants worked 36 h per week (ranging from 12 to 48 h); primarily in daily shifts (65%). The median length of employment in this position was 5.5 years (range, 0.4-33 years).
The lumbar region had the highest number of reported complaints, with 55% of individuals experiencing symptoms within the previous 12 months. The shoulders and neck were closely monitored, with both regions reporting a 47.5% incidence of symptoms. When seeking medical assistance, the lumbar region was the most common area of concern (17.5%), followed by the upper back region (15.0%). These symptoms in the lower back were severe enough to limit the ability to perform daily activities, including work, leisure, and domestic care, in 30% of those surveyed. Additionally, 12.5% of the participants reported similar limitations due to upper-back symptoms. In terms of recent complaints within the last 7 days, the lumbar region remained the most affected (50%), followed by the upper back, neck, and shoulders (40%). Table 1 provides further details on the prevalence of musculoskeletal symptoms.
Table 1: Nordic questionnaire results in emergency department nurse staff (n = 40). View Table 1
According to the PSQI, the median score was seven, ranging from one to 15. The majority (65%, 26 individuals) scored > 5, indicating poor sleep quality. Group five, the sleep disturbance group, had the lowest scores of the seven evaluated sleep components. 26 respondents reported taking > 30 min to fall asleep, while 33 were unintentionally awake. Furthermore, nine professionals reported regularly using hypnotic drugs to aid sleep.
Association between sleep quality and musculoskeletal symptoms: The data presented in Figure 1 show that individuals with PSQI scores > 5 had a higher prevalence of musculoskeletal symptoms across all sites in the last 12 months (p = 0.014). In addition, there were greater odds of experiencing musculoskeletal complaints among professionals with poor sleep quality (OR = 9.0 [95% CI, 1.5-53.9]).
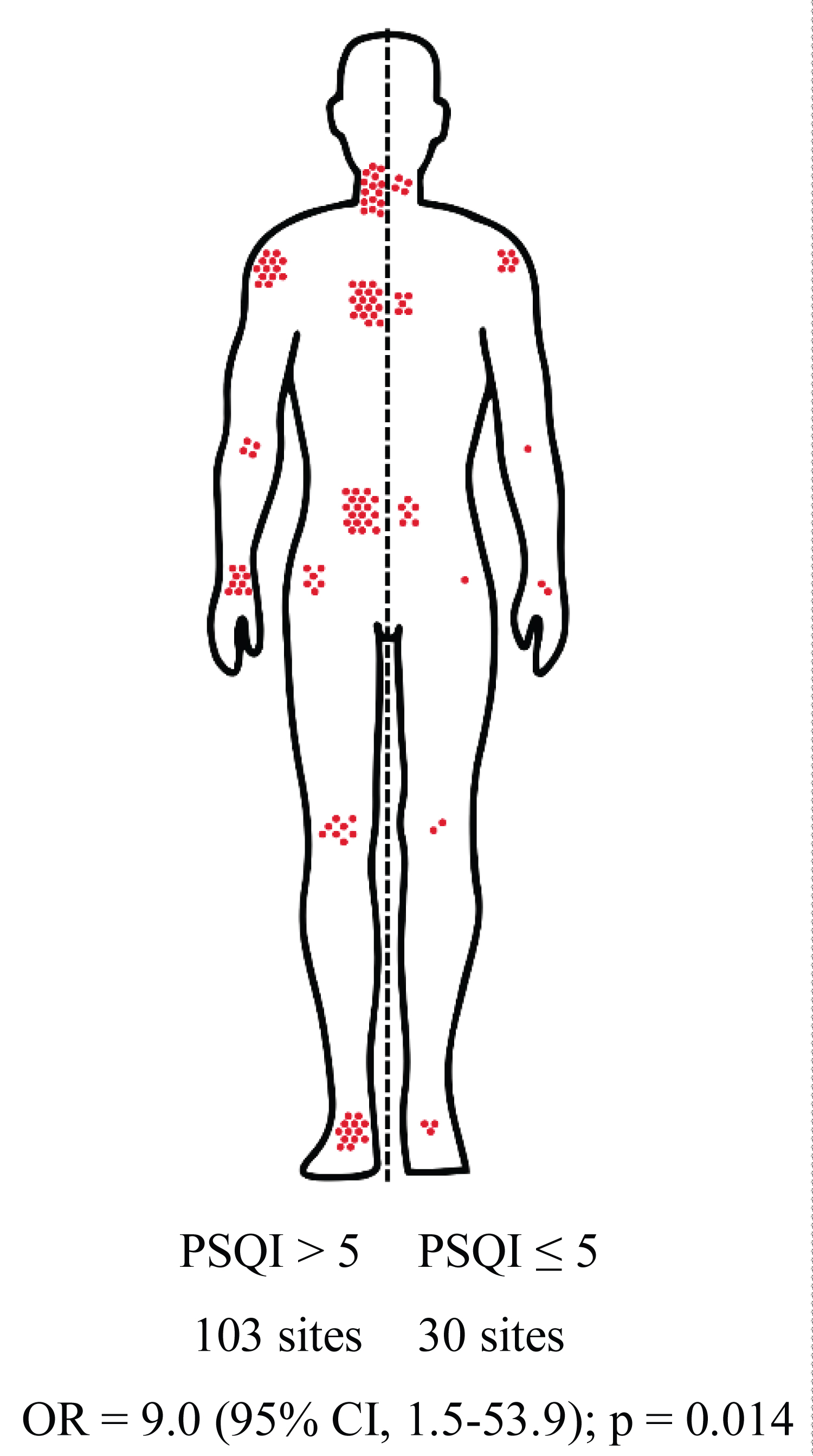 Figure 1: Prevalence of musculoskeletal symptoms according to sleep quality assessed by PSQI.
View Figure 1
Figure 1: Prevalence of musculoskeletal symptoms according to sleep quality assessed by PSQI.
View Figure 1
A logistic regression model was used to identify variables associated with musculoskeletal symptoms. A stepwise approach was applied, and only two variables, comorbidities, and the PSQI were retained in the final model. An interaction analysis conducted between the two variables revealed that comorbidities did not moderate the PSQI scores. Therefore, only PSQI was used as an independent variable in the final model.
Another regression model was used to identify the optimal combination of variables associated with the number of affected sites. Negative binomial regression analysis revealed that the BMI and PSQI scores were the only significant variables. An interaction analysis was subsequently conducted between these two variables, ultimately revealing that BMI did not moderate PSQI scores. Consequently, only the independent variable, PSQI, was included in the final model. Figure 2 displays the number of symptomatic body regions as a function of the PSQI. The graph compares the actual values with those predicted using the Full, Stepwise, and Final models.
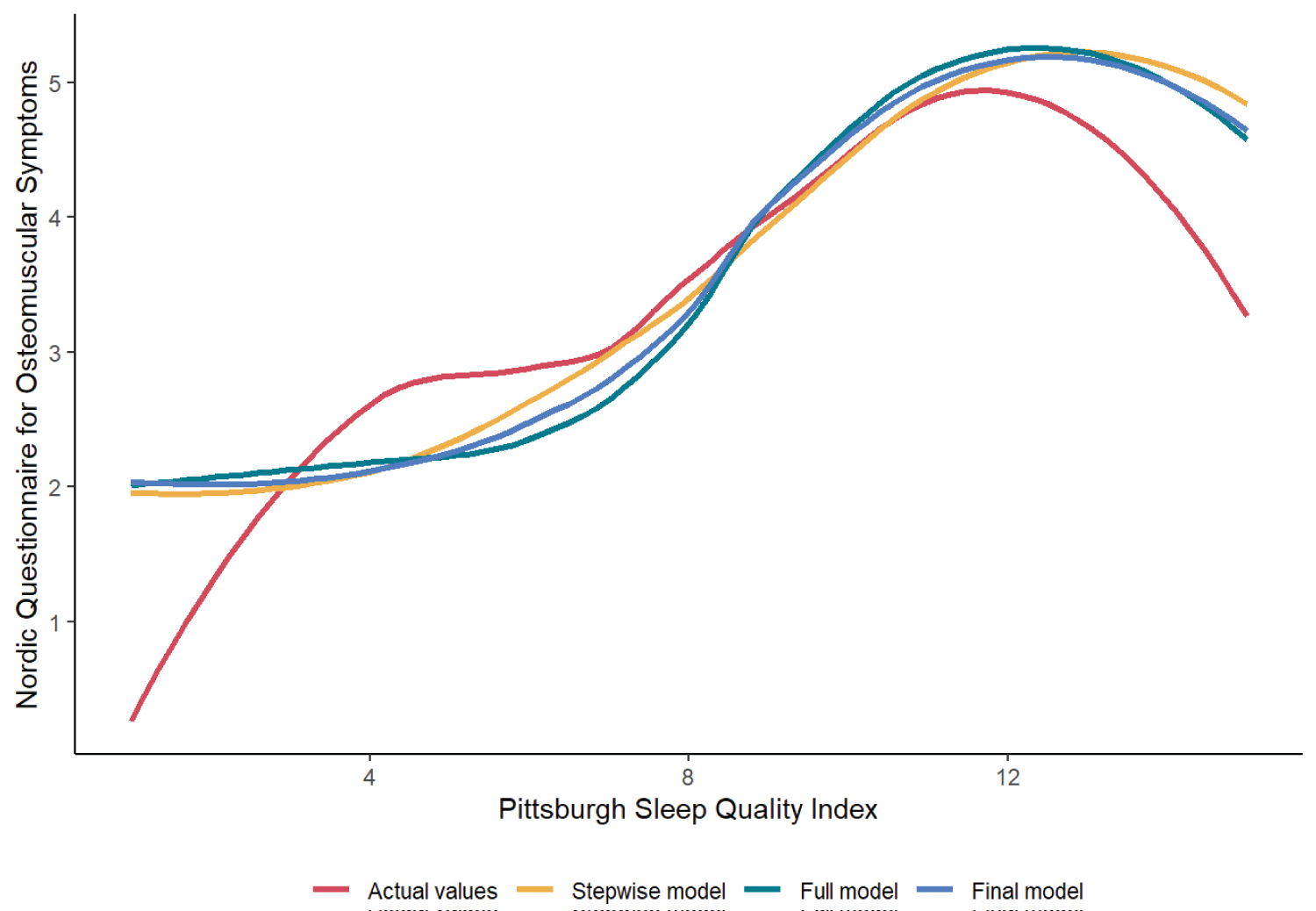 Figure 2: Number of symptomatic body regions as a function of the PSQI.
View Figure 2
Figure 2: Number of symptomatic body regions as a function of the PSQI.
View Figure 2
According to the study, emergency department nurses were more likely to be overweight and have at least one ongoing medical condition. They often experience discomfort in their lower back, shoulders, and neck. This study also found a significant correlation between factors, such as BMI, comorbidities, poor sleep quality, and musculoskeletal symptoms. Additionally, a large percentage of participants reported poor sleep quality, and those with poor sleep quality were nine times more likely to report symptoms than those with good sleep quality.
Musculoskeletal disorders can cause substantial financial setbacks [3]. Nursing professionals may experience job dissatisfaction due to these maladies [13,14], leading to absenteeism, early retirement, and a decline in customer relationships [14].
According to our results, the lumbar spine, shoulders, and neck were the most frequently affected regions. These findings are consistent with those of a similar study conducted in Brazil, which revealed that hospital nurses experienced a symptom prevalence of 57, 52, and 48% in the lumbar, shoulder, and neck regions, respectively [15]. However, international studies have reported different outcomes, with lower back pain being the most common cause of discomfort. For example, a study in Iran found that hospital nurses experienced an 88.4% prevalence rate of lower back pain, 88.4% of knee pain, and 71% of hip/thigh pain [14]. Similarly, a Malaysian study found that hospital nurses experienced an 86.7% prevalence rate of lumbar pain, 86.7% of ankle pain, and 86% of neck pain [16]. Chiou, et al. [17] reported a 68.3% prevalence rate of lumbar pain among hospital nurses in Taiwan, and Rypicz, et al. [18] reported a 66.9% prevalence rate of lumbar pain among hospital nurses in Poland. These findings underscore the need for targeted interventions to address this issue and prioritize the well-being of this population of healthcare workers.
Nursing professionals working in hospitals face various risks that can result in musculoskeletal symptoms. According to a study conducted by Chiou, et al. [17], nurses working in surgery centers, delivery rooms, emergency departments, and intensive care units (ICUs) have a high prevalence of lower back pain. Another study by Ou, et al. [19] indicated that emergency department nurses were more prone to experiencing shoulder, lower back, and knee symptoms than ICU or ward workers. This study also revealed that emergency department workers were at a higher risk of developing musculoskeletal disorders than their counterparts in other departments.
Studies show that musculoskeletal disorders have a complex and multifaceted origin [20]. Hospital nurses are particularly vulnerable to these disorders due to a variety of contributing factors, including age [16,21-23], shifts that exceed 7h [24], biomechanical and ergonomic stressors at work (such as awkward postures and manual patient handling) [23,24], and psychosocial factors (such as high work demands with low control, effort-reward imbalances, and low social support) [23,25]. Additionally, being female [21,23] has been identified as a risk factor for these disorders. In our study, we identified three key factors contributing to musculoskeletal symptoms among healthcare workers. These factors included BMI, presence of comorbidities, and sleep quality.
Our findings align with those of previous studies conducted by Krishnan, et al. [16], who noted a higher frequency of symptoms among Malaysian nurses with elevated BMI. Similarly, Lin, et al. [20] found a correlation between BMI and symptoms in various body parts in hospital nurses in China. Furthermore, both Azizpour, et al. [21] and Rezaei, et al. [26] discovered that healthcare professionals with a higher BMI had a greater likelihood of experiencing lower back pain than their eutrophic colleagues. An individual’s BMI can significantly impact on joint health, potentially leading to the development of conditions such as osteoarthritis [27]. Obesity can also create additional strain on the abdominal region, which may increase the likelihood of muscle spasms in the lumbar area [26]. Additionally, a sedentary lifestyle is often associated with higher BMI and may contribute to musculoskeletal discomfort [28]. Encouraging healthy eating habits and physical activity can help reduce BMI and alleviate musculoskeletal symptoms among hospital nurses.
The presence of comorbidities is associated with a higher incidence of musculoskeletal symptoms. In a study by Alexopoulos, et al. [29] on nurses in Greece, a poorer overall health status (encompassing comorbidities) was associated with a greater prevalence of lower back, neck, and shoulder pain. Nursing professionals face various occupational hazards, such as biological, chemical, ergonomic, and psychosocial risks [30], which increase their susceptibility to morbidity from different health issues, as outlined in a systematic review by Fronteira, et al. [30].
With regard to sleep quality, this study showed that the sample of hospital nurses had poor overall sleep quality, a finding consistent with other studies conducted both internationally and in Brazil [31-34]. Specifically, among nurses working in the emergency department, one study found a 66% prevalence of poor sleeps quality [33], while another found a prevalence of 52.8% [34]. Factors that have been linked to poor sleep quality in the nursing population include greater fatigue [31], poor mental health [32,33], being female [33,34], having a higher weekly workload [32], having more years of service or being in the institution [33,34], working night shifts [32-34], working in the emergency department, ICU, or department of gynecology and obstetrics [33,34] having poor perception of general health [33], experiencing high occupational stress [33,34], and having low physical activity outside of work [34].
In this study, participants with poor sleep quality had a nine-fold increased risk of developing musculoskeletal symptoms. Another study conducted in Sweden in the general population also found an increased risk of lower back pain in subjects with sleep disorders [35]. Similarly, a study conducted in Finland in the general population found a significant correlation between poor sleeps quality and shoulder impingement syndrome [36]. Among hospital nurses, certain characteristics of poor sleep quality, such as prolonged sleep onset latency and the use of sleep-promoting substances were associated with a higher risk of musculoskeletal symptoms [37]. However, no studies have investigated the relationship between sleep quality and musculoskeletal symptoms among nurses working in the emergency department.
Insomnia independently affects the development and prognosis of chronic pain [38-40]. Pain can be both, a cause and a consequence of sleep deficiency [9]. This bidirectional relationship between sleep and pain has important implications for patient care, the prevention of chronic pain, and public health [9]. Sleep deficiency affects several systems that influence nociceptive processing. Specifically, sleep disturbances seem to have an inhibitory effect on mediators with analgesic properties (opioid, orexinergic, melatonin, and dopamine signaling systems) while activating systems with hyperalgesic properties (nitric oxide signaling, adenosine, and inflammatory mediators of the immune system) [9,38]. Finally, it is worth noting that sleep disorders can significantly impact work performance among nursing professionals. Specifically, they can decrease efficiency and productivity, increase the likelihood of errors compromising patient safety, increase job dissatisfaction, and influence the decision to leave their jobs [41].
Our study had a few limitations. First, its cross-sectional design restricted the ability to make temporal comparisons. Additionally, our data were obtained from a single center using convenience sampling. This approach may have introduced bias, as those affected by musculoskeletal symptoms may have considered the research more relevant, whereas those without symptoms may have chosen not to participate. Moreover, the interview process was subjective and reliant on volunteer collaboration, which may be affected by mood, physical or mental exhaustion on the day of completion. Such factors can influence the responses, making them unreliable. Despite these limitations, our study offers valuable insights into the health statuses of nursing agents working in emergency units. We advanced the current understanding of this topic by demonstrating the importance of sleep quality in these subjects.
Nursing agents working in emergency units exhibit poor health status, as evidenced by frequent complaints of musculoskeletal symptoms and poor sleep quality. These symptoms are particularly associated with BMI, comorbidities, and sleep quality, highlighting the need for improved lifestyle habits, healthcare, and work routines to enable these professionals to achieve better rest.
1. Musculoskeletal and sleep disorders are prevalent in emergency nursing professionals.
2. The highest prevalence of musculoskeletal symptoms was at the lower back, followed by shoulders, and neck.
3. Professionals with poor sleep quality have a 9-fold increased risk of presenting symptoms.
We are indebted to the staff at the Emergency Department of the Ribeirão Preto Medical School Hospital.
There is no funding source.
☒ The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
☐ The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: