Worldwide burden of ID estimated to be 43% globally in 2011 and about 70% in Central and West Africa and 7-9% of USA children ages 1-3 years have iron deficiency (ID). Countries in high caloric nutrition switch have a high prevalence of overweight and obesity, a moderate prevalence of undernutrition and micronutrient deficiencies. Infants and children must obtain 30% of their daily iron from their diet to provide the necessary iron for new muscle cells and RBCs.
259 infants visited child health family medicine clinic Hatta Hospital, UAE for 12 months assessment and vaccination from April 2014 to January 2015. Anemia was defined as per World health organization (hemoglobin ≤ 11 gm/dl).
Anemia was found in 99 infants (38.2%), Iron deficiency anemia in 60 (23.2%), thalassemia trait in 12 (4.6%), normocytic anemia in 27 (10.4%) and iron deficiency in 57 (22%). Mild anemia was found 41 infants (61.3%, p value 0.000) in iron deficiency anemia.
Serum iron 49 infants (81.7%, p value 0.000), high RDW 52 (86.7%, p value 0.000), Mentzer index 54 (90%, p value 0.000) and Srivastav index (50%, p value 0.000) significantly detect iron deficiency anemia.
Iron deficiency anemia (23%) in this population are consistent with other reports from region but higher than developed countries. Serum iron, high RDW, Mentzer and Srivastav index were significant in detecting iron deficiency anemia in this study. Microcytosis in the study population apart from iron deficiency anemia could be attributed to alpha thalassemia trait in this population.
Iron deficiency, Anemia, Infants
Iron deficiency (ID) is the most common micronutrient deficiency in children [1]. Worldwide burden of ID estimated to be 43% globally in 2011 and about 70% in Central and West Africa and 7-9% of USA children ages 1-3 years have ID [2]. ID during fetal development and the first 2 years of life is associated with poor growth and decreases in cognitive, motor, and social emotional development [3,4].
Countries in advanced nutrition switch have a high prevalence of overweight and obesity, a moderate prevalence of undernutrition and micronutrient deficiencies [5]. World Health Organization (WHO) detects deficient and inadequate intakes or status of calcium, iodine, iron, and zinc as well as vitamin A, vitamin D, and folate as commonly reported by many countries in the Middle East region, mostly in children and childbearing age women [6].
A study done by Hopkin, et al., showed the prevalence of anemia was 23% at 8 months of age, and 18% at 12 months of age [7]. The prevalence of non-anemic iron deficiency may be as high as 30% in toddlers from developed countries [8-10].
According to WHO prevalence of anemia severity describes as mild problem 5%-19.9%, moderate problem 20%-39.9%, and severe problem ≥ 40%; most Arab Middle East countries fall within the category of moderate to severe deficiency [11,12].
IDA was predominant in boys and peak IDA incidence was noted among infants aged 9-12 months. Only 7% patients exhibited symptoms of IDA, while 23.6% patients with severe IDA demonstrated classic symptoms/signs of IDA [13].
Anemia is the most prevalent nutritional disorder among children in the Middle East and North Africa region. The prevalence of anemia in children and adolescents ranges from 11.6% in Saudi school-aged children to 37%-52% among Egyptian children aged 12-36 months [14-17].
This rise in the prevalence of anemia is attribute to shifting of food consumption patterns and increases in childhood diarrhea [18].
The purpose of this study was to determine the hematological profile, the frequency and severity of iron deficiency anemia (IDA) in one-year old Emeriti infants of Hatta suburb, UAE.
All infants attended child health family clinic Hatta Hospital-UAE, for one-year assessment and vaccination from April 2014 to January 2015 were included in the study and infants who were not underwent laboratory test were excluded. After history, physical examination conducted by family physician, laboratory test such as complete blood count (CBC), serum ferritin (Fe), serum Iron were advised and follow up appointment given after 4 weeks to review lab test.
Anemia was defined as: Hemoglobin ≤ 11 gm/dl [19].
Anemia severity classified according to WHO guideline as:
1. Mild anemia: Hemoglobin 10-11 gm/dl
2. Moderate anemia: Hemoglobin 7-9.9 gm/dl
3. Severe anemia: hemoglobin < 7 gm/dl
Iron deficiency anemia defined as; low hemoglobin (≤ 11 gm/dl), low MCV (≤ 70 fl) with low serum ferritin (as per laboratory reference, some cases mentioned 4.01 and in other 61) or serum iron (< 43), high red cell distribution width (RDW) ≥ 15%.
Thalassemia trait defined as low hemoglobin (≤ 11 gm/dl), low MCV (≤ 70 fl) with normal serum ferritin or serum iron, high RBC mass, low RDW < 15%.
Iron deficiency was defined as normal hemoglobin with low serum ferritin or serum iron level.
Three index were used to differentiate Iron Deficiency Anemia with thalassemia trait.
| Formula | IDA | Thalassemia Trait | |
| Mentzer index | MCV/RBC | > 13 | < 13 |
| RDWI | MCV × RDW/RBC | > 220 | < 220 |
| Srivastava index | MCH/RBC | > 3.8 | < 3.8 |
All data entered into SPSS software version 24. Mean and Standard Deviation was taken for variables such as Hemoglobin, MCV, RBC mass, MCH, RDW, Serum iron, Serum ferritin and frequency of variables such as anemia, anemia severity, anemia types, Microcytosis, Serum iron, serum ferritin, RDW, RBC mass, Mentzer index, RDWI index, Srivastava index.
Chi-square test was used to differentiate quantitative variables (anemia severity, RBC mass, RDW, Mentzer index, RDWI index, Srivastava index) in Iron deficiency anemia and thalassemia trait. P value of < 0.05 considered as significant. Prior approval taken from ERC committee and department head of facility.
Total 320 infants attended child health family clinic Hatta Hospital-UAE, for one-year assessment and vaccination from April 2014 to January 2015, out of these 259 did laboratory test. Mean and Standard Deviation of variables (Hemoglobin, MCV, RBC mass, MCH, RDW, Serum iron, Serum ferritin) were calculated as shown in Table 1.
Table 1: Mean and standard deviation data. View Table 1
Anemia was found in 99 infants (38.2%), Iron deficiency anemia in 60 (23.2%), Thalassemia trait in 12 (4.6%) and normocytic anemia in 27 (10.4%). Iron deficiency was found in 57 infants (22%). Details of frequency of quantitative variables (anemia, anemia severity, anemia types, Microcytosis, Serum iron, serum ferritin, RDW, RBC mass, Mentzer index, RDWI index, Srivastava index) are shown in Table 2. Details of frequency of anemia variables shown in Table 3 and type of anemia shown in Figure 1.
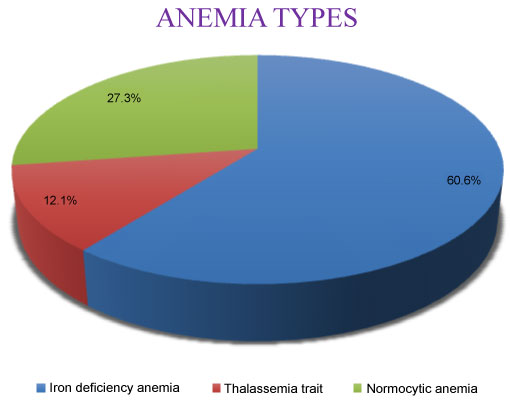 Figure 1: Anemia types. View Figure 1
Figure 1: Anemia types. View Figure 1
Table 2: Frequency of variables (Total 259). View Table 2
Table 3: Frequency of variables in anemia. View Table 3
Among iron deficiency anemia most infants had mild anemia 41 (61.3%, p value 0.000). Serum iron was significantly low in iron deficiency anemia 49 infants (81.7%, p value 0.000) as compare to serum ferritin 33 (55%, p value 0.025). RDW was significantly high in 52 (86.7%, p value 0.000). Among indexes, Mentzer and Srivastav index were significant in detecting iron deficiency anemia 54 (90%, p value 0.000) and 30 infants (50%, p value 0.000) respectively, while RDWI index 22 infants (36.7%, p value 0.183) as shown in Table 4.
Table 4: Frequency of variables in iron deficiency anemia. View Table 4
Srivastav index significantly detect thalassemia trait 30 (50%, p value 0.000) while Mentzer index and RDWI index were not significant in our study. Details of variables among thalassemia trait shown in Table 5.
Table 5: Frequency of variables in thalassemia trait. View Table 5
Infants and children must obtain 30% of their daily iron from their diet to provide the necessary iron for new muscle cells and RBCs. Both the United States Department of Health and Human Services and the World Health Organization (WHO) have set goals to reduce ID and iron deficiency anemia (IDA). The WHO priorities have now been adopted as Priority Nutrition Indicators for the United Nation’s post-2015 Sustainable Development Goals [20-22].
The principal risk factors associated with IDA were age 6-18 months, male sex, higher birth order, consumption of cow’s milk, predominant breastfeeding > 6 months, and/or low iron intake.
Routine screening for ID and IDA between 6-24 months is recommended, especially for children living in areas with a high prevalence of ID. In upper-income countries, a full blood count is obtained, which will give hemoglobin, hematocrit, mean corpuscular volume, and RBC distribution width. In children with IDA, mean corpuscular volume will be decreased and RBC distribution width will most likely be increased. In some settings, ferritin is also measured as part of the screening process. However, ferritin values can be misleading in children living in areas where the infectious disease burden is high because ferritin is also an acute-phase protein.
It is recommended that full-term breastfed infants should start an iron supplement at 4 months (elemental iron 1 mg/kg daily, maximum 15 mg) and the supplement should be continued until the infant is taking sufficient quantities of iron-rich complementary foods [1].
Full-term and preterm babies should be taking complementary foods by 6 months of age. Iron-rich complementary foods include meat (lamb, chicken, beef, and pork), baby cereals (including fortified rice), and some vegetables (green beans, peas, and spinach) [23,24].
• Iron deficiency anemia (23%) in this population are consistent with other reports from region but higher than developed countries.
• The microcytosis in the study population apart from anemia could be attributed to alpha thalassemia trait and a normal variant microcytosis which is highly prevalent in the study population.
• Iron deficiency was found in 22% infants, warrant early interventions to reduce the risk of developing future anemia.
• Need to conduct studies with large sample size, which will help and signify the magnitude of the IDA.