There is emerging evidence that most nursing leadership learning occurs in practice and through social interactions. However, how this social process of learning takes place is not clear and there is limited information about how to support nursing leadership learning as it occurs in clinical settings. The purpose of this study was to increase understanding of the nature of leadership learning in nursing practice. It further aimed to discover the ways in which this type of learning is important to leadership development, and to determine how and why this is the case.
Using a constructivist grounded theory approach, a total of 19 semi-structured interviews with 15 nurse managers were undertaken. Data analysis consisted of coding, constant comparison, memo writing, theoretical sampling and conceptualisation.
It was found that learning occurs by engaging in social interactions, as these interactions are converted into learning events. A four-stage process of learning was identified: Reflecting, discovering, deciding, and choosing. Moving through this process can give rise to changed behaviours and leadership development.
Nurse managers should be supported by providing them with the opportunity to engage in the learning process by providing action learning sets, focusing on reflection.
Nursing leadership, Learning, Social interactions and practice
Nursing leadership development is essential for achieving leadership effectiveness and better organisational performance [1]; improved patient outcomes; [2-5]; increased self-awareness; effective communication including patient-centred communication and interdisciplinary collaboration [6,7]; job satisfaction and workforce retention [8-10]; and improved work environments [11]. Within this broad context the concept of nursing leadership has been put forward as one solution for addressing issues within practice environments [12,13]. Nursing leadership is complex in terms of how it is both learnt and how it is displayed. The increased importance given to nurse leadership learning over the past thirteen years [5,14-18] has led to a plethora of leadership programs for front-line managers. Yet these programs may only be partially successful in achieving their intended learning outcomes such as successfully developing self and others [19,20]. The developers of leadership programs may assume that leadership is context free, ignore the human elements and focus too much on competencies [20,21]. More than four decades ago, Fiedler [22] questioned why most studies are unable to demonstrate the outcomes of leadership development programs. Fiedler [22] questioned the value of the training provided as well as the suitability of leadership theories on which these leadership development programs were based. It appears that to date, this question remains largely unanswered and is further confounded when the practice environment and social learning processes in leadership development initiatives are largely disregarded.
Nursing is a practice based discipline and "revolves around tenets of caring within an overarching altruistic framework" [23]. Conventional wisdom within the nursing profession holds that most learning for nurses occurs through practice. Benner's [24-26] seminal work created an increased understanding of how nursing knowledge is used in practice and highlighted the essential role of experiential learning in professional development [27,28]. Benner's [26] skills acquisition framework was developed on the proposition that nurses develop skills and understanding of patient care along their clinical journey through a sound educational foundation, and more importantly, multiple experiences derived from day-to-day practice.
Therefore, the essential aspects of the nursing role are learned in a healthcare work environment, and nurses' leadership learning may also take place in the work environment. Nursing leadership develops through day-to-day (social) interactions and is a progression of stages through which individuals achieve effective leadership behaviours [29,30]. Indeed, many prominent scholars outside the field of nursing [31-34] have described that leadership development is predominantly a process of learning from social interactions.
Little is known about the process of nursing leadership learning in practice. This may be because the processes involved in the mechanism of learning have not been clearly described. This may be due to the fact that learning that takes place in practice often occurs implicitly [35], and the knowledge generated remains tacit and unacknowledged. Therefore, it is important to explore how nurse managers learn to lead in practice. This will contribute to a greater understanding of the learning processes involved. This study investigated nursing leadership learning from a point of view that sees learning as being a socially situated process and focuses on social interactions and context.
The aim of the study was to increase understanding of the nature of nurse leadership learning in practice. It further aimed to discover the ways in which learning in practice is important to leadership development, and to determine how and why this is the case. A constructivist grounded theory approach [36,37] was used to guide this study.
Ethics approval was obtained from the Tasmanian Health and Medical Human Research Ethics Committee (approval number H0011860).
This study was conducted in two public healthcare organisations in Tasmania, Australia. They included acute, sub-acute and non-acute care settings. The Tasmanian public health and human services sector employs approximately 11,000 people and services a population of approximately 510,000. The study used purposive sampling to recruit 15 nurse managers engaged in the management of a clinical area and who had greater than five years of post-registration experience. Nurse managers were invited to participate by email and four did not respond to the invitation. None of the participants dropped out and both males (n = 4) and females (n = 11) were recruited. The ages of the participants ranged between 30 and 55 years and this is representative of the ages of nurse managers working within the Tasmanian Health Service. The number of participants was not pre-determined and recruitment continued until theoretical sufficiency (data saturation) was established. After fifteen participants were recruited and 19 interviews were analysed theoretical sufficiency was reached.
The interview schedule was based on the research aims and objectives and existing theoretical concepts identified in the literature. Consistent with a constructivist grounded theory approach [36], a few broad, open ended questions were devised to invite detailed discussion of the topic. The semi-structured interviews were conducted by the first author at the participants' place of work. Interview texts provided thick descriptions of the leadership phenomenon under investigation. Interviews varied in length from 35 minutes to 70 minutes and 19 interviews were conducted and analysed. Four participants were interviewed twice to develop a better understanding of some of the emerging concepts and this is a form of theoretical sampling, integral to a grounded theory method. Interviews were audio recorded in a digital format and transcribed verbatim and each interview was analysed before the next interview. Data saturation was reached after 19 interviews, when it was determined that the collection of more data would not provide new theoretical insights and no new codes were produced.
Consistent with a constructivist grounded theory approach, data collection, coding and analysis took place concurrently [37]. Data analysis was performed by using coding, categorisation, conceptual ordering, and theorising. Constant comparison and theoretical sampling were also features [36,37]. The entry of data and coding using computer software QSR Nvivo10 allowed for easy sifting, sorting and discovering of relations between categories [38].
Learning to lead was found to involve social interactions played out in practice. The social interactions differed between individuals and context. None of the participants described the exact same sequence of events, and each social interaction was different in nature, however, a cohesive and shared narrative emerged, which underpinned the study's findings. Nurse managers were found to learn from social interactions by moving through a four-stage learning process (Figure 1):
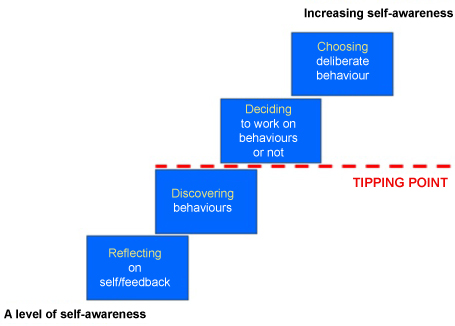 Figure 1: The learning process resulting from the analysis of interviews (N = 19). View Figure 1
Figure 1: The learning process resulting from the analysis of interviews (N = 19). View Figure 1
1) Reflecting: Self-examination, experience and feedback from others;
2) Discovering desirable or undesirable behaviours;
3) Deciding to work on these behaviours or electing not to do so; and
4) Choosing deliberate behaviours.
The learning process starts with one's level of self-awareness and moves towards a position of increased self-awareness. This change is triggered by reflection, self-examination and feedback from others.
Reflection is the first step of the process as reflection on practice events can start the learning process. The participants explained that confrontations with staff prompted reflections. One such interaction involved a nurse being challenged by a staff member in the middle of the corridor. The ensuing discussion was filled with emotion on both sides. The participant in question reflected on the incident and became aware that the situation required attention. The participant realised that it was inappropriate to have the conversation in the corridor and she returned to the person involved explaining that she may not have handled the situation well. Learning for the participant took place through this self-reflection who determined to handle future similar situations differently by saying: "You are feeling very strongly about that. Why don't we pop into the office?"
It was apparent that executing the role of the nurse manager led to social interactions triggering reflection. One participant noted, "Often you are chairing meetings or you are in meetings and you are expected to contribute on behalf of your colleagues or on behalf of the patients, and that takes extraversion". Extraversion in the context of this study means the ability to be an advocate for patients and staff, expressing the needs of these groups. Some participants described themselves as not being outspoken and this was perceived as hindering them in their role as a nurse manager. Participants articulated that they had to abandon their natural inclination of being quiet, as they became aware of not contributing effectively to important conversations. This realisation was predominately reached by comments from colleagues: "Oh, you were quiet in that meeting", or "You did not say much then". These comments acted as a catalyst for participants to reflect and to realise the importance of contributing to discussions, particularly concerning patients and staff. This realisation and awareness can be seen as a discovery, the second phase in the process.
Discovering behaviours is defined as becoming aware of certain (leadership) behaviours. A range of behaviours were depicted in the participants' descriptions and these behaviours were either perceived as desirable or undesirable. Often a focus was placed on the behaviours considered to be a weakness or that required adjusting, but desired behaviours emerged as well. The words and phrases used to describe desired behaviours included: Being persistent, being a 'people person' and being fair. One participant described being fair as "I always try to be fair and consistent. Like if I make a decision about something, I know staff might not necessarily like it but I will make it because it is fair and equitable". Displaying this fairness was considered to be important in the way nurse managers executed their role. The words and phrases used to describe the undesirable behaviours included: Flying off the handle; taking matters personally; keeping information; and being closed. 'Keeping information' and 'being closed' are typical examples of how undesired behaviours discovered can be transformed into' desired behaviours, by becoming for example, a sharing leader and being approachable. Participants said they had to learn to share their thoughts with others by what was referred to as: "Putting things out there for the staff to be able to see" and "It is about learning to share your thoughts with the staff - and sometimes you have things in your head but it is not always out there".
In addition to the above discovered behaviours, some participants said that they possessed positive natural leadership skills and abilities, which were confirmed for them through social interactions and feedback. One noted, "I must have had some core leadership skills. Those decision making skills were obviously there and it was not until an opportunity to demonstrate that that I realised, I can do this or that the feedback that I got from other people was positive that I was obviously doing the right thing".
Feeling confident, receiving constructive feedback and discovering strengths contributed to their positive feelings towards the nurse manager position, which in turn stimulated the learning process. The phase 'discovering behaviours' is followed by a phase of 'deciding'. An active choice is required to work on adjustments, weaknesses or perceived undesired behaviours and to expand on perceived desired behaviours.
Deciding to work on behaviours or electing not to is the third phase in the social process. The decision to work on behaviours is seen as the tipping point. Once having reached the deciding stage, many participants were motivated, and demonstrated a willingness to start making the effort to change or to adjust. The decision to make a change involved stepping out of their comfort zones and became something of a personal achievement in itself. The tipping point is a point of progression, a critical stage in an evolving situation. This study has shown that participants' decisions to work on their behaviours resulted in change, as illustrated by participants who discovered being quiet prevented them from being effective. A decision to work on becoming more vocal became personal goals. By working on these goals number of participants developed positive feelings about contributing to important conversations, as they realised that they were becoming a more assertive leader. This positive feeling started to build up to the point where participants could change their behaviours. One participant described this notion, "I don't think we are all set …You can actually change".
It became evident that at times some nurse managers would work on their behaviours and others not. This was apparent when participants spoke about improving their communication with staff: "My biggest learning? Learning, probably that what I am doing is okay". In this instance, the participant was not engaged in the learning process, as there was signs of reflection. The deciding stage in the process is crucial as this can open the way to changing or adjusting behaviours. Once having reached the deciding phase, a number of nurse managers demonstrated a willingness to undertake the effort to change or to adjust. Participants believed that this change or adjustment would help them to become a more effective leader.
Choosing deliberate behaviours is the fourth and final phase of the learning process. It is the redirection of the way nurse managers engage with their world and involves implementing and using the changed behaviours in practice. Reaching the last stage of the process involved changing attitudes and beliefs. It was found that some participants were not using the newly learned behaviours all the time, but they had the ability to channel it. "It's not about changing completely but it is about having the ability to change when you need to that is the thing". Channelling in the context of this study means using changed behaviours towards certain events instead of using it continuously. Nurse managers learned to make a switch from an existing behaviour to a newly learned behaviour depending on the issues emerging. This leads to the notion that you can, in certain circumstances, deliberately choose to change your behaviours, but these choices require enhanced self-awareness. For example, switching from being a quiet person to being a more outspoken one is a learned behaviour and this switching can be utilised in a variety of situations.
There were occasions where permanent change of behaviour was found to be challenging. One participant described this experience, "You could identify aspects of all those things in yourself but I don't know whether I have changed". "You can probably do it for a day and say, well, I'm going to be more assertive or I am going to be more supportive or I am going to be more caring, but you automatically drift back into your normal practice". A number of participants handled these challenges by practicing and experimenting with the newly learned behaviours, which eventually became engrained. It is the accumulation of the processed social interactions which leads to sustainable change. It was discovered that practising requires ongoing support from peers and the organisation of employment.
Learning to lead is a complex process, comprised of events that occur in social interactions played out in practice to which nurse managers responded to. It was found that the four stage learning process identified was essential to changing behaviours. There is consensus in the literature that enhanced self-awareness is a major step in leadership development, as it implies that a greater awareness leads to leadership learning [39-43].
Experiencing social interactions in practice could be regarded as learning opportunities as they were strongly and positively related to the actual attainment of new and altered behaviours. This notion carries similarities with the work of Van Ruyssevelt and Taveniers [44] who defined learning opportunities as "…the extent to which work stimulates growth and development of the employee" (p. 11). Social interactions or learning opportunities in practice are considered to be a precondition of leadership learning in practice. The social interactions had the potential to develop into 'key learning events'. Congruent with the experiential learning cycle of Kolb [45], the key learning events also included reflective observation and experimentation. Thus, social interactions stimulated the activation of reflection, ultimately leading to changed behaviours.
By reflecting on the social interactions, nurse managers examined existing knowledge and behaviours. The interactions were used to build on this knowledge. This notion is in accordance with earlier research in the area of workplace learning. For instance, Holman and Wall [46], Morrison, et al. [47] and Poell, Van Dam & Van Den Berg [48] argue that the workplace can be perceived as an environment which offers staff opportunities to exercise their existing skills, and also develop new knowledge and skills. However, these scholars did not mention behaviours. This is surprising because the expression of leadership is often through demonstrated behaviours [49,50]. Future research should give greater consideration to examining behaviours in leadership development.
Within the workplace, knowledge, skills and behaviours are formed in a social context, originating in social interactions and with the likelihood of being disseminated via social interactions [51,52]. Interactions with other people in the work milieu create many learning opportunities [48,53,54] but surprisingly draw little attention in the literature on nurses' continuing leadership learning. The close relationship between the response to the social interaction played out in practice and the learning situation, is often overlooked [55]. In spite of the importance of this notion, there is a dearth of research that takes context into account as an influencing factor [56]. Furthermore, within the area of leadership there is a limited understanding of the influence and connectivity of context and processes that shape leadership learning [32,57-60].
Learning arose through interactions with staff. The primary thrust of learning from formal leadership positions is concerned with developing the ability to deal with interpersonal relationships and staff issues [19,61]. Comparatively little attention has been paid in the extant literature to the role that human relations play in creating opportunities for learning [62]. As identified in this study and supported by Eraut [63], leadership development is a process that is socially constructed in practice and knowledge acquisition and behaviour change is dependent upon the relations between individuals in this process. Therefore, leadership learning is connected with being involved in social interaction, instead of being only a mental process [64]. Leadership training programs should therefore intentionally incorporate adequate opportunity for social interaction.
Behavioural change that is fully integrated occurs only through the re-examination and reconstruction of reality. A reconstructed or 'new' reality allows new behaviours to continue in the presence of the practice environment [65]. It was found that participants could revert to using their old behaviours. This might be due to the notion that some behaviours have become routine, preserving energy. In the literature, this is known as habitual action [66]. To break this habitual action it was essential for participants to ask themselves questions, such as: How did it go? What exactly happened? What did I do, what was my reaction? Can I do it differently? Would it be better to ….if…? Nurse managers engaged in the learning process asked these questions in their endeavours to learn. The answer to start the learning process may be well situated within this notion of enabling questions. Learning the skills of enquiry could consequently be the start of effective leadership learning. Therefore, it is of vital importance that nurse managers are encouraged to ask enabling questions and reflect on practice and this can be done in the workplace in a more structured way through action learning networks.
Action learning, a concept coined by Revans [67] proposes that the best way human beings learn when they work with existing organisational issues is in a group setting in real-time. Action learning is a work-based method that emphasises the importance of questioning in order to improve insight [68-70]. Leadership learning entails social interaction and reflection and both are required to improve leadership skills. Without the opportunity to reflect, a person's ability to lead is compromised and therefore not progressive [71]. Action learning is incorporated into a number of leadership programs [69,72,73] as organisations recognise that learning through reflection is important for leadership development. However, an organisational understanding of how this learning occurs has not been reached. Nevertheless, nurse managers in other studies have reported that by undertaking action learning they increased their repertoire of leadership skills [73]. Therefore, action learning is a useful approach in leadership development.
This study was set in two organisations within one Australian state. These organisations hold similar and yet distinctive cultural characteristics. Consequently, it must be acknowledged that the environments will have differences to other healthcare organisations and the results of this study are related directly to the organisations in which the research took place. However, the findings could provide valuable understandings for others who see a resemblance between this study context and their own. The substantive nature of the learning process discovered in this study creates the opportunity to test it, and by examining it, add to the value of the theory. A recommendation for future research is for a larger experimental study, with nurse managers across different organisations to test the hypothesis that nurse managers who are aware of and apply the learning process in practice develop leadership skills more efficiently than nurse managers who do not.
This study has revealed how nurse managers have learned to lead from social interactions, an under-explored area of investigation. Given the insights into the process of learning to lead that have emerged from this research, educators, organisational developers and executive (nursing) management teams may be able to use the potential of social interactions in practice as a modality for leadership learning. This presents an alternative to the more conventional class-room or online methods that take participants out of their work environment. It has been made clear that it is not effective to teach leadership to nurse managers removed from the clinical setting where leadership takes place. The learning from these learning modes may not be applicable to the issues found in the workplace. Hence, leadership development cannot be increased by didactic methods alone. Therefore, instead of fully relying on classroom and online education, we need to bring leadership development back into workplace where learning events occur. Nurse managers should be supported with opportunities to engage in the learning process through action learning sets, that promote social interactions and reflection.