Background: Tuberculosis (TB) is a major public health concern throughout the world, particularly in low- and middle-income countries. Patient delay in seeking TB care is one impediment to sustainable development goals. There is limited data on patient delays seeking health care in the study area.
Objective: To assess patient delay in health care seeking and associated factors among tuberculosis patients attending TB clinic in Hawassa city health facilities in Sidama region, Hawassa Ethiopia.
Methods: An institutional-based cross-sectional study was conducted on 196 new pulmonary tuberculosis patients aged ≥ 18 years who enrolled in the intensive phase from March 1, 2022, to April 30, 2022, in selected public health institutions of Hawassa city. All TB patients who were on Anti TB in Hawassa city health facility during the study period were included. Data were collected through pretested and structured questionnaires adopted from literature. Descriptive statistics were summarized by a table, graph, proportion, and mean or median with their corresponding measure of data dispersion.
Results: The overall magnitude of patients delay to seeking health care was 70 (40.2%) with a median health care seeking delay was 28 days. Older age [AOR: 0.24; (95% CI; 0.06, 0.88)], underweight [AOR: 2.68; (95% CI: 1.22, 5.9)], having larger family member [AOR: 3.69; (95% CI; 1.5, 8.9)], smear negative status [AOR: 3.9; (95%; 1.3, 10.9)] and having multiple health care contact [AOR: 3.69; (95% CI; 1.53, 8.90)] were independent risk factors of patient delay to health care seeking.
Conclusion: This study revealed that a significant proportion of the patients delay for more than 30 days seeking health care. Age, nutritional status, having larger family members, smear-negative status, and having multiple health care contacts were the independent risk factors for patient delay in seeking care. Therefore, raising public awareness levels and improving the diagnostic modality in public health facilities are suggested to reduce delays in diagnoses of tuberculosis.
Delay, Hawassa, Tuberculosis
Tuberculosis (TB) is a chronic disease caused by Mycobacterium tuberculosis (MTB). It affects the lungs and other parts of the body [1]. Ten percent (10%) of people infected with Mycobacterium tuberculosis progress to active TB disease during their lifetime [2,3]. People with compromised immune systems and malnutrition are more likely to develop TB. The risk of developing TB among people living with HIV is 15 to 22 times higher than in people without HIV [4]. People with under nutrition are three times more at risk of developing TB. An estimated, 2.2 million new TB cases were attributed due to malnutrition in 2019 [5].
Tuberculosis remains a major public health problem, especially after the era of HIV, globally [6]. Tuberculosis is one of the top 10 causes of death and the leading cause of a single infectious agent (above HIV/AIDS). The World Health Organization (WHO) 2019 report estimated that there were 10.0 million people who fell ill with the diagnosis of TB. A total of 1.4 million people died from TB in 2019 (including 208,000 people with HIV). But TB is curable and preventable [5]. However, patients' delay in seeking care increases the transmission of pulmonary tuberculosis and hence the burden of the disease [7].
Sub Saharan Africa region, is an area of high TB/HIV-related morbidity and mortality in the world. The indicated, mortality related to TB is greater than HIV infections, moreover, HIV and TB work together to suppress the immunity of the patients and, thereby, shorten the lifespan if there is no early treatment [8]. In South Africa, TB is a major health problem with 520 per 100,000 new cases reported to have occurred in 2018, but TB-drug resistance and HIV co-infection rates are high [9].
Ethiopia is one of the 30 High TB, TB/HIV, and MDR-TB Burden Countries with an annual estimated TB incidence of 157/100,000 populations and a death rate of 25 per 100,000 populations for 2019 [6]. Poverty and overcrowded housing are increasing the vulnerability to HIV and TB infection [10]. TB is a disease of poverty, and economic distress, marginalization, stigma, and discrimination are often faced by people affected by TB [5]. About 85% of people with tuberculosis can be successfully treated with a six-month drug regimen. Anti-tuberculosis treatment has reduced over 60 million deaths [5].
The study will be conducted in public health institutions in Hawassa city from April 1st to 30th 2022. Hawassa city is surrounded by the shores of Lake Awassa in the Great Rift Valley and is located 273 km (170 mi) far away from Addis Ababa the capital city of Ethiopia. The city serves as the capital of southern nations, nationalities, and people regions (SNNPR) and the Sidama region. Geographically it is located 130 kilometers east of Woliata Sodo, 75 kilometers north of Dilla, and 22 kilometers south of Shashemene. The city administration is divided into eight sub-cities and 32 kebeles. According to the Hawassa City Administration Health department 2013 EFY population profile, the total population of Hawassa city is approximately 0.5 million. Regarding the health infrastructure, there are 4 governmental hospitals (1 comprehensive specialized, 1 general, and 2 primary hospitals) and 11 health centers. According to the 2nd quarter HIMS report, there are 402 patients in the intensive phase of treatment.
An institutional-based cross-sectional study was conducted among new pulmonary tuberculosis patients aged ≥ 15 years who enrolled in the intensive phase from March 1, 2022, to April 30, 2022, in public health institutions of Hawassa city.
Source population: Study participants all newly diagnosed bacteriologically positive or X-ray positive pulmonary tuberculosis cases, ≥ 15 years of age, diagnosed in the study settings from March 1, 2022 to April 30, 2022.
Study population: The study participant all newly diagnosed bacteriologically positive or X-ray positive pulmonary tuberculosis cases, > 15 years of age, diagnosed in the study settings from March 1, 2021 to April 30, 2022.
Inclusion criteria: All newly diagnosed bacteriologically positive or x-ray positive pulmonary tuberculosis cases, > 18 years of age, diagnosed in the study settings from March 1, 2021 - April 30, 2022, were included in the study.
Exclusion criteria: Those who were unable to communicate, were seriously ill as well as patients aged below 18 years were excluded from the study. And also retreated and multiple drug resistance (MDR) TB patients were excluded from the study.
The sample size was determined using the single population proportion formula by assuming that: the prevalence (p) of delay in health care seeking was 49% [11,12], the confidence level of 95%, the margin of error of 5%, and the non-response rate of 10%.
Where,
z- Confidence interval of 95% which is = 1.96
p- Estimated proportion to be studied
d- Marginal error
n= 384
if N < 10,000 we can used correction formula
Then, 10% will be for non-response, 196 sample size is required.
From 4 public hospitals and 11 health center under Hawassa city administration, two hospital and eight health centers were selected by simple random sampling, by using lottery method to conduct the study. The selected facilities were Adare general hospital, Motite primary hospital, Alamura, Chefekotijebessa, Adare, Millennium, Tula, Finchawa, Tilte and Bulcha health centers.
All newly diagnosed TB patients who were on antituberculosis were recruited until the required sample size fulfill. Randomly selected health facilities and calculated by population proportion formula to conduct study (Figure 1).
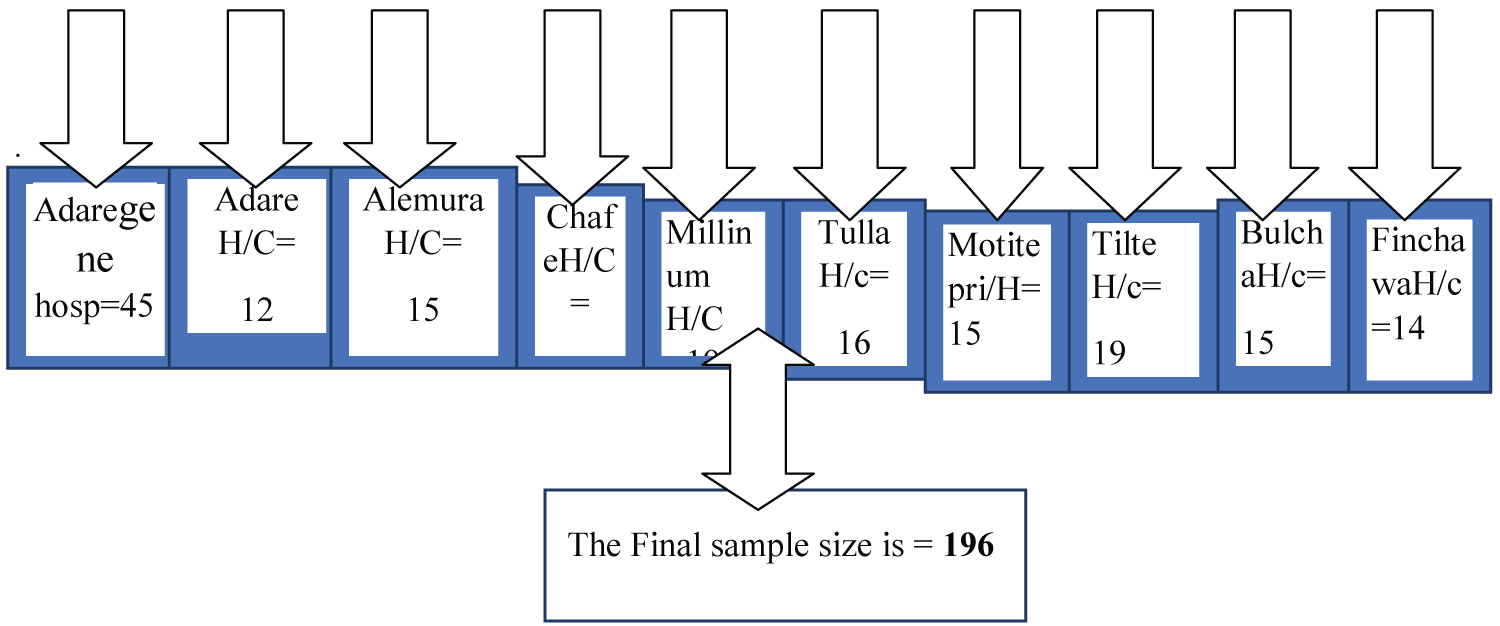 Figure 1: List of selected health facilities for study in Hawassa city adiminstration Sidama region, Ethiopia, 2022. View Figure 1
Figure 1: List of selected health facilities for study in Hawassa city adiminstration Sidama region, Ethiopia, 2022. View Figure 1
• Dependent variable: Duration in days of delay in commencing anti-TB treatment, a binary outcome of whether patients were delayed or not to initiate treatment (presence/absence of total delay).
• Independent variables: Sex, educational status, age, family size, occupation, residence, income, distance to the health facility, attitude towards traditional healers, attitude towards spiritual healing, the severity of disease, perceptions towards TB and its treatment, knowledge of TB disease.
Diagnostic delay: It is the time interval between the onset of symptoms and confirmation of TB in the patient. This includes patient delay and health system delay.
Patient delay: Period from the onset of the first symptom(s) related to pulmonary TB such as cough, fever, and chest pain to the first medical consultation.
Health system delay: The period from the first consultation to the date of diagnosis. Diagnostic delay was categorized using a cutoff value of 4 weeks by considering an acceptable patient delay and health system delay of 2 weeks each.
The questionnaire was initially prepared in English and then translated to the Amharic language, and translated back to English to check for any inconsistencies. The questionnaire consisted of socio-demographic characteristics, clinical and health-seeking behavior, and knowledge about TB and related stigma. TB registration books will be reviewed for tuberculosis diagnostic information, such as date of diagnosis, type of PTB, type of diagnostic investigation used to diagnose TB, nutritional status, HIV serostatus, patient category, and date of treatment initiation. Data were collected by trained nurses working in TB clinics.
To assure the data quality, the data collection tool was prepared after a review of relevant works of literature and similar studies. The training was given for one day both for data collectors and supervisors on a briefing on the general objective of the study, and a discussion of the contents of the questionnaire. Pre-testing was done for 5% of the tool.
Data were cleaned, coded, and entered into exported to SPSS software version 20.0 for analysis. Data were summarized using frequency, proportions, mean, median, standard deviation, and inter-quartile range. Both bivariate and multivariate logistic regression analyses were conducted to identify factors associated with patient delay. Variables significant at p-value < 0.25 level in the bivariate analysis were candidates for the final multivariate logistic regression analysis to identify factors associated with patient delay.
The strength of association was summarized by using an adjusted odds ratio (AOR), statistical significance testing was done at 95% CI and variables having a p-value less than 0.05 in the multivariate logistic regression model were considered statistically significant.
Ethical clearance was obtained from Hawassa College of Health Science and submit the Hawassa city health department a brief explanation of the purpose of the study was provided and permission was obtained and then individual consent was obtained from the patients. Participation in the study was voluntary and based on each patient's ability to give informed consent. Participants are guaranteed confidentiality of the information collected. Non-participation would not hurt care.
The research report will be disseminated through the written form to Hawassa College of Health Science and the concerned sartorial office.
A total of 196 new TB patients were included in this study. The mean age of respondents was 38.6 ± 12.4 years. More than half 115 (58.7%) were males and 149 (76.1%) were urban residents. Of the respondents, 140 (71.7%) were married and 41 (20.7%) were housewives. 35 (17.9%) had no formal education. More than three-fourths (85.5%) of the patients live in less than an hour's walking distance from the nearest health facility (Table 1).
Table 1: Socio-demographic characteristics of tuberculosis patients in public health institutions, Hawassa, Sidama, Ethiopia 2022. View Table 1
The most frequently reported symptom was cough in 62 (31.52%) patients; followed by chest pain in 54 (27.85) and weight loss in 24 (12%) (Figure 1). Nearly two-thirds of the respondents, 127 (65.2%) were smear-positive in classification and before the commencement of treatment, all of the cases were offered HIV screening tests of whom 18 (9.2%) tested positive. Regarding contact history, in the last year of TB patients, only 53 (27.2%) had contact with TB patients and 73 (37%) were underweight at diagnosis of tuberculosis (Table 2 and Figure 2).
Table 2: Healthcare seeking behavior among TB patients in Hawassa city public health facilities, Sidama Ethiopia, 2022. View Table 2
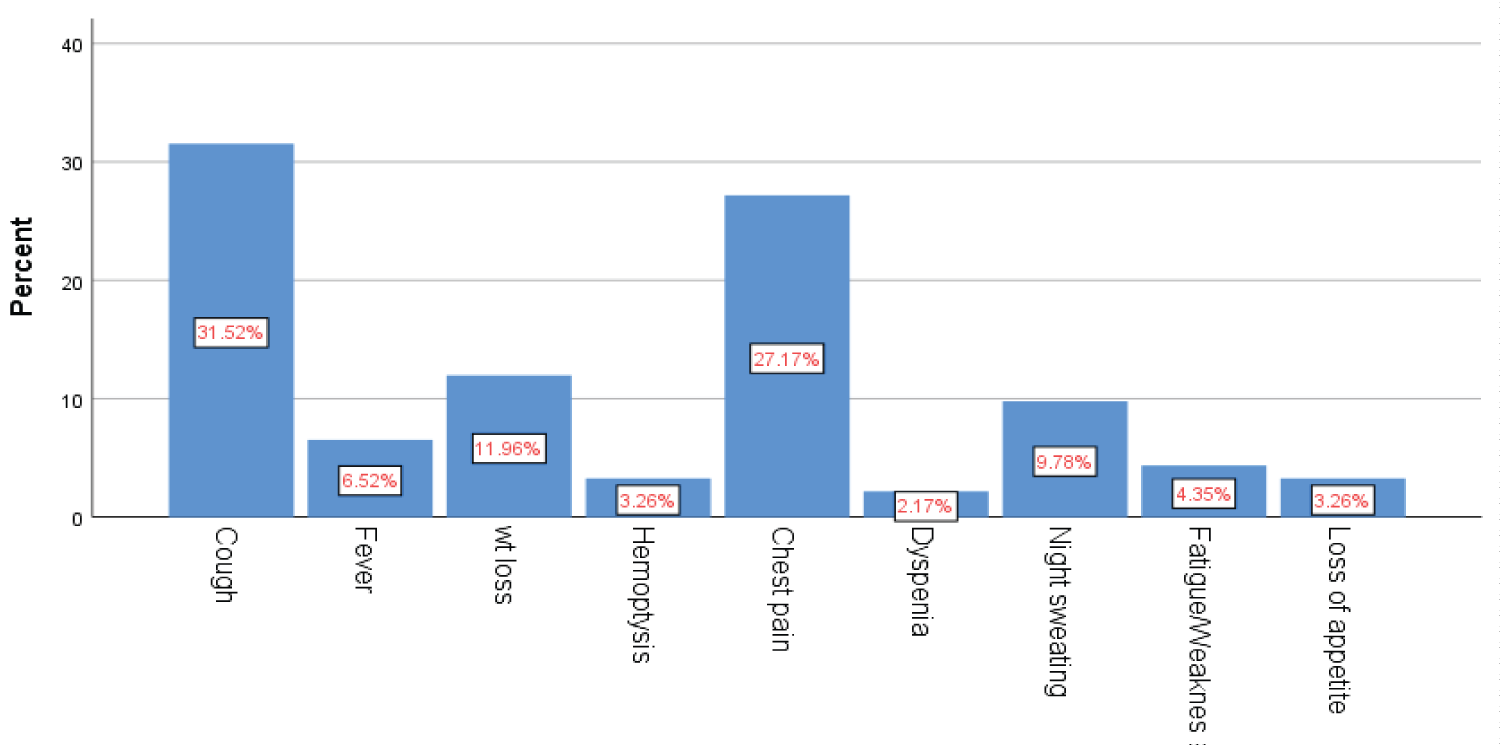 Figure 2: Complaints, which made patients seek medical care in Hawassa city public health facilities, Sidama, Ethiopia, 2022. View Figure 2
Figure 2: Complaints, which made patients seek medical care in Hawassa city public health facilities, Sidama, Ethiopia, 2022. View Figure 2
The median healthcare-seeking delay was 28 days (IQR = 21-56 days). Of the total respondents, 79 (40.2%) sought health care after 30 days of the onset of their illness. After the onset of symptoms, 96 took action including self-treatment and the use of traditional medicine before the HCF visit. Regarding the severity of the diseases at presentation, 70 (35.9%) of the patients were ambulatory in functional status before contacting a formal health facility. Of all the respondents, 172 (88%) perceived their first visit was delayed for which 131 (66.7%) and 115 (58.7%) reasoned expecting the illness to limit by itself and followed by lack of money respectively. More than three quarters, 151 (77%) of patients first contacted public health facility and 119 (60.9%) were encountered more than one health care contact before a diagnosis of TB made, and 128 (65.2%) patients were diagnosed at public hospitals. Related to community-based health insurance (CBHI) status 83 (42.4%) were a member before seeking care among respondents. 87 (44.6%) were diagnosed by sputum microscopic examination (Table 2).
Table 3: Bivariate and multivariate analysis to assess factors associated with patient delay among TB patients in Hawassa city public health facilities, Sidama Ethiopia 2022. View Table 3
The association between socio-demographic variables and delay in health seeking care was tested in a binary logistic regression both bi-variants and multi-variants analysis was done and presented in. Variables whose value less than 0.25 in bivariate analysis were a candidate variables to enter in to multivariate analysis. Variables whose values < 0.05 were considered as significant. Socio-demographic variables: age, marital status, educational status and income were significantly associated with delay in seeking health care among TB patients. Being in age group > 45 was (AOR: 1.2, 95% CI 0.006, 0.03) was 1.2 times at risk for delay in TB diagnosis (p = 0.012). Being married was two times s found to be associated with Patient delay in health seeking (AOR: 2, 95% CI 0.001, 0.13) with p-value of (p = 0.006).
Regarding respondents income it was also found to be significantly associated with patient delay. More than half of the respondents have monthly income of less than 1000 ETB and was associated with delay in health seeking (AOR: 2.6 95% CI (0.03, 1.96 with (p-value = 0.03) and educational status of respondents also significantly associated with patient (AOR: 0.02 95% CI 0.002, 0.02).
The overall magnitude of patient delay in seeking health care was 79 (40.2%) with a median healthcare-seeking delay was 28 days. Age, marital status, educational status, and low monthly income. Delay in diagnosis is still a major challenge for tuberculosis control and prevention programs in low- and middle-income settings [13-16].
The finding of this study was comparable to studies done in Chain Hubei province and South Africa showed that 40% of patients were delayed to seek healthcare [8,9]. But, it was higher than studies done in Chania reported that 13.2 to 21.54% of patients had delays in care seeking [7,17]. Similarly, it was higher than studies from Tanzania at 21%, and northwest zone of the Tigray region 31.3% of patients had delayed for more than 30 days before seeking health care [18,19]. The cultural issue, low socioeconomic standing, and low level of knowledge and understanding of the disease are all potential explanations for disparities in delay.
It was lower than studies have done Tigray region showed that 44.8% [20-24], Gamo zone (56.9%) [25-27], South Africa (56.3%) [28], Nigeria (61.8%) [29], and North Wollo Zone (62.3%) of patients consult after 30 days in [30-33]. This difference might be due to the geography of the study area and period, countries' health systems, strategies and policies, infrastructure, source population, and sample size.
In this study, the age of the patient was identified as an independent risk factor for a delay in seeking health care. Being older age was 76% likely delayed to seek health care as compared to young age patients. This is inconsistence with studies done in rural Nigeria [29,34]. Married people are more presumably to delay than those of single and divorced, people with monthly income < 1000 are more likely delay than that of having > 1000 EBR. The finding was supported by a study done in the Gamo zone [27], this could be due to the patient presenting with weight loss being more likely to delay. This might be due to those underweight patients possibly coming from low socio-economic status, given that poverty commonly influences the health-seeking behavior of individuals.
The patient who had larger family members and SNPTB are less associated as factors that are causing patient delay compared with small family size and smear positive PTB cases. The finding was not supported by another study conducted in West Gojjam Zone [35], sputum smear-negative patients were at a 58% increased risk of delay in seeking health care. In the current study, the majority of health setups used smear microscopy as the only TB diagnostic tool.
Moreover, having multiple health care contact patients were 3.7 times more delay in seeking health care as compared to their counterparts. This is consistent with a study conducted in Bale Zone, patients who visit more than 2 different types of health service providers before the start of anti-TB treatment were 3.2 times more likely delayed compared to those with 2 or less [36].
The current study has limitations: Some degree of recall bias while trying to remember the symptoms to approximate days of commencement of the symptoms, and the start of TB treatments.
The study showed the magnitude of healthcare-seeking behavior among tuberculosis patients was much delayed. Age, marital status, having low monthly income, and educational status were the independent risk factors for patient delays in seeking care. Delay in diagnosis is still a major challenge for tuberculosis control and prevention programs in low- and middle-income settings.
Based on the findings of this study the following are recommended;
For community;
✓ The community should be sensitized to seeking appropriate health care as early as possible.
✓ For health facilities;
✓ Health education sessions should be designed and provided to enhance accurate awareness dissemination on symptoms, medication options, and the curability of TB in the community, as well as among patients attending primary health care facilities.
✓ The diagnosis of TB in elderly individuals, efforts should be made to reduce these delays to stop or control the spread of TB
✓ For government and stakeholders;
✓ Provide training for health care providers and monitor the quality of diagnostic modality to reduce health system delay.
✓ The programs should take into consideration of different groups in a society such as women, elders, the illiterate, and the economically poor by using culturally convenient media of communication to ensure that the whole community is reached.