Amidst the prevailing vaccine misinformation today, there is an urgent need for new methods to verify, inform, and promote vaccination. One potential approach involves utilizing early childhood education institutions, such as preschools since every student must present an updated vaccination card for enrollment or re-enrollment. By instructing the school staff on how to verify vaccination records or conducting vaccination campaigns within schools, there is the possibility of improving vaccination rates. The study investigated vaccination coverage among children aged one to six years in public day care centers in a municipality in the Vale do Paraíba region of São Paulo. A cross-sectional study was conducted, involving the collection of vaccination cards from two Municipal Early Childhood Education Schools (EMEI) in the area. The research considered children between the ages of one and six who were properly enrolled in the EMEIs during the data collection period, with exclusion criteria related to the illegibility of vaccination cards. Ethical clearance for data collection was obtained from the Research Ethics Committee involving human subjects, and informed consent was obtained from the children's guardians. Data were collected manually by analyzing copies of vaccination cards, and vaccination coverage was assessed based on the minimum 95% coverage recommended by the National Immunization Program (PNI) in Brazil. More than half of the analyzed vaccination cards (56.8%) were found to have outdated vaccination schedules. Several vaccines failed to achieve the recommended 95% vaccination coverage, including the measles, mumps, and rubella (MMR) vaccine, measles, mumps, rubella, and varicella (MMRV) vaccine, hepatitis A vaccine, varicella vaccine, and polio vaccine. In contrast, vaccines with adequate coverage included the Bacille Calmette-Guérin (BCG) vaccine, pentavalent vaccine, rotavirus vaccine, pneumococcal vaccine, meningococcal vaccine, and others. The analysis also revealed a concerning decline in childhood vaccination coverage, posing a risk not only in terms of resurgent diseases but also to the country's future economic productivity. As Brazil's population ages, failure to ensure children's access to vaccination may hinder their neurological, psychomotor, and social development, negatively impacting the future workforce. In conclusion, leveraging early childhood education institutions for vaccination verification and campaigns presents a promising strategy to improve vaccination rates in the face of increasing vaccine hesitancy and misinformation.
Vaccine coverage, Early childhood education, Immunization campaigns
Brazil is currently the largest producer of serums and vaccines in Latin America through the Unified Health System (SUS), offering free vaccination coverage regulated by the National Immunization Program (PNI) of the Ministry of Health, which recommends a vaccination coverage of atleast 95% [1].
During the COVID-19 pandemic, the lack of information about the necessity and importance of adhering to the vaccination schedule, coupled with anti-vaccine movements and fake news, have become significant obstacles to achieving their commended 95% vaccination coverage for children, as set by the PNI. It appears that them is information that plagued the country during the Vaccine Revolt of 1904 continues to persist [2,3].
Outside the country, these numbers are no different. A Canadian study aimed at understanding the reasons behind the decline in vaccination coverage among children less than 2 years of age conducted research showing that depending on the area where a person lived, they were more or less inclined to have their child vaccinated. Additionally, areas with more immigrants were less reluctant to vaccinate their children. However, ten years later, these same immigrants were as reluctant as Canadian citizen’s themselves [4].
In addition to the problem of there surgence of previously eradicated diseases, the decline in vaccination coverage also threatens the country's economic productivity. Analyzing Brazil's age pyramid, it is clear that in a few years, the country will have a majority of adults and elderly individuals. Therefore, by not ensuring that children have access to and assurance of vaccination, the future economically active population is at risk of not developing properly in terms of neuro-psychomotor and social aspects due to the impacts of these preventable diseases, thereby reducing productive capacity [4].
The analysis of the vaccination status of the younger population is of utmost importance for monitoring and planning public health and the economy of Brazil in the coming years. Before the pandemic, evidence indicated that in 2017, immunization rates for children against 17 diseases reached the lowest levels in recent years, including measles [5]. Studies with data from 2006 to 2016 also showed a decline in national vaccination coverage for BCG, polio, and MMR vaccines in children less than one year of age [6]. Vaccines against hepatitis A, MMR, and varicella between 2014 and 2020 also experienced a decline in recommended coverage, not reaching the 95% target set by the PNI, as in the case of polio vaccines, with a decrease in coverage rates in 2015 and 2019. This information raises public health concerns in the country, regarding the potential return of diseases that were previously eradicated.
Mapping vaccination coverage makes it possible to develop intervention strategies on this issue and identify which vaccines have adequate coverage or not [7-11].
To investigate the vaccination coverage of children aged one to six years in public day care centers in a municipality in the Paraíba Valley, São Paulo.
A cross-sectional study was conducted to analyze the vaccination status of children in a sample population in Taubaté.
Data were collected by examining vaccination cards from two Municipal Early Childhood Education Schools (EMEI) in a municipality in the Paraíba Valley.
Inclusion criteria included children aged one to six years who were properly enrolled in the EMEIs during the data collection period. Exclusion criteria were based on the illegibility of a child's vaccination card.
Data collection was carried out after obtaining approval from the Ethics Committee for Human Research under protocol number [insert protocol number], along with the signing of informed consent forms by the children's guardians.
Data were manually collected in person by analyzing copies of vaccination cards at the institutions. The variables collected from the vaccination cards included the administration of vaccines against Bacillus Calmette-Guérin (BCG), pentavalent (diphtheria, tetanus, Bordetella pertussis, Haemophilus influenzae type B, and hepatitis B), polio (intramuscular and oral), pneumococcal 10V, meningococcal C, yellow fever, trivalent vaccine (measles, mumps, and rubella), hepatitis A, quadrivalent vaccine (measles, mumps, rubella, and varicella), and varicella alone, along with recommended doses according to the current National Immunization Program in Brazil.
After data collection, children were categorized as adequately vaccinated (those who had received all doses recommended by the PNI vaccination schedule) or inadequately vaccinated (those without the complete vaccination schedule recommended by the PNI). The minimum requirement for vaccination adequacy was set at 95% coverage, as stipulated by the PNI.
For data analysis, Bio Estat version 5.3, the Statistical Analysis Software (SPSS), and statistical tools from the Google Sheets application were used.
More than half of the analyzed vaccine cards (56.8%) had outdated vaccination schedules. Vaccines that did not meet the 95% vaccination coverage goal included the MMR vaccine (measles, mumps, and rubella), MMRV vaccine (measles, mumps, rubella, and varicella), hepatitis A vaccine, varicella vaccine, and polio vaccine. Conversely, vaccines with adequate coverage included BCG, rotavirus, pentavalent (diphtheria, tetanus, pertussis, Haemophilus influenzae type B, and hepatitis B), pneumococcal, and meningococcal vaccines, as shown in Table 1.
Table 1: Vaccination coverage rates observed in the children's vaccine cards at EMEI A (n = 210) and EMEI B (n = 159). View Table 1
The flow chart of the selection process for the children's vaccine cards is described in Figure 1.
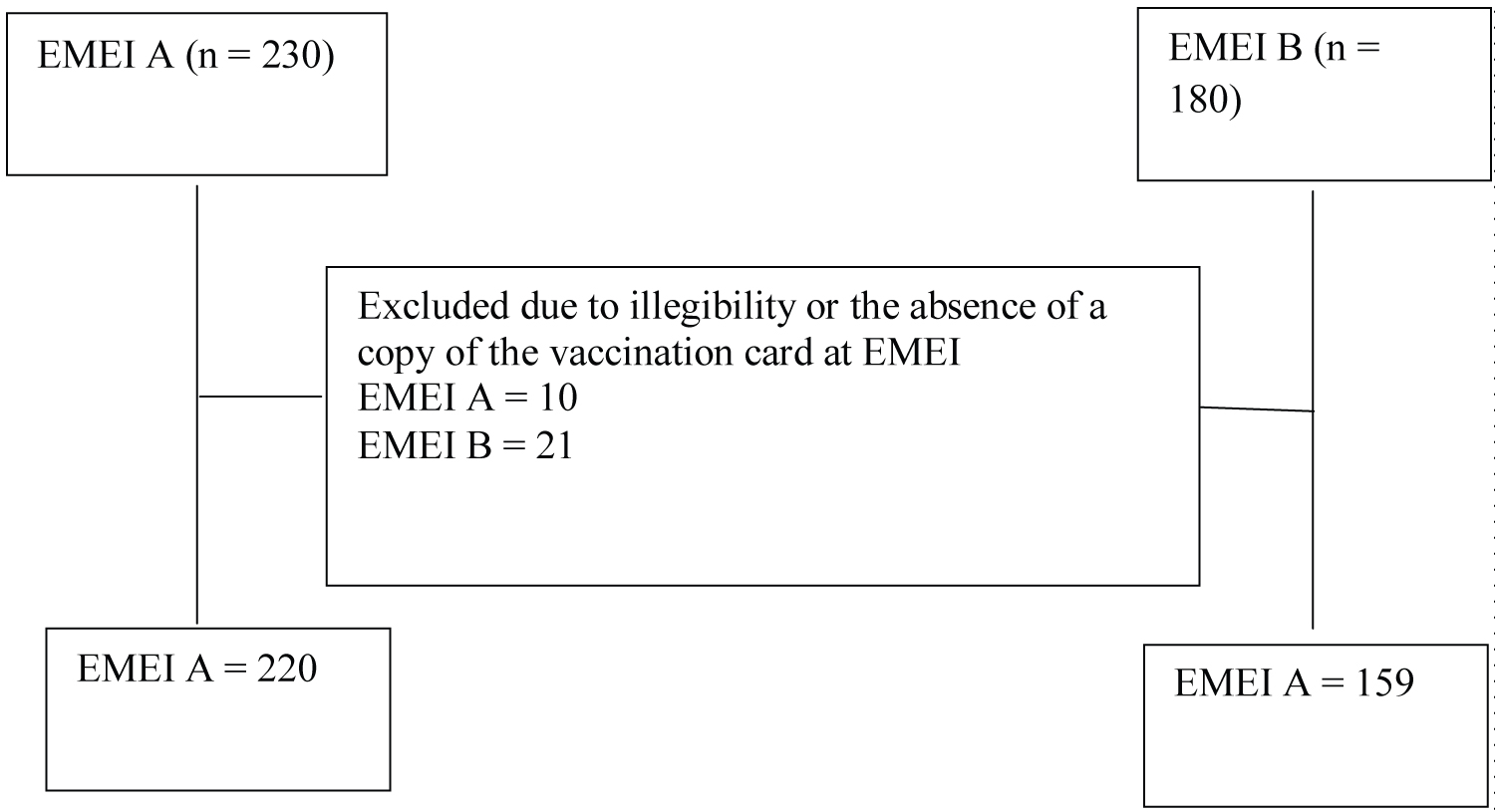 Figure 1: Selection process for the children's vaccine cards.
View Figure 1
Figure 1: Selection process for the children's vaccine cards.
View Figure 1
In line with the recent decline in childhood vaccination coverage in recent years, out of the 159 students who possessed vaccination cards, only 64% (102) had them upto date. Four vaccines fell below the recommended levels by the National Immunization Program (PNI): The rotavirus vaccine (94.3%), MMRV (91.8%), varicella (91.8%), hepatitis A (91.8%), and the polio vaccine (62%).
When analyzing both schools together, it becomes evident that out of the 379 students studied, only 197 (52%) had up-to-date vaccination cards. Varicella and polio immunizations were the most affected, with 246 (64.9%) and 196 (51.7%) students respectively receiving all the required doses (Figure 2).
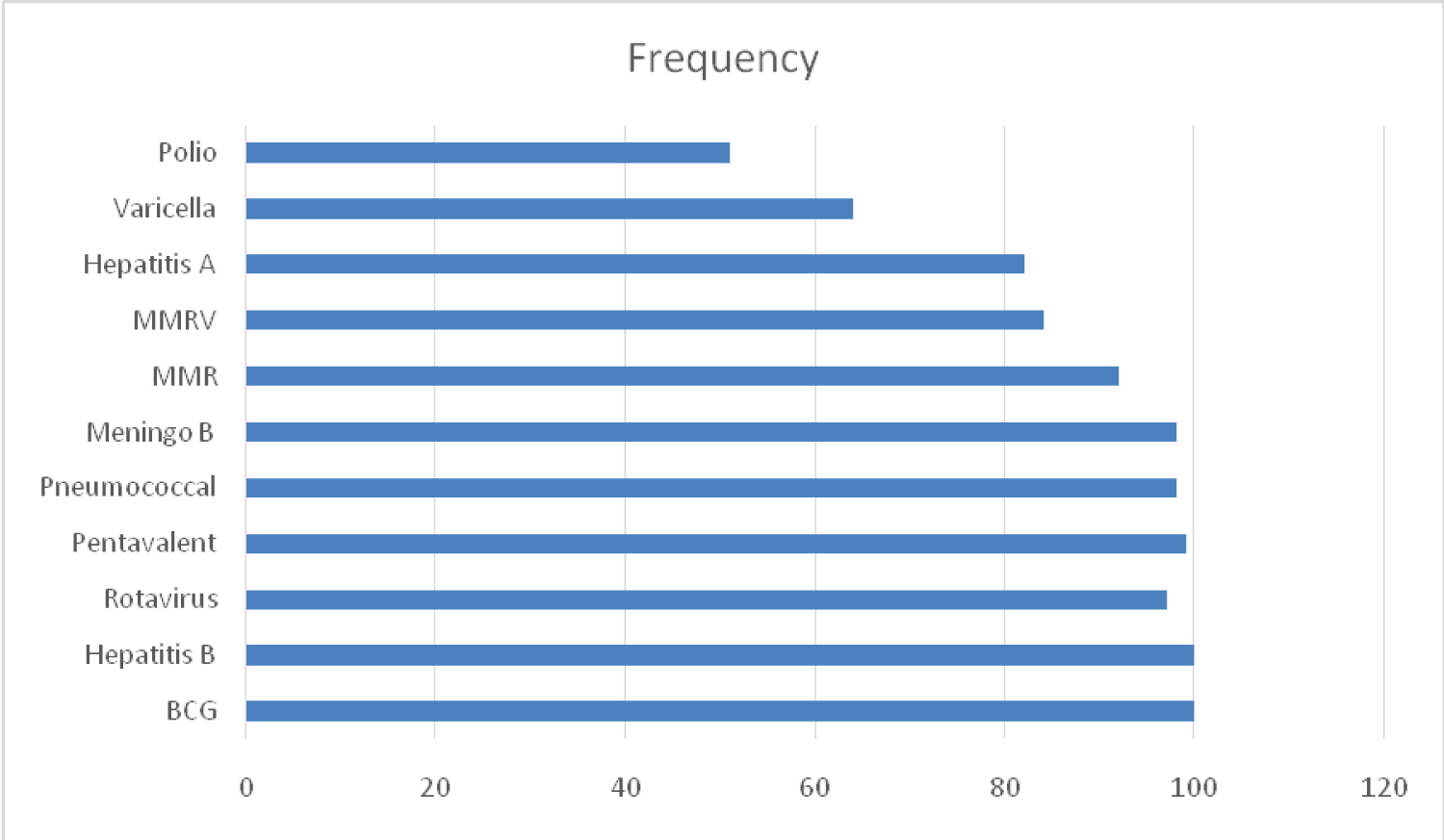 Figure 2: Frequency of vaccine doses in children's vaccination cards.
View Figure 2
Figure 2: Frequency of vaccine doses in children's vaccination cards.
View Figure 2
The DATASUS information system indicates that in 2022, the vaccination coverage in the city of Taubaté against polio was 62.96%, while varicella had a coverage rate of 64.98% in the same year. When considering all vaccines, the city had an overall coverage of 57.21%. Therefore, it is possible to conclude that the collected data align with the figures provided by the Ministry of Health [9].
These numbers are concerning as they could precede a resurgence of diseases that were previously considered eradicated in previous years. An example of this is measles, a serious vaccine-preventable disease with a high contagiousness that can lead to pneumonia, seizures, central nervous system (CNS) injuries, and even death. In 2016, Brazil obtained the certification of being measles-free; however, due to decreasing vaccination coverage, new cases emerged, and after a year of sustained transmission, the country lost that certification [10-13].
The same could happen with polio, a viral disease that, although mostly asymptomatic, in some cases can lead to paralysis with permanent sequelae, including respiratory failure and death. The last case of this disease in the country was recorded in 1989, and since 1994, Brazil has been certified as having eradicated it. However, according to the Pan American Health Organization (PAHO), there are still countries with active cases, and until this disease is eradicated worldwide, there is a chance of the virus returning, making vaccination coverage of utmost importance [13-19].
Lastly, amidst all the misinformation circulating about vaccines today, there is a need for new ways to verify, inform, and promote vaccination. One possibility is through preschools, as every student must present an updated vaccination card for enrollment or re-enrollment. By educating staff on how to perform these checks or even conducting vaccination campaigns in schools, there is potential for improvement in vaccination rates.