Myositis Ossificans is characterized by the heterotopic formation of bone inside a muscle, tendons and ligaments. This pathology is traditionally classified into two groups: Myositis Ossificans Progressiva and Myositis Ossificans Traumatica. The pathogenesis of Myositis Ossificans Traumatica is still not well established. Because it is uncommon in the maxillofacial region, there are no consolidated treatment protocols. The purpose of this study is to present a case of a patient who evolved with Myositis Ossificans Traumatica of the masticatory muscles after performing third molar extraction.
Myositis ossificans, Masticatory muscles, Oral surgery, Oral pathology
Myositis Ossificans (MO) is characterized by the heterotopic formation of bone within a specific muscle, tendons and ligaments and is rare in the head and neck region in cases of Myositis Ossificans Traumatica (MOT) [1].
MO is traditionally classified into two groups: Myositis Ossificans Progressiva (MOP) and MOT. The first, also called Fibrodysplasia Ossificans Progressiva, is an autosomal dominant disease in which heterotopic bone formation occurs in various muscles, fascia and tendons of the body. In cases of MOP, 70% of patients with a mean age of 19 years presents trismus or restricted jaw opening due to heterotopic ossification [2]. The second, also called Myositis Ossificans Circumscripta or Myositis Ossificans Localized, is characterized by the heterotopic formation of bone within a single or group of muscles submitted to one or several episodes of trauma [3-6].
MOT is well described in the orthopedic literature, affecting mainly the quadriceps femoris and brachialis anticus muscles, being rare in the head and neck region [3,6]. In maxillofacial region specifically, the muscle most affected by MOT is the masseter. This may be justified by its position more lateral to the mandible, which predisposes it to receive external traumas directly [3,6,7]. Nevertheless, there are reports of involvement of multiple masticatory muscles after trauma [4,7-9].
An English literature review revealed 42 cases of MO of the masticatory muscles. The Mean age of affected patients is 38.1 years (range, 15-73 y; median, 34 y; standard deviation, 14.2). Men were 29, whereas female patients were 12, with a ratio M:F of 2.4:1 [5].
The diagnosis of MOT is based on anamnesis (history of trauma), on clinical, radiographic and microscopic characteristics [6]. The most relevant clinical finding reported when masticatory muscles are involved, is the severe limitation of mouth opening [5,10].
In this article, the case of a patient who evolved with bilateral MOT of the lateral and medial pterygoid muscles after extraction of the four third molars will be described, with the objective of reviewing current literature, contributing to the diagnosis and treatment of these patients.
A 25-year-old male patient sought the Oral-Maxillofacial Surgery and Traumatology service at the "Dr. Mario Gatti" Municipal Hospital (Campinas-SP) in January 2016, with complaint of limitation of progressive mouth opening (2 mm), seven months after extraction of upper and lower third molars (Figure 1 and Figure 2). The patient denied prior medical problems, prior episodes of heterotopic ossification in other locations, history of family diseases and did not present hallux valgus. The hypothesis of MOP was ruled out by previous genetic test (ACVR1 gene). The patient reported using a single dose of bisphosphonate (Zolendroic Acid) and was taking Vitamin C and Indomethacin after the appearance of symptoms, a medication that had been prescribed in another service for one month.
 Figure 1: Extraoral photography evidencing severe trismus.
View Figure 1
Figure 1: Extraoral photography evidencing severe trismus.
View Figure 1
 Figure 2: A) Intraoral photography showing maximum intercuspation; B) Intraoral photography showing maximum mouth opening.
View Figure 2
Figure 2: A) Intraoral photography showing maximum intercuspation; B) Intraoral photography showing maximum mouth opening.
View Figure 2
The routine laboratory tests required were within the reference values. The C-terminal Telopeptide (CTX) test was within normality limits but showed a probable decrease bone resorption due to treatment with bisphosphonate.
Magnetic Nuclear Resonance (MRI) examination of TMJ revealed articular discs with normal signal intensity and morphology only in the closed mouth, since the other positions were not possible due to severe trismus. An inflammatory process with thickening of the medial and lateral pterygoid muscles on the right was also observed, with no collections. CT examination revealed the presence of bilateral calcification in the medial and lateral pterygoid muscles, and the right medial pterygoid muscle presented greater involvement by the pathology (Figure 3 and Figure 4). The results found in the imaging examinations, along with the clinical examination, suggested the diagnostic hypothesis of MOT of masticatory muscles.
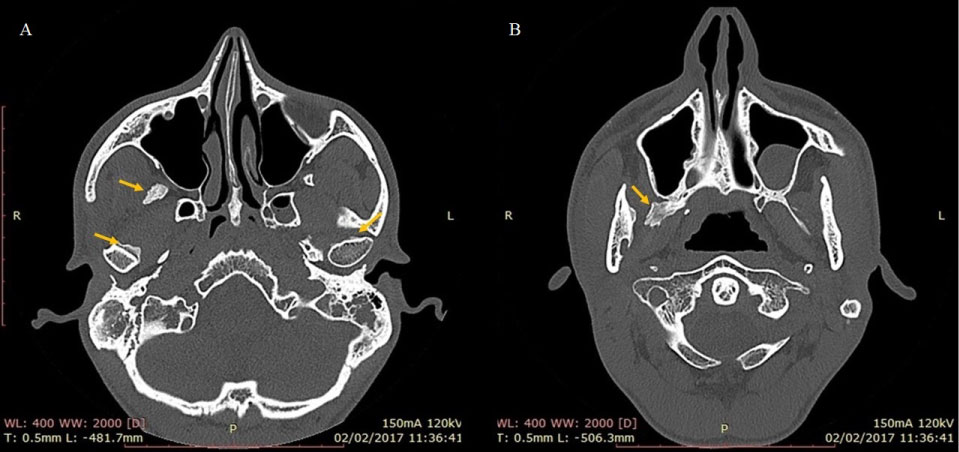 Figure 3: Preoperative CT axial plane, with seven months after dental extraction. Location of the lesion marked by the yellow arrow.
View Figure 3
Figure 3: Preoperative CT axial plane, with seven months after dental extraction. Location of the lesion marked by the yellow arrow.
View Figure 3
 Figure 4: Coronal plane of preoperative CT, with seven months after dental extraction. Location of the lesion marked by the yellow arrow.
View Figure 4
Figure 4: Coronal plane of preoperative CT, with seven months after dental extraction. Location of the lesion marked by the yellow arrow.
View Figure 4
The treatment of choice was surgical, which was performed under general anesthesia with assisted video-assisted nasotracheal intubation. Right submandibular access was made to access the mandibular branch. Vertical osteotomy of the mandibular ramus was used to access the affected right medial pterygoid muscle, and the calcified was removed mass and partial myotomy of muscle was performed. There was disarticulation of the right TMJ, with high condylectomy of the right condyle. Ipsilateral coronoidectomy was also performed (Figure 5). At this moment, the patient had maximum mouth opening of 38 mm. Bone synthesis of the osteotomy was performed with rigid internal fixation of the 2.0 system (Figure 6). Suction drains were installed to prevent hematoma formation in the region. Due to satisfactory mouth opening in the trans-operative period, no approach to the muscles affected on the contralateral side was applied.
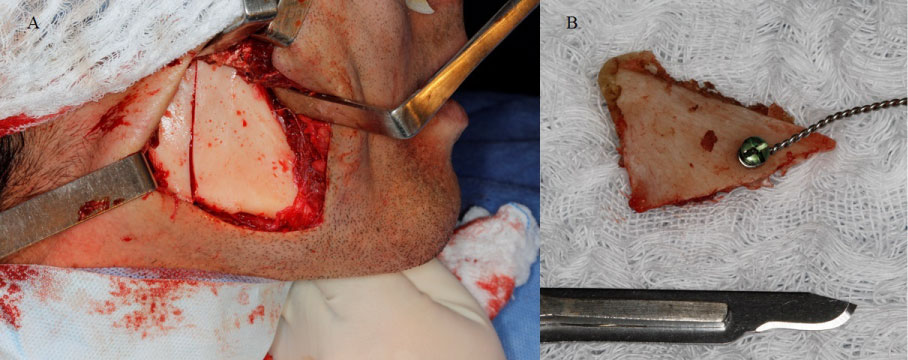 Figure 5: A) Transoperative photograph of vertical osteotomy of the mandibular ramus and coronoidectomy for access to the right medial pterygoid muscle; B) Fragment of coronoid bone removed during surgery.
View Figure 5
Figure 5: A) Transoperative photograph of vertical osteotomy of the mandibular ramus and coronoidectomy for access to the right medial pterygoid muscle; B) Fragment of coronoid bone removed during surgery.
View Figure 5
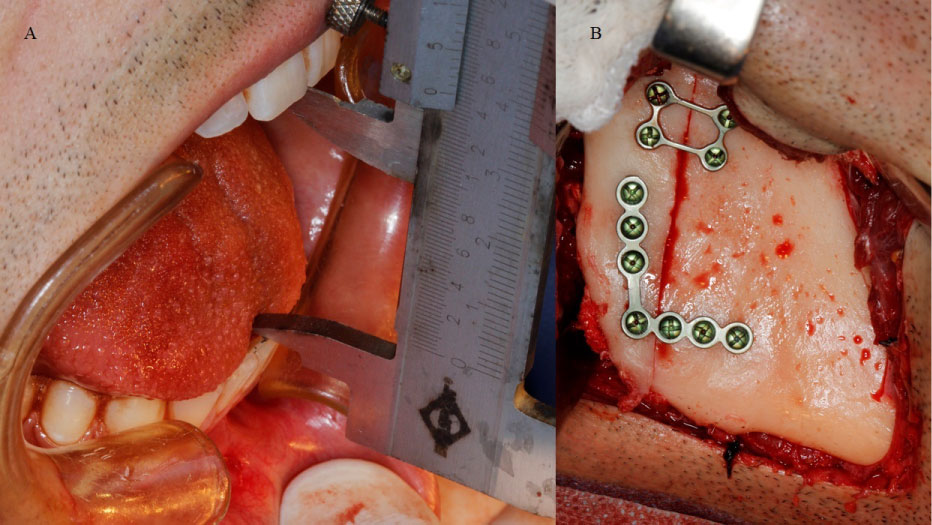 Figure 6: A) Transoperative photograph of maximum buccal opening obtained after the first surgical procedure; B) Fixation of the vertical osteotomy of the mandibular ramus.
View Figure 6
Figure 6: A) Transoperative photograph of maximum buccal opening obtained after the first surgical procedure; B) Fixation of the vertical osteotomy of the mandibular ramus.
View Figure 6
In the postoperative period, early and aggressive physiotherapy for mandibular movement was performed. Nevertheless, in the postoperative follow-up of seven days, the patient evolved with paresis of the innervated muscles by the marginal nerve of the mandible to the right and decrease of the maximum mouth opening to 19.3 mm. The patient could not perform lateral movements and mandibular protrusion.
During the first month of postoperative follow-up, the patient evolved with progressive reduction of maximum mouth opening and, as early as the second month, was not able to perform any opening movement. At that time, a new face CT was requested, which revealed recurrence of the lesion, with increased involvement of the left medial and lateral pterygoid muscles and also calcification of the left temporalis muscle.
A new surgical approach was performed four months after the first intervention. At this surgical moment, also under general anesthesia with assisted video-assisted nasotracheal intubation, bilateral submandibular access was performed to access the right and left mandibular ramus. Vertical osteotomies of the mandibular branches were used to access the bilateral medial pterygoid muscle, with removal of the calcified mass and partial myotomy of these muscles. There was disarticulation of the right TMJ, with a new high condylectomy. Coronoidectomy on the left was performed. The patient had maximum mouth opening of 50 mm in the trans-operative period. Bone synthesis of osteotomies with rigid internal fixation of the 2.0 system and interposition of abdominal fat grafting in the medial aspect of the bilateral mandibular ramus were performed (Figure 7 and Figure 8).
 Figure 7: A) Transoperative photograph of the second surgical procedure, evidencing the accesses and osteotomies performed in the right side; B) Transoperative photograph of the second surgical procedure, evidencing the accesses and osteotomies performed in the left side.
View Figure 7
Figure 7: A) Transoperative photograph of the second surgical procedure, evidencing the accesses and osteotomies performed in the right side; B) Transoperative photograph of the second surgical procedure, evidencing the accesses and osteotomies performed in the left side.
View Figure 7
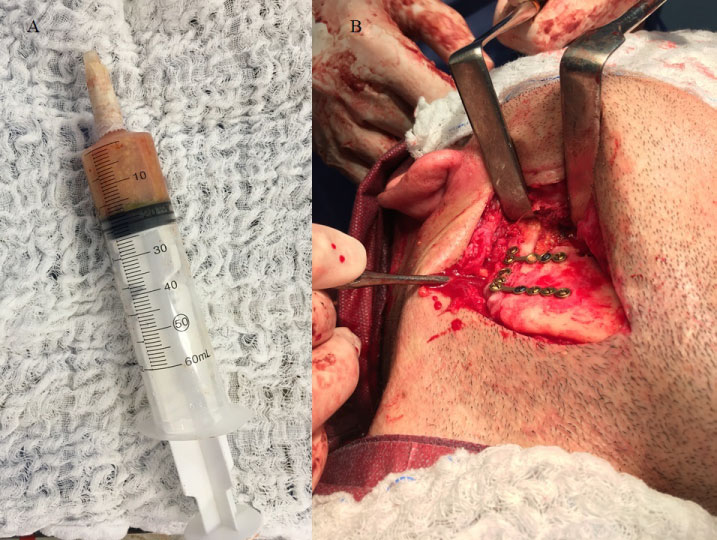 Figure 8: A) Abdominal fat graft; B) Transoperative photograph of the second surgical procedure, evidencing the interposition of a free abdominal fat graft.
View Figure 8
Figure 8: A) Abdominal fat graft; B) Transoperative photograph of the second surgical procedure, evidencing the interposition of a free abdominal fat graft.
View Figure 8
Again, aggressive and early physiotherapy was proposed in the immediate postoperative period.
After the second intervention, the patient evolved with occlusal dystopia due to posterior premature contact on the right and facial paresis (VII pair) on the left. The maximum mouth opening in the first week of follow-up was 18 mm (Figure 9). The patient has been followed for six months, with limited mouth opening (13 mm) and absence of mandibular excursion movements, even with constant physiotherapy. Even with limited mouth opening, the patient maintained acceptable masticatory and phonatory function. In the control CT scan, new heterotopic calcification was observed in areas where intervention was performed (Figure 10).
 Figure 9: Intraoral photography after the second surgical procedure, which reveals the limitation of mouth opening and occlusal dystopia.
View Figure 9
Figure 9: Intraoral photography after the second surgical procedure, which reveals the limitation of mouth opening and occlusal dystopia.
View Figure 9
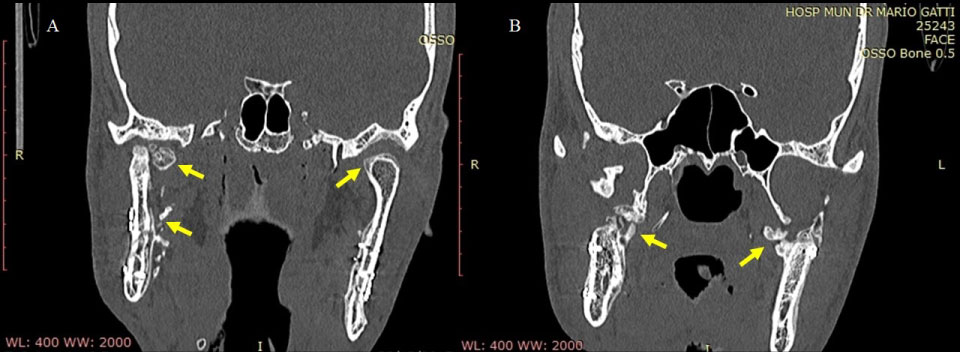 Figure 10: A, B) Coronal plane CT after the second surgical procedure, in which lesion recurrence is observed.
View Figure 1
Figure 10: A, B) Coronal plane CT after the second surgical procedure, in which lesion recurrence is observed.
View Figure 1
The most frequent symptom associated with MOT of masticatory muscles is trismus, which must be differentiated from trismus caused by abscesses, traumas, tumor lesions and by TMJ disorders [5].
Conventional radiographs are restricted in the diagnosis of MOT, as they present overlapping anatomical structures of the skull, making the visualization of lesions difficult. The most indicated image exam is face computed tomography (CT), which provides 3-dimensional images with different cutting options, aiding in diagnosis and treatment planning. The pathognomonic characteristic of MOT is a hyperdense image well delimited in the periphery with the hypodense central region, and may or may not be connected to the adjacent bone [5].
On histopathological examination, MOT lesions present a peripheral zone containing mature lamellar bone and active osteoclasts, an intermediate zone composed of cartilage and osteoid material and a central zone with proliferation of fibroblasts and mesenchymal cells [5,7,9,11].
Laboratory tests are generally within normal standards, except for a few reported cases that presented elevation in alkaline phosphatase [5].
Some authors presented four stages for MOT, according to histological and radiological findings. The initial phase shows proliferation of capillary and mesenchymal cells at the wound periphery. Due to the lack of calcification, this phase is invisible on radiographic examination. Subsequent phases exhibit classical radiographic changes and include the incipient bone production phase (1-2 weeks), the intermediate phase (4 weeks) and the late phase (6 weeks). Radiographically, the mature lesion is characterized as a central radiolucency surrounded by a bone margin [3,5,12,13].
Etidronate administration has been described as an auxiliary treatment of MOT of masticatory muscles despite the long-term side effects already known as osteomalacia. This medication is a bisphosphonate that adheres to hydroxyapatite, avoiding the aggregation, growth and calcification of crystals. Conner & Duffy (2009) [7] used this medication at the dose of 400 mg orally, 3×/day, during the period of 2-3 postoperative months.
Celecoxib (200 mg orally, 2×/day for 20 days) and Indomethacin (50 mg orally, 2×/day for 20 days) are non-steroidal anti-inflammatory drugs used to prevent heterotopic bone formation following hip surgery [14]. These medications have action on the pre-osteoblasts, inhibiting their differentiation [7].
Low radiation doses have been described to prevent heterotopic bone formation following pelvic surgeries, inhibiting the differentiation of mesenchymal cells into osteoblasts [15].
Ascorbic Acid (Vitamin C) appears to act favorably in the stabilization of MOP. Its mechanism of action is attributed to a decrease in the synthesis of procollagen type III during the inflammatory process, thus reducing the formation of heterotopic ossification [16].
The use of steroid injections presents anecdotal evidence [7].
Warfarin may prevent the formation of heterotopic bone by interfering with the production of vitamin K-dependent osteocalcin; however, hemostatic changes should be considered [7].
Despite the described clinical treatments, the surgical treatment method, with excision of the ossified mass, presents higher casuistic in literature for MO of masticatory muscles [5]. This procedure may be associated with the interposition of autogenous or alloplastic grafts or alloplastic prostheses of temporomandibular joint (TMJ) [5,6,12,17,18].
In the differential diagnosis of MOT, Osteoma should be distinguished from Osteochondroma, Chondroma, TMJ Ankylosis, Rhabdomyoma, Nodular Fasciitis, Soft Tissue Sarcoma, Chondrosarcoma and Hemangiomas [3,19].
In the current literature, there is no evidence to justify the involvement of a specific muscle in cases in which several muscle groups have been injured. As an example, in this case-report, even after performing submandibular accesses, the masseter muscle was not affected by MOT.
Extraction of third molars, cervical neck immobilization, absolute alcohol injections for treatment of trigeminal neuralgia, prolonged mouth opening for dental procedures, direct blunt trauma, odontogenic infection and anesthetic infiltration are the agents described in literature that may trigger the MOT condition [1,4,8,9,12].
In most cases, no alterations in laboratory tests of the patient diagnosed with MOT are observed. Only a few cases in the orthopedic literature and two cases with involvement of the head and neck region have shown elevation of serum alkaline phosphatase; however, it has been proposed that this alteration is a consequence of the disease and not its cause [7].
Several imaging tests are described as complementary diagnostic tests for MOT, such as X-ray, CT and Magnetic Resonance Imaging (MRI). For adequate surgical planning, Torres, et al. [6] have suggested that CT associated with the use of biomodels improves the visualization of the shape and location of lesions and can simulate the best localization of incisions and osteotomies, minimizing surgical risks. Conner and Duffy (2009) [7] indicate periodic CT scans every 2-3 months to evaluate the progression and confirm the interruption of the ossification process.
Some non-surgical therapies for the treatment of MOT have been proposed but there is no clinical evidence of their effectiveness [7]. Administration of local magnesium sulfate injections associated with the use of oral magnesium lactate, low doses of radiotherapy, use of bisphosphonates, indomethacin, Celecoxib, warfarin and injections of steroidal anti-inflammatory drugs were described in literature; however, without consensus regarding dosage and results obtained [1,7,14,20,21].
The surgical modality of treatment, with early and complete excision of the involved muscles concomitant with additional procedures to avoid the relapse of MOT is the therapy most accepted by most surgeons [1,6].
There are no surgical treatment protocols described, being reported in literature only the removal of bone mass, the removal of all involved muscle, condylectomy or coronoidectomy and the interposition of grafts. With these treatments, present satisfactory results with a reduced follow-up time, but evolving with recurrence, in most cases, in the long-term follow-up time. Some authors suggest only incisional biopsy and functional exercises [5].
The timing of the surgical approach is also controversial, with some authors indicating the early approach (3-6 weeks after trauma), while others recommend waiting for the complete lesion development [5].
In the case described, the evolution of the disease was rapid, with severe trismus 4 weeks after extraction of the third molar and after the first surgical intervention for MOT.
For intubation of patients with MOT, the aid of fibro-optic device is necessary due to the limitation of mouth opening and impossibility of laryngoscopy [5,12]. Thus, the presence of specialized equipment and the use of suitable optical devices are imperative, making the procedure more expensive.
The interposition of graft free of abdominal fat or buccal adipose body obliterates the dead space, preventing the formation and organization of hematoma, which would contribute to the relapse of MOT [12,17]. The use of suction drains in the gap formed after resection of the bone mass also prevents the formation of hematomas and, consequently, the recurrence of the lesion [3]. Other authors suggest the interposition of Silastic [18] or silicone slides [8] to prevent recurrence of MOT. In this case-report, all these procedures (except Silastic interposition) were performed in an attempt to avoid relapse.
The use of alloplastic TMJ prostheses has also been reported to prevent relapses and have the advantage of returning the posterior height of the mandibular branch when this occurs in bone resections [1,5].
It is consensus in literature that aggressive and early physiotherapy should be instituted in the immediate postoperative period, preferably assisted by the professional [3,6,12,17]. This procedure aims to prevent recurrence of MOT.
Another relevant point observed in the patients with MOT in maxillofacial region is that there is a marked decrease in the muscular strength of the masticatory muscles, which do not respond well to physiotherapy maneuvers for the performance of mandibular excursion movements. It was observed in this clinical case, in addition to the difficulty of mouth opening, a great difficulty of the patient in promoting the mouth closure after maximum opening achieved during physiotherapy sessions, with true muscle stiffness whether in a closed or open mouth position.
The postoperative follow-up of cases described in literature is deficient, with most articles presenting less than one year of follow-up [5]. This fact may mask the real recurrence rate, which may predict a worse prognosis for MOT cases of masticatory muscles.
It could be concluded that MOT of masticatory muscles is a rare pathology of difficult handling and treatment, which can lead patients to significant functional limitations of the stomatognathic system. Management is challenging due to the various forms of manifestation and variety of masticatory muscles involved, and there is no established treatment protocol.
None.
The Myositis Ossificans Traumatic is a rare entity in the head and neck region and their treatment remains a challenge for maxillofacial surgeons. Therefore, all cases of this pathology should be reported to aid in the treatment of the disease.