Bisphosphonate medications are widely prescribed for the treatment of osteoporosis and cancer metastases to bone. However, these medications are among a list of agents which are implicated in medication related osteonecrosis of the jaw (MRONJ). A variety of non-surgical and surgical approaches are indicated in the treatment of this condition, depending on disease severity. This case series demonstrates the success of the mylohyoid flap in combination with platelet rich fibrin (PRF) in achieving closure of necrotic bony defects.
Medication related osteonecrosis of the jaw (MRONJ) is a condition that manifests as exposed, necrotic and non-healing jaw bone, in patients who have been treated with bisphosphonates, denosumab, chemotherapeutic agents, anti-angiogenic drugs, tyrosine kinase inhibitors, thalidomide and steroids [1-4]. The mandible is twice likely to be involved than the maxilla [4]. Following theories have been proposed to discuss the pathogenesis of MRONJ:
1. Inhibition of osteoclastic function and increase in osteoclast apoptosis, which negatively affects bone healing and remodeling [4].
2. Inflammation and infection secondary to bioflims [4-6].
3. Interruption of vascular supply leading to osteonecrosis [4].
There are four stages of MRONJ: Stage 0 to stage 3, with increasing severity of clinical appearance [4]. Based on the staging and severity of the condition, MRONJ can be managed surgically and/or non-surgically [4]. Non-surgical therapeutic approach includes pain control, antibacterial mouth rinse, systemic antibiotics, pentoxifylline and alpha-tocopherol [7]. Surgical treatment comprises of debridement and sequestrectomy, resection and reconstruction [7]. Although, surgical treatment is warranted for stage III MRONJ, the extent of surgery is debatable [8]. Moreover, the recommendations for surgical treatment of stage I and II MRONJ vary in the literature [8,9]. The aim of this case series is to present a surgical approach utilizing mylohyoid flap along with platelet rich fibrin (PRF) combined with antibiotics and chlorhexidine mouth wash to manage patients with stage II and advanced stage I MRONJ. To our best knowledge, this is the first case series reporting the use of local vascularized soft tissue flap along with PRF in treating patients with MRONJ.
Three patients treated for MRONJ at the Department of Oral and Maxillofacial Surgery was included in this retrospective analysis. All three patients had stage II MRONJ, which is characterized by exposed and necrotic bone (2.5 cm-4 cm) along with symptoms such as pain and erythema either with or without purulent drainage as seen in Figure 1a and Figure 1b [4] . Patient characteristics are summarized in Table 1 and Table 2.
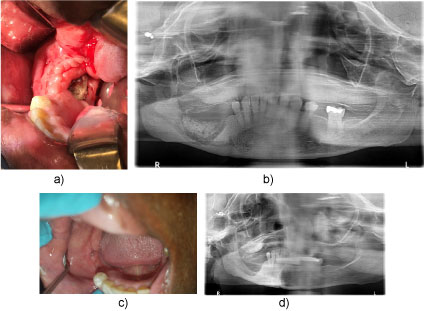 Figure 1: Extraoral view of a 23-old-male patient with oligodontia and class III anomaly before treatment.
View Figure 1
Figure 1: Extraoral view of a 23-old-male patient with oligodontia and class III anomaly before treatment.
View Figure 1
Table 1: Patient Demographics and Medication History. View Table 1
Table 2: Triggering Factors and Symptoms. View Table 2
All three patients were treated with chlorhexidine and antibiotics peri-operatively. They received IV antibiotic prophylaxis with ampicillin and sulbactum an hour before the surgery. Clindamycin was administered in penicillin allergic patients. The antibiotics were continued for seven days post-operatively. Surgical procedure was performed under general anesthesia. The surgical technique consisted of raising a mucoperiosteal flap to expose the necrotic bone. The flap was extended anteriorly and posteriorly a little beyond the affected bone. The necrotic bone, including 2 to 5 millimeters of surrounding healthy margins was removed until bleeding bone was encountered. Next, smoothing of the sharp bony edges with a pineapple bur under normal saline irrigation was performed, and care was taken to preserve the continuity of mandible. Then a mylohyoid flap was prepared by exposing the mylohyoid line and separating mylohyoid muscle. The detached muscle was then mobilized over the defect for tension free closure. Extreme care was taken to preserve the lingual nerve and submandibular duct throughout the procedure. PRF was prepared using autologous blood and was placed over the bone. The mylohyoid muscle was secured to the buccinator muscle with 4-0 Vicryl mattress sutures. The mucoperiosteal flap was re-approximated to obtain a double layered closure (mylohyoid muscle and mucoperiosteum). Primary watertight closure was achieved in tension free manner. All patients were evaluated post operatively at: 1 week, 3 weeks, 2 months, 6 months and 1 year.
This case series showed that use of mylohyoid flap and PRF are associated with complete healing after performing sequestrectomy in patients with stage II MRONJ. The mylohyoid flap is a vascularized soft tissue flap that can be used for reconstruction of small sized mandibular defects [10,11]. It provides an additional soft tissue coverage over the debrided bone, thereby promoting healing. Consequently, reducing the risk of dehiscence and the rate of disease recurrence. PRF is a combination of an autologous platelet concentrate and immune cells [12]. It plays an essential role in releasing cytokines and stimulating defense mechanisms [12]. Therefore, it is also known as an "immune node" [12]. Additionally, it has platelet derived growth factors (PDGF), transforming growth factor beta (TGF-β), epidermal growth factors (EGF) and vascular endothelial growth factors (VEGF) which promote angiogenesis and aids in the healing process [13,14]. Furthermore, PRF functions as a membrane when placed over the bone prior to soft tissue closure [15]. Alternatively, the pedicled buccal fat pad can be advanced to cover not only posterior mandibular defects but also posterior maxillary defects [16,17]. The stem cells in a highly vascularized fat tissue differentiate into endothelial progenitor cells which are responsible for the formation of new blood vessels [16]. Hence, double layered closure with the buccal fat pad has proven to be very successful [18].
In our case series, all three patients had stage 2 MRONJ, which was limited to the posterior mandible. The treatment strategy addressed the pathogenesis of MRONJ in the following manner:
1. Discontinuation of the offending medication and drug holiday after discussion with prescribing physician to improve osteoclast function and bone remodeling.
2. Administration of prophylactic and post-operative antibiotics to address inflammation and infection secondary to biofilms.
3. Use of pedicled soft tissue flap along with PRF after removal of necrotic bone improved the vascular supply supporting the healing process.
All patients reported resolution of symptoms and demonstrated complete healing of the surgical site with no recurrence, as seen in Figure 1c and Figure 1d. None of our patients experienced any complications. Some of the reported complications of this procedure are damage to the lingual nerve and salivary gland duct [10,11]. However, this therapy can only be employed in select MRONJ cases such as small sized mandibular defects.
The mylohyoid flap and PRF played a vital role in the treatment of MRONJ. Nonetheless, more studies are required to demonstrate the success of mylohyoid flap and PRF in managing MRONJ.
We acknowledge the ongoing support of the Chairman of the Department of Oral and Maxillofacial Surgery Dr. Hillel Ephros, for providing great patient care and excellent resident education. We also want to thank Dr. Amin Khoshnevisan for his contributions in finding patient information through electronic records.