The aim of this study was to analyze the etiology, clinical presentation management and treatment modalities by the protocol of management of severe odontogenic infections in patients undergoing to the emergency of Dr Angel Larralde Universitary Hospital in Valencia-Venezuela during 15-y period.
This retrospective study was done from January 2001 to December 2016 and included 1124 patients with a mean age of 30.23 yrs. Data collection included age, gender, site of infection days of hospitalization, white blood cell count, temperature on admission, past medical history, treatment administrated length of hospital stay and results of bacteriologic sampling. The SPSS 20.0 software (IBM, Inc., Armonk, NY) was used for all statistical analyses, with a threshold for statistical significance set at p < 0.05.
Majority of patients were in age group of 21-29 years, followed by 31-55 years. Out of total of two groups with 1124 patients, 580 patients (51.60%) were males and 544 patients (48.40%) were females. Toothache was the most common symptom found in 900 patients (80.07%), followed by neck swelling in 204 patients (18.19%), trismus in 846 patients (69.75%), In term of management incision and drainage were done in 252 patients (89.67%). Mean hospital stay was 5.2 days with a minimum of 4 days and a maximum of 15 days. All the patients were drained and removal the etiology under local anesthesia.
This paper described the management of odontogenic infections in a public Hospital in Venezuela and suggests that the early dental extraction, incision and drainage coupled with intravenous antibiotic therapy, is the most effective treatment.
Odontogenic infections, Maxillofacial space, Incision, Abscess, Drainage
An important feature of suppurative odontogenic infections is that they are typically polymicrobial in nature, with mixed aerobic and anaerobic bacteria present. However, the anaerobes generally outnumber aerobes by a factor of two to four folds [1-3].
Early recognition and management of orofacial infections is mandatory. The majority of orofacial infections spread along the contiguous facial planes, leading to more severe infections [4].
Treatment of these infections is challenging because potentially fatal complications such as sepsis, airway obstruction, cavernous sinus thrombosis, necrotizing fasciitis, and mediastinitis can occur. Treatment of odontogenic infections is mainly surgical aiming at removal of the source. Root canal therapy, dental extractions and incision and drainage of infected spaces are usually supported by antibiotics and other measures to improve patients' defense [5].
Maxillofacial infections (MI) are characterized as polymicrobial, endogenous, opportunistic, and dynamical and mixed (aerobic and anaerobic bacteria) [6]. The literature shows that MI affects mainly male patients either in adult or child populations [5,6].
In this study all odontogenic maxillofacial infection seen over 15 year period were analyzed to determine whether factors such differences in antibiotic therapy, timelines of exploration and drainage and presence or absence of underlying disease processes affected the outcome.
During the last 15 year, there were no detailed studies about odontogenic maxillofacial infections in Venezuela. However, severe maxillofacial odontogenic infections are prevalent. After treatments are completed, all related documentation is archived centrally. This central accumulation information allows for the study of time trends in disease incidence as well as examination of risk factors and different aspects of disease management. Having this considerable amount of data available presents a unique opportunity for retrospective analysis, which has scientific value as well as clinical implications.
The aim of the present study was to analyze treatment modalities and results in patients with severe odontogenic maxillofacial infections treated by our protocol in the Dr. Angel Larralde Universitary Hospital, Valencia Venezuela, between August 2001 and May 2016 during a 15-year period.
In this study 1124 patients were retrospectively evaluated, a descriptive study was conducted including all patients with odontogenic maxillofacial infection. All patients admitted to Oral and Maxillofacial Service at Dr Angel Larralde Universitary Hospital was studied for a 15 years period.
The patients that were included after confirming the following inclusion criteria: 1) The presence of severe odontogenic infections; and 2) The need for hospital admission. The usual criteria for hospital admission in this type of pathology include: Trismus (defined as an oral aperture of less than 40 mm), dysphagia, odynophagia, dyspnea, high fever (over 38 ℃), worsened general condition or the need for hospital control of concomitant systemic diseases. One or more of these admission criteria were required for inclusion in the study.
All patients underwent surgical treatment such as drainage of underlying infiltrates and extraction of a causal tooth either under local or general anesthesia (Figure 1).
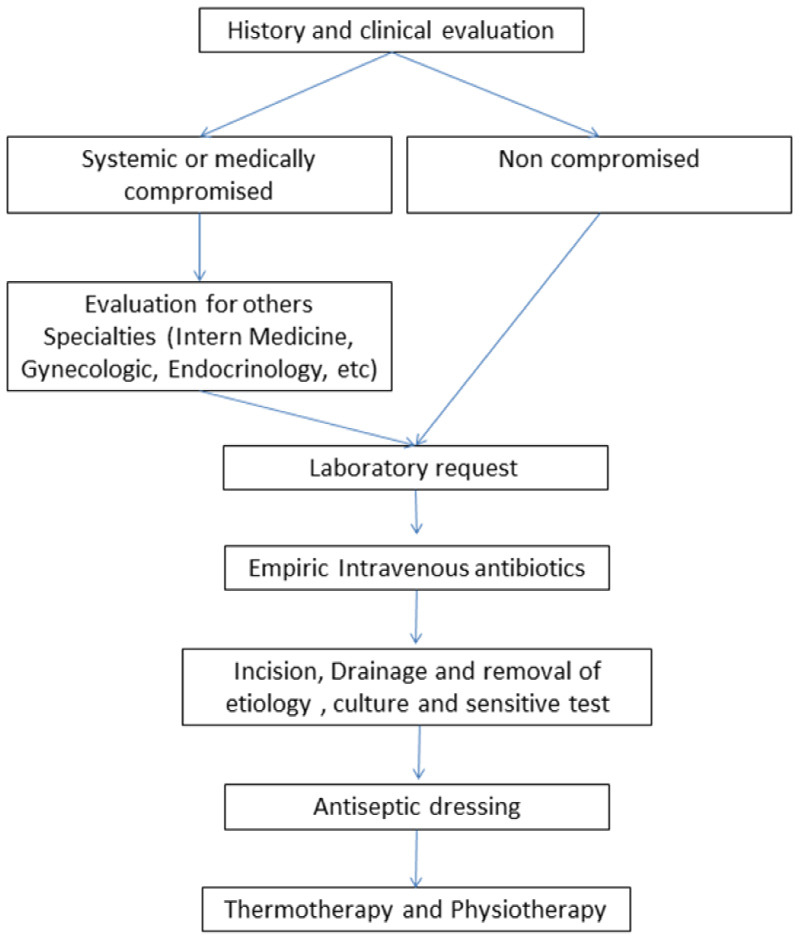 Figure 1: Protocol for the management of Odontogenic infections in Dr Angel Larralde Universitary Hospital.
View Figure 1
Figure 1: Protocol for the management of Odontogenic infections in Dr Angel Larralde Universitary Hospital.
View Figure 1
In addition, the following data were also collected: Age, gender, presence of systemic diseases, smoking history, and treatment-related information such as time of first appointment, length of hospital stay, type of treatment provided, and microbiology.
All the medically compromised patients and pregnant females were also included. Preoperative image exams were obtained providing radiographic diagnosis for the infection cause.
According to cited criteria 1,077 medical records were included in the study. The SPSS 20.0 software (IBM, Inc., Armonk, NY) was used for all statistical analyses, with a threshold for statistical significance set at p < 0.05. The categorical variables were represented as frequencies and percentage.
In this paper we use the anatomical space classification of infection for Grosinsky, et al. [7,8].
The follow-up protocol was weekly until completing one month postoperatively, and after that it was scheduled once every month, for at least 6 months. However, this protocol was not followed in all cases, because some patients did not return, this patient was not recorded in the study.
This study was approved by the Carabobo University and Dr. Angel Larralde Universitary Hospital IRB and all participants signed an informed consent agreement. (Bioethics and Human Research committee approval N°, 17-1338). All patients who were attended in the Emergency area are necessary that they sign an informed consent for the use of their information in studies of the institution.
In our study, Out of total 1124 patients, 580 patients (51.60%) were males and 544 patients (48.40%) were females. The mean age of patients was 30.23 years, with a minimum age of 2 years and a maximum of 92 years (Table 1). Majority of patients were in age group of 21-29 years, followed by 31-55 years (Table 2). Only 5% of the women were pregnant in second trimester of pregnancy.
Table 1: Distribution of patients for sex. View Table 1
Table 2: Age group (years) distribution. View Table 2
Incidence of all odontogenic infection was 1124-75 cases each year, with a maximum of 78 cases and minimum of 66 cases per year. Distribution of odontogenic maxillofacial infections during the 15-y period is shown in Figure 2.
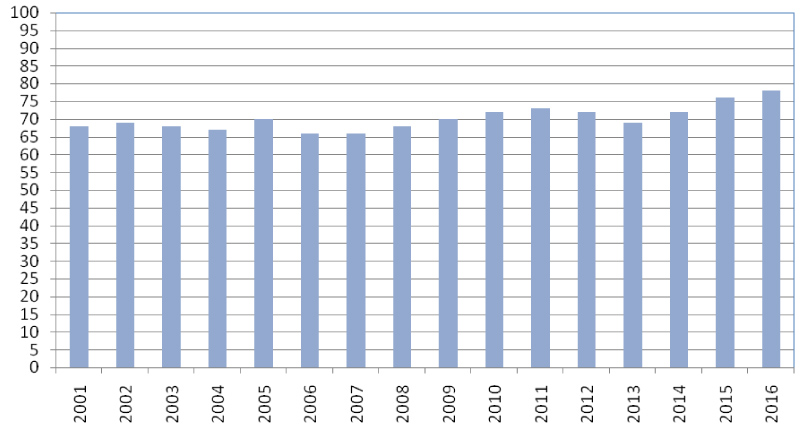 Figure 2: Incidence of maxillofacial infection.
View Figure 2
Figure 2: Incidence of maxillofacial infection.
View Figure 2
On average, maxillofacial odontogenic infections accounted for 6.7% of all Department of Oral and Maxillofacial Surgery patients who were hospitalized each year.
Toothache was the most common symptom found in all 1124 patients (80.07%), followed by neck swelling in 204 patients (18.19%), trismus in 846 patients (75.21%), facial pain in 844 patients (75.09%) and odynophagia each in 844 patients (48.75%), fever in 665 patients (58.72%), airway difficulty in 523 patients (43.77%) and torticollis in 215 patient (18.86%) (Table 3).
Table 3: Distribution of dental units causing odontogenic infections. View Table 3
In term of management incision and drainage were done in 1008 patients (89.67%). All 1124 patients were given broad spectrum intravenous antibiotics which were later changed based on culture and sensitivity report.
All surgical procedure was performed within the first 6 h after hospital admittance. An intraoral incision was made in 104 cases, extraoral incision were made in 1008 patients. Twelve patients drained through the postexodontic alveolus.
The most common bacteria isolated were Viridans streptococci, Prevotella, Staphylococci, and Peptostreptococcus. Viridans streptococci accounted for 28.99%, Prevotella for 21.2% (57 isolates), Staphylococci for 8.9% and Peptostreptococcus for 4.8% from the total isolates. Culture and sensitivities were reviewed on 1012 patients; however, anaerobic sensitivities are routinely not performed at this institution.
The 97.88% of all cases of maxillofacial infections were admitted for surgical and pharmacological management, the rest of cases were ambulatory. Mean hospital stay was 5.2 days with a minimum of 4 days and a maximum of 15 days. 37.2% of the patients were hospitalized for more than 8 d.
The complications observed during hospital stay were also documented. Following hospital discharge, we collected information on those patients. Complication occurred in 1% of cases: 2 patients had Mediastinitis and need to be treated by Department of surgery, two patients had necrotizing fasciitis. There was no death during the 15 years of study.
Of all patients, 379 (36.1%) were smokers; 128 were females (33.7%) and 251 were males (66.2%). Thirty patients (2.7%) had diabetes mellitus, 59 (5.4%) had arterial hypertension, and 41 (3.8%) patients were pregnant women.
Patients with diabetes mellitus not controlled and malnutrition conditions had longer hospital stays than patients without systemic conditions. A strong correlation of variables between diabetic status and hospitalization could be established and was determine a more time for recovery of maxillofacial infection.
Odontogenic infections are among the conditions most commonly treated by oral and maxillofacial surgeons. These infections affect a large portion of the population, and can give rise to serious complications if not treated quickly and adequately. Thus, the importance of infections of dental origin is their high incidence and morbidity [9-13].
In our series of cases the mean patient age was 30.23 years, which is somewhat younger than in other studies which a mean of 40.3 years [14].
Epidemiological surveys are conditioned by socioeconomics profiles, geography, inadequate nutrition, educational level, health services access [12]. In our study the systemic disease nutrition and the access to odontology service conditioned the odontogenic infection.
The literature in replete with many reports on odontogenic infections. In 2001 Parker, [15] present a study with 373 patients, the mandibular first permanent molar was the most offending tooth at 33.2% followed by mandibular third molars (10%), mandibular permanent second molars (9.1%), mandibular second deciduous molars (7.2%), maxillary first permanent molars (5%) mandibular first deciduous molars (13 cases: 3.5%), maxillary deciduous first molar (2.4%) and maxillary second molar (2.4%).
In comparison with our study we have the mandibular third molar was the most offending tooth 45.20%, in second place was mandibular first molar (Table 3). In contrast, other studies have found the lower molars to be the most frequent causal teeth [16-20].
This predominance of lower molars in maxillofacial infections has been explained by deficient oral hygiene and the technical difficulty of restorative treatments in these posterior locations [21,22].
Peters, et al. [23] described the underlying medical condition and location of the infection to be the best predictors of length of hospital stay. In our study we have found length of hospital stay as an indicator of severity of infection was related to following factors: Socioeconomic status, blood sugar level, haemoglobin level, and oral hygiene and WBC counts.
During hospital admission, (Table 4) all the patients were treated with intravenous antibiotics, and the majority also received surgery under local anesthesia 97%. This surgery usually consisted of extraction of the causal tooth, abscess drainage with a active latex drain. According to the literature, surgical drainage is needed in 10-83% of all cases [5,15,24-26].
Table 4: Distribution of symptom in admission of the patients. View Table 4
Our study also showed that infections involving one anatomic space (submandibular space) were more common (54.63%) (Table 5) Parker, et al. [15]. Reported that the submandibular space was the most often affected in cases of facial infection.
Table 5: Distribution of localization of Odontogenic infections. View Table 5
The administration of Penicillins (penicillin, ampicillin and amoxicillin) is considered to be useful for the empirical management of odontogenic infections, as described by other studies published in Spain and particularly in other countries [1,4,12-14,17,19]. The advantages of such treatment are based on its appropriate spectrum, few side effects and low cost. However, some studies have alerted to an increase in the incidence of beta-lactam resistant organisms, particularly beta-lactamase producing anaerobes and viridans streptococci, which are frequently found in odontogenic infections [1,7,15,16]. In this study, penicillin and ampicillin resistance was found in 9.5% of the samples.
There are many complications subsequent to odontogenic infections as reported in the literature. Notable squeal are septicemia with disseminated intravascular coagulation, mediastinitis, thoracic emphysema, cardiac tamponade, and death [27-30].
Maxillofacial infections present a significant public health problem and one of the main reasons for consultations of the maxillofacial emergency service.
In our study, is shown that one the most effective treatment with incision, drainage and removal of etiology.
The obtaining of cultures and sensivity reports does not appear clinically helpful, and don't modificated the management in the majority of the cases. It is also very important to give attention to the high risk groups like diabetics, old age, patients with systemic diseases and pregnant women. All patients should be started with empirical intravenous antibiotics therapy which should be later on changed as per culture and sensivity report.
A multicenter prospective study with follow up data would be desirable to compare the different treatment options.
None declared.
None.
The authors declare that procedures conformed to the ethical standards of the responsible committee on human experimentation and in accordance with the World Medical Association Declaration of Helsinki.
The authors declare that they have followed the protocols of their workplace on the publication of data from patients and that all patients included in the study have received sufficient information and have given their written informed consent to participate in the study.
The authors have obtained the informed consent of patients and/or subjects referred to in the article. This document is in the possession of the author of correspondence.
None.