Treatment of cystic lesions includes multiple options, ranging from resection, decompression or marsupialization to enucleation. Different techniques for enucleation have been reported for head and neck cysts. This paper describes Shira's technique, using alginate as a filling material inside the cystic cavity, allowing demarcating the limits of the cystic lesions, maintaining their integrity. The use of alginate is recommended for the enucleation of cervicofacial cysts at the time of surgical excision because provide shorter operating time, also is an effective, safe and economical method. The authors will explain proper surgical exposure and operative procedure.
Alginate, Cysts, Enucleation
Cysts are defined as a pocket of connective-epithelial tissue, lined internally by epithelium and covered on its outer surface by connective tissue, enclosing liquid or semi-fluid content. The origin of these lesions in the head and neck can be congenital, inflammatory and neoplastic [1,2]. Rarely, they spontaneously involute and often increase rapidly and may be associated with secondary infection or trauma; becoming symptomatic, acquiring large size and even externalized [3,4]. There are alternatives for the treatment of these lesions that include surgical removal going from decompression, marsupialization, laser excision, intralesional injection and enucleation [5].
Currently, different techniques for enucleation have been described for head and neck cysts, such as hydro-dissection, sclerotherapy and alginate instillation described by Shira (1962), using it as a filling material inside the cystic cavity, delimiting the margins and maintaining the integrity of the lesion [5-8]. Considering the biomechanical properties of this material to improve visual access to the cyst, its properties such as malleability, setting time, low immunogenicity, biocompatibility, elasticity and its antimicrobial action improve the safety of this technique [9,10]. The aim of this study is to describe the enucleation of cervicofacial cysts using the Shira's Technique.
A series of 3 patients who attended the Oral and Maxillofacial Surgery Unit of the University Hospital of Maracaibo, Venezuela, from January 2014 to September 2016, with differential diagnosis of cervicofacial cysts. All the patients had no relevant medical records and were treated by the alginate instillation technique (Shira's technique) (Table 1).
Table 1: Distribution of the cases treated with the Alginate instillation technique according to age, gender, diagnosis, etiology, location and approach. View Table 1
As unit protocol and within the framework of congenital lesions of the midline, complementary studies such as echo Doppler, neck ultrasound and CT scans were requested, where vascular malformations and the presence of thyroid gland involvement were ruled out.
This study was approved by the University Hospital of Maracaibo IRB and all the patients and/or legal representatives signed an informed consent agreement.
All patients were treated in the operating room under balanced general anesthesia. After an adequate infiltration of lidocaine with 1:100.000 epinephrine, the incision of the superficial plane was made, minimizing bleeding and performing hydro dissection in the superficial planes of the surgical bed, the dissection was continued until the cystic lesion was meticulously exposed. Subsequently, a fine needle aspiration of the cystic content was performed and, with the needle in place, a syringe containing a mixture of low-density alginate was inserted and injected into the lumen of the lesion in proportion 1:1 to the aspirated liquid, replacing the liquid content with the irreversible hydrocolloid (Figure 1 and Figure 2) Once the material is gelled, it occludes the light of the cyst closing the minimum incision with it. The enucleation of the lesion was performed resecting it in its entirety and in a single piece by blunt dissection, without damaging adjacent structures, performing hemostasis and primary closure by planes (Figure 3). The specimen obtained in one single piece and aspirated liquids were sent to histopathological and cytopathological study respectively (Figure 4).
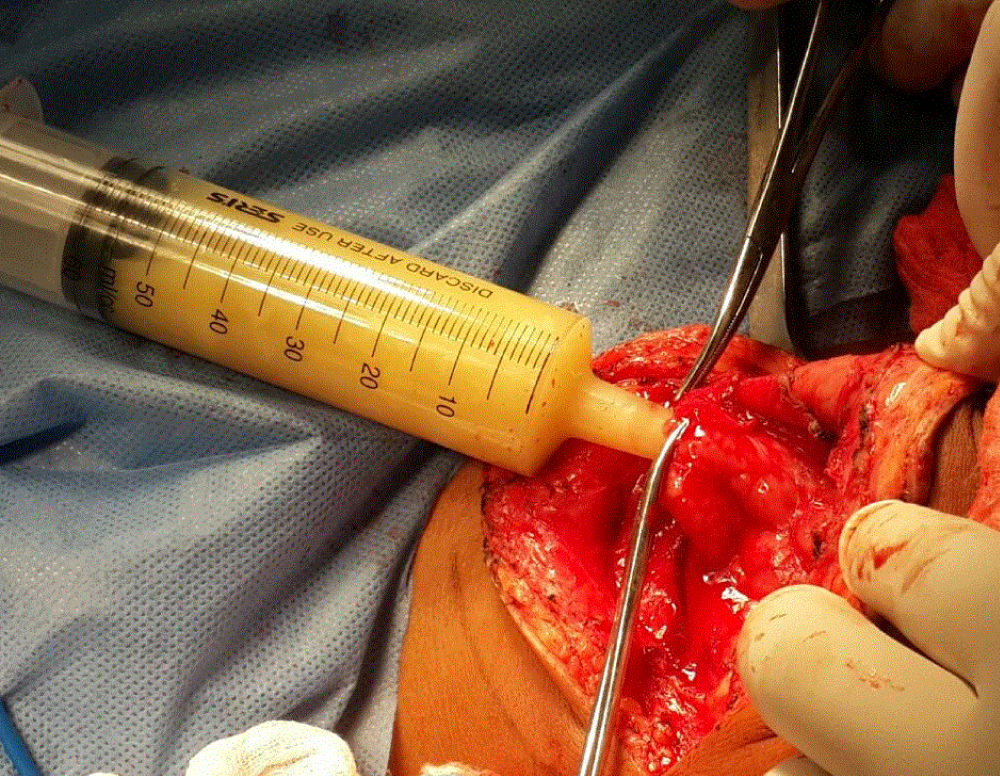 Figure 1: Aspiration of the cyst content.
View Figure 1
Figure 1: Aspiration of the cyst content.
View Figure 1
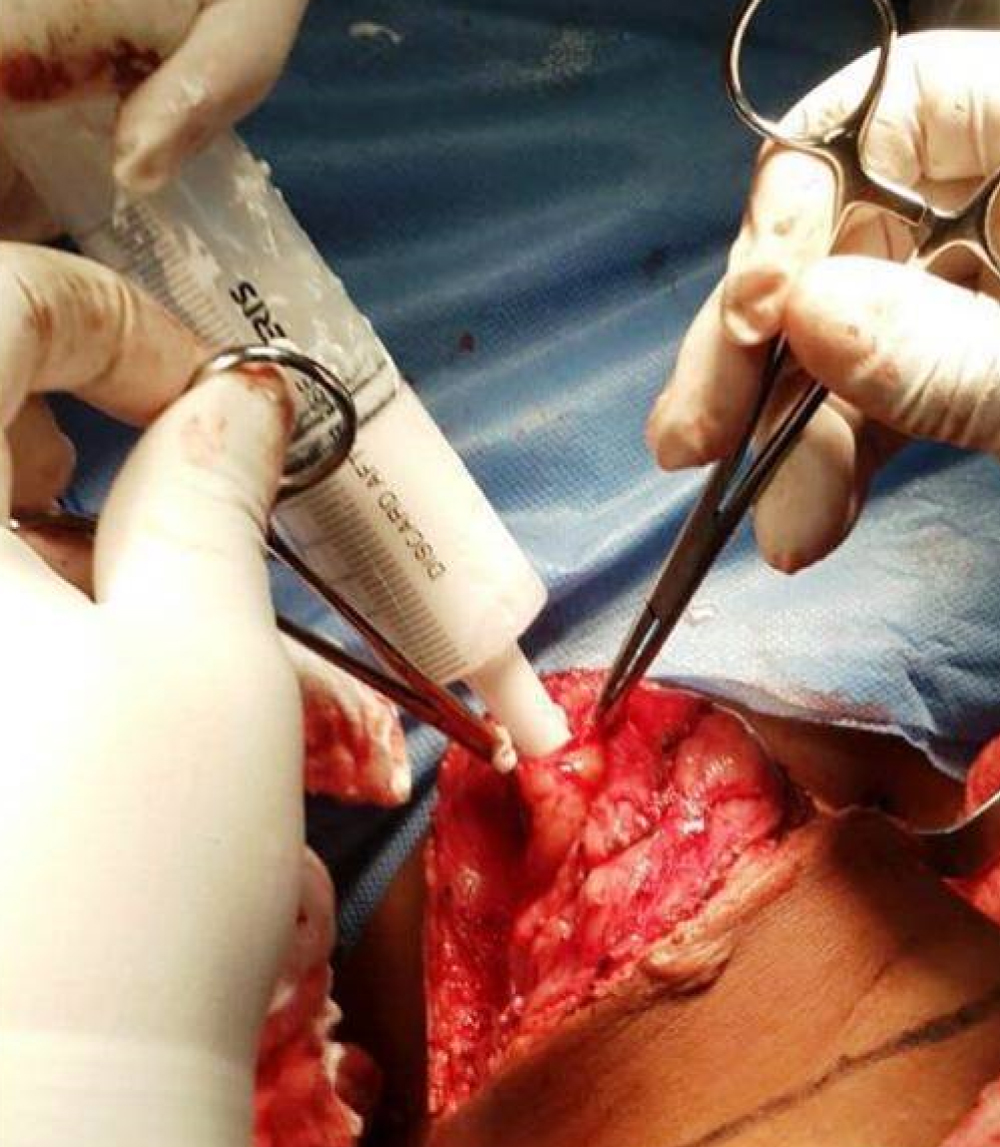 Figure 2: The alginate instillation technique.
View Figure 2
Figure 2: The alginate instillation technique.
View Figure 2
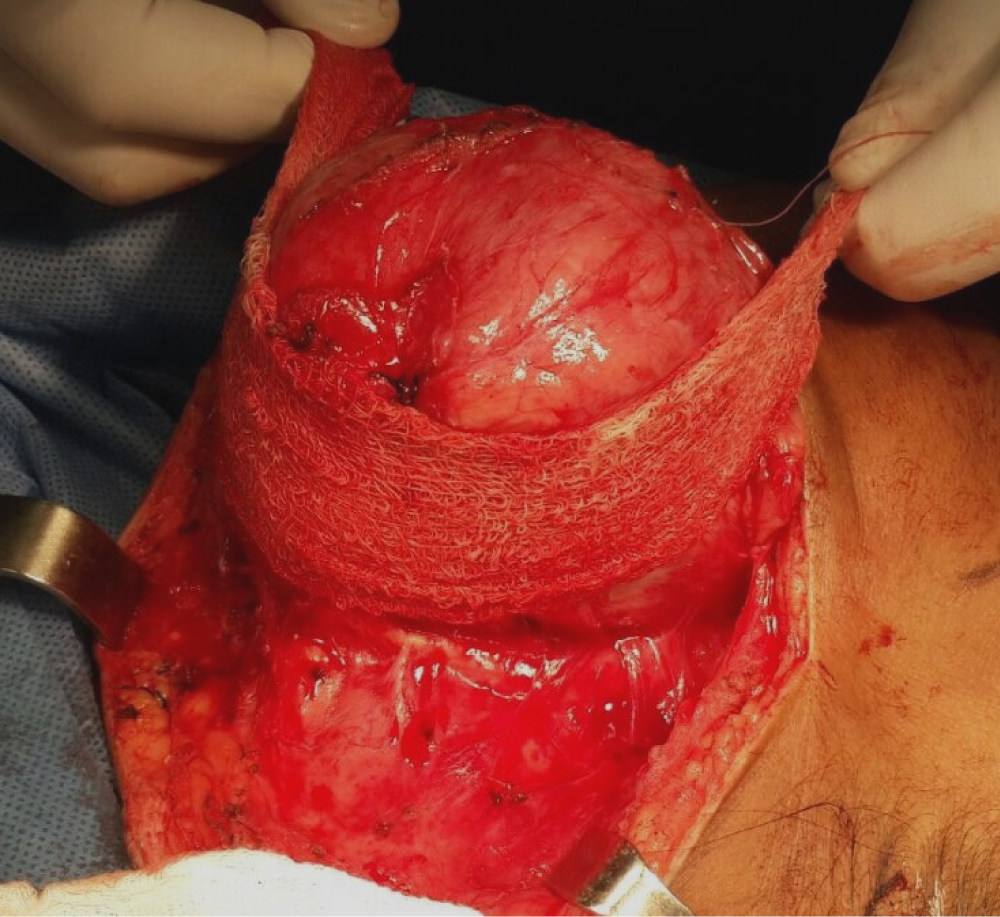 Figure 3: Enucleation of the cystic lesion.
View Figure 3
Figure 3: Enucleation of the cystic lesion.
View Figure 3
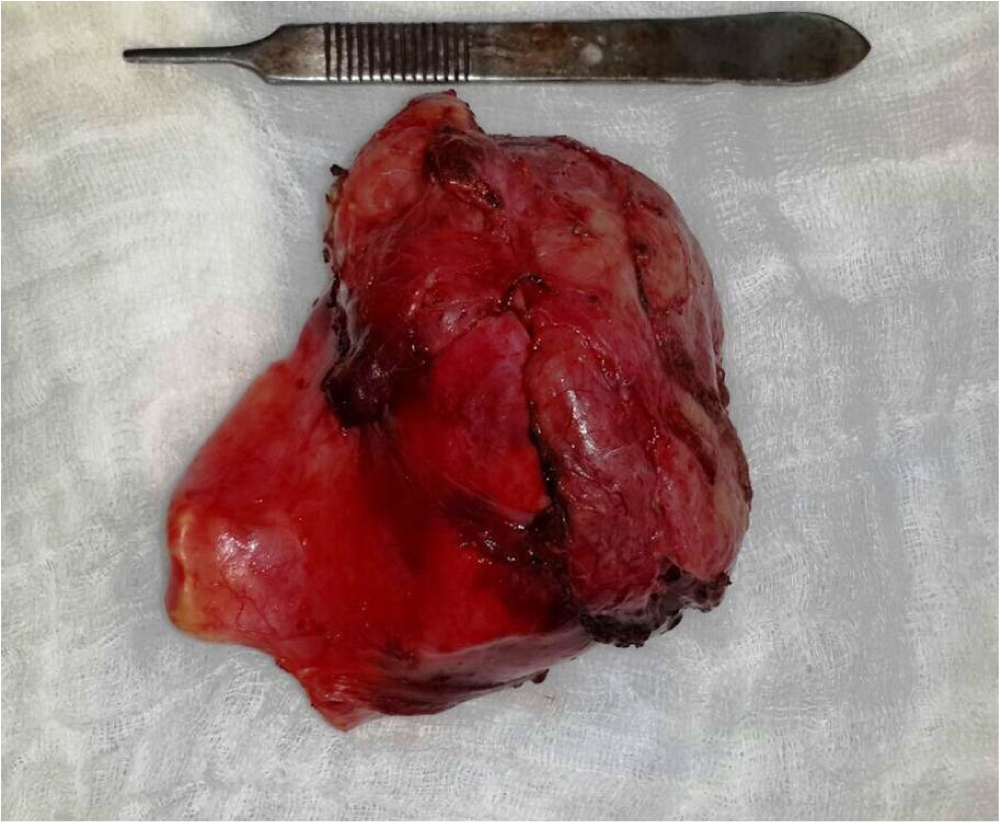 Figure 4: The sample obtained in a single piece.
View Figure 4
Figure 4: The sample obtained in a single piece.
View Figure 4
Alginate is a natural hydrocolloid used as dental impression material introduced in 1940. Since then, it is called an elastic printing material widely studied for its little allergenic property, good biocompatibility and biodegradability [11]. It presents viscous dissipative, plastic and elastic behaviors in different degrees depending on its composition, without deforming [12]. Its characteristics such as tractability, time of elasticity and faster setting at room temperature should be taken into account [9]. It should be addressed that one of the inherent properties of the alginate is the presence of antimicrobial action, which enhances the safety of this technique [13]. These characteristics allow the technique to be carried out, with only a portion of alginate; in addition for being an inexpensive (approximately 2.59 US$ for a 60cc siringe with 0.13 lb of alginate, considering the cost of 17 US$ for 1lb) and easily accesible dental material.
Shira (1962), proposed the treatment of mucoceles and ranulas by aspiration of the fluid content of the lesion, followed by the injection of alginate, allowing to delimit the margins of the injury and maintain its integrity. Therefore, surgical removal can be done quickly without the participation of adjacent structures [8]. In large lesions this technique is practical, safe and easy, avoiding recurrence and damage to vessels and/or major nerves; the filling of the cystic cavity with alginate improves visual access for surgical removal.
Several authors have reported the use of the technique of alginate instillation in cystic lesions in the head and neck: Shira (1962) [8], Santana, et al. [12], reported the technique in the treatment of mucoceles and ranulas; Katsuno, et al. [9], described the use of alginate instillation in the treatment of lymphangiomas, without reporting any incidents or signs of recurrence during the study period. We reviewed the literature on all the cysts treated using this technique (Table 2).
Table 2: Characteristics of included studies. View Table 2
This method can be used for the dissection of any cystic lesion with a collapsible lining. This technique is performed before excising the cystic lesion, in which the impression material of very low viscosity is allowed to set after being slowly injected into the lesion, therefore acting as a reliable guide to demarcate the exact boundaries of the same, decreasing intraoperative surgical time [17].
In the present study, the technique described by Shira was used, in two cases midline lesions of congenital origin and one in the submandibular region of traumatic origin; coinciding with that reported in the literature with the phenomena of mucosal extravasation in the sublingual region. However, only two cases of a cystic lesion of congenital origin have been reported [7,9], recommending complete surgical excision using the aforementioned technique, allowing easier recognition of the cystic capsule from the surrounding tissues. All these diagnoses were confirmed through histopathological study. It is noteworthy that the use of the impression material did not cause histopathological changes, in all 3 cases the classic characteristics of the lesions were evident. Similarly, Shira's proposal to inject irreversible impression material into the lesion represents an attempt to overcome difficulties inherent to the injury. The purpose of the procedure is to delineate the affected area clearly from the surrounding normal tissue. It also tends to stabilize the soft tissues, making dissection easier [14].
Due to the fact that this technique has almost not been reported in the literature, there is no evidence that supports that it reduces the risk of complications. However, in our experience we can confirm that it provides making dissection easier, thus, avoiding damage to adjacent structures as well as reducing the risk of recurrences. Compared to other techniques, the one hereby exposed is associated with less bleeding, fewer incidents of damage to soft and neural tissues and a much shorter operating time. Only two complications have been reported in the literature: foreign body reaction and local infection, especially when any residue of the hydrocolloid material is left in the operative field [14,17].
In our study, although it is a limited sample, we did not have any of these complications in the trans-operative or postoperative period, achieving normal healing and satisfactory results. Likewise, there were no recurrences during the follow-up period of forty-eigth months.
Shira's technique allows to clearly demarcate the limits of the cystic lesion, which is of utmost importance to achieve its complete extirpation, simplifying the recognition of the cystic capsule from the surrounding tissues and making dissection easier, thus, avoiding damage to adjacent structures and reducing the risk of recurrences of this type of pathologies as well as decreasing intraoperative time and inherent intraoperative complications, so this procedure should be considered a cost-effective approach. Despite this, given the low frequency described in the literature and several limitations of this study, further clinical studies are required to assess advantages and/or restrictions of this technique.
The authors declare that they have no conflicts of interest.