The aim of this paper is to draw up-to-date conclusions regarding small cell neuroendocrine carcinoma (SCC) of the parotid gland reviewing the largest case series from the literature and presenting them in a chronicle type manner. In addition, the first Greek case of SCC of the parotid gland with a favorable outcome is being reported.
A case occurred in a 76-year-old male patient is presented here. A partial parotidectomy and a selective neck dissection were performed. Post-operatively he underwent radiotherapy. A clinical and radiological follow-up examination disclosed no complication or recurrence until now, 5 years after surgery. The immunohistochemical study demonstrated that the tumor cells were positive for cytokeratin 20 (CK 20) among others neuroendocrine markers.
SCC of the parotid gland is a rare and very aggressive malignancy with histologic and immunostaining overlap with others SCCs. Clinicopathologic and demographic characteristics of this entity are very well defined. Prognosis remain very poor. Prognosticators that have been proved to reduce overall survival are tumor size and older age. Prospective studies are needed to establish better treatment modalities. Until then, treatment plan should be aggressive and encompass extended excision with neck dissection and adjuvant radiotherapy or chemoradiotherapy.
Neuroendocrine carcinoma, Small cell neuroendocrine carcinoma, Parotid gland, Salivary small cell neuroendocrine carcinoma
Small cell carcinomas (SCC) belong in the neuroendocrine neoplasms (NENs), being the most aggressive type of them, generally named neuroendocrine carcinomas (NECs) [1]. NENs are neoplasms that arise from cells derived from the neural crest with neuroendocrine differentiation [1]. SCCs usually arise in the lungs but 2-4% are extrapulmonary cases [1]. In the salivary glands they are extremely rare consisting < 1% of major salivary glands malignancies and 1% of primary parotid malignancies [2]. Due to this rarity, extended research has not been conducted yet to facilitate treatment guidance and our knowledge is based on case reports and case series [3].
As an exceedingly rare entity in the Head and Neck region, a complete work-up is mandatory in order to define whether this is a primary or a metastatic case [4]. The definitive diagnosis relies on histopathology and immunohistochemistry, and currently, the treatment regimen is not definite and includes surgery, radiotherapy and chemotherapy, or a combination of these methods [5].
The aim of this paper is to draw up-to-date conclusions regarding small cell neuroendocrine carcinoma (SCC) of the parotid gland reviewing the largest case series from the literature and presenting them in a chronicle type manner. In addition, the first Greek case of SCC of the parotid gland with a favorable outcome is being reported.
A 76-year-old male patient was referred to our Department of Oral and Maxillofacial Surgery on August 2015, with a painless, rapidly growing mass of the left parotid gland, appeared before 4 months. His medical conditions were noncontributory and regulated by drugs. No smoking history was reported.
On presentation, his chief complaint was that the last 2 months, after fine needle aspiration (FNA) was performed, the mass was growing even faster and the overlying skin had been ulcerated (Figure 1). The FNA report was inconclusive, showing greater probability of lymphoma, however further investigation was essential. The lesion was biopsied under local anesthesia and the histopathology report revealed a neuroendocrine carcinoma of the parotid gland with elements of both small and medium-sized cells.
 Figure 1: Preoperative image of the lesion with the ulceration of the overlying skin (yellow arrow).
View Figure 1
Figure 1: Preoperative image of the lesion with the ulceration of the overlying skin (yellow arrow).
View Figure 1
Clinical examination revealed a scleroelastic, firm, painless mass in the left inferior aspect of the parotid gland with ulceration of the overlying skin. Palpation of the neck did not reveal any signs of swollen nodes. Furthermore, other symptoms referring to the patient's general condition (paraneoplastic symptoms) were not mentioned. In the radiological examination with Computed Tomography (CT) scan, a mass of soft tissues was described in the left parotid tail measuring 2.5 × 1.9 cm with no skin involvement. After Intravenous contrast administration the mass was heterogeneously enhanced suggesting areas of central necrosis (Figure 2).
 Figure 2: CT scan preoperatively before skin ulceration (A) Before (white arrow) and; (B) after (yellow arrow) intravenous contrast administration.
View Figure 2
Figure 2: CT scan preoperatively before skin ulceration (A) Before (white arrow) and; (B) after (yellow arrow) intravenous contrast administration.
View Figure 2
In order to exclude a metastatic lesion in the parotid gland the patient underwent a thorough whole-body CT scan including brain, chest and abdomen and a positron emission tomography and computed tomography (PET-CT), where no signs of malignancy or suspicious lesions were present. Hence, the final diagnosis was primary small cell neuroendocrine carcinoma of the parotid gland and an operation was scheduled.
He was admitted to our department and a partial parotidectomy with excision of the overlying skin was performed. The facial nerve was preserved and before the excision a selective neck dissection was performed (Ia, Ib, IIa, III, Va). Grossly, the tumor was a grey pinkish approximately 2.7 cm in greater dimension.
The histopathology report revealed the presence of a malignant small cell carcinoma. The cells of the tumor were compactly arranged, forming sheets of uniform small cells with rounded nuclei containing evenly dispersed chromatin. Nucleoli were inconspicuous. Mitotic figures were frequent and fragmental necrosis was visible (Figure 3). Sections from the overlying skin revealed that it was free from malignant cells.
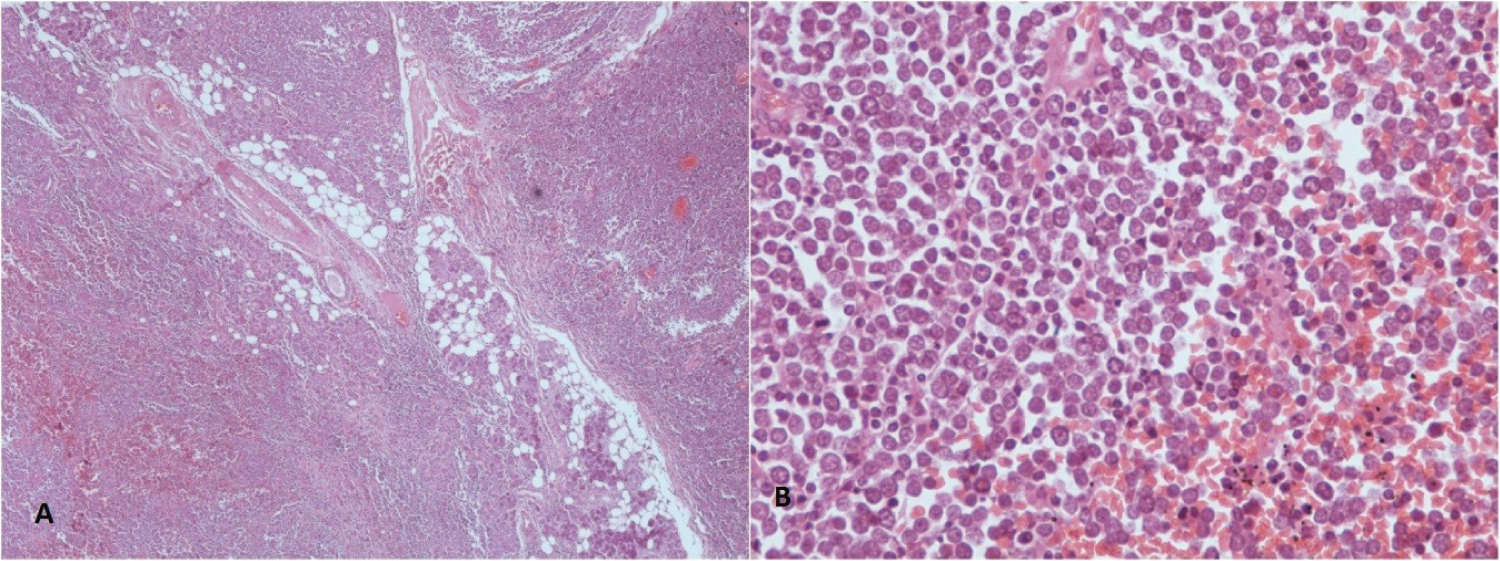 Figure 3: (A) Salivary gland lobules are largely replaced by irregular solid sheets of small densely basophilic tumor cells (H+E stains x200); (B) high magnification of the tumor cells shows ill-defined cytoplasmic borders, round nuclei with dispersed chromatin and rare small nucleoli. Mitoses are numerous (H+E stains x400).
View Figure 3
Figure 3: (A) Salivary gland lobules are largely replaced by irregular solid sheets of small densely basophilic tumor cells (H+E stains x200); (B) high magnification of the tumor cells shows ill-defined cytoplasmic borders, round nuclei with dispersed chromatin and rare small nucleoli. Mitoses are numerous (H+E stains x400).
View Figure 3
The immunohistochemical study demonstrated that the tumor cells were positive for cytokeratin 20 (CK 20) (paranuclear dot-like pattern), epithelial membrane antigen (EMA), synaptophysin (SYN), CD 56, chromogranin and NSE (neuron specific enolase). On the other hand, cells were negative for S-100, TTF-1 and CD 117.
Additionally, the proliferation index as calculated by Ki67 index was very high 70-75% (Figure 4). The histopathological report coincided with the previous one. In addition, the surgical margins were free of malignant cells and all 18 nodes were free of metastasis.
 Figure 4: (a) Cytokeratin 20 immunoreactivity. The punctate perinuclear globular staining results in the characteristic dot-like pattern; (b) Chromogranine A positive; (c) CD56 positive; (d) The proliferation index as evaluated by Ki67 index is very high.
View Figure 4
Figure 4: (a) Cytokeratin 20 immunoreactivity. The punctate perinuclear globular staining results in the characteristic dot-like pattern; (b) Chromogranine A positive; (c) CD56 positive; (d) The proliferation index as evaluated by Ki67 index is very high.
View Figure 4
The patient made an uneventful postoperative recovery and was discharged a week later. The tumor board's decision was postoperative radiotherapy, Due to the absence of adverse signs in the histopathology report and due to tumors size, that was 2.7 cm, chemotherapy was not decided at that time. Six weeks later he underwent radiotherapy receiving 6600 cGy on the parotid region and on the left neck. A clinical and radiological follow-up examination disclosed no complication or recurrence almost 5 years after treatment.
The first case of SCC of the head and neck was reported by Olofsson and Van Nostrand in 1972, and was found in the larynx [5]. SCC was once considered to be a type of undifferentiated carcinoma, so the first reports of undifferentiated carcinomas of the salivary glands that basically were SCC appeared in 1972 as well, where Koss, et al. presented a case series of 14 oat cell-like SCCs of the minor salivary glands [6]. The first case report of SCC of the parotid gland is being reported in 1976 by Wirman, et al. where they describe a tumor from the parotid gland that fits Koss's histopathological description [7].
Later in 2004 Nagao, et al. reported that until then only 60 cases of SCC in the parotid gland had been published [8]. He also added a case series of 15 patients with SCC of major salivary glands - 13 patients with SCC of the parotid and 2 patients with SCC of the submandibular gland searching in Mayo Clinic files from 1930-2002 [8].
In 2013, Servato, et al. published a systematic review of the literature gathering 130 cases before implementing exclusion criteria. 17 referred to SCC of minor salivary glands and excluded. From the remaining 113 patients with major salivary gland SCC, he included 44 and concluded that this entity has well defined demographic and clinicopathologic characteristics. However, it has not been possible to establish treatment recommendations with such a low number of cases [9].
The overwhelming majority of salivary NECs are high grade with the small cell type outnumbering large cell by 5:1. Well and moderately - differentiated are < 10 cases described in the literature [10].
The largest research conducted so far, as far as the patients' number is concerned comes from Zhan, et al. in 2016, where they searched the US Cancer Database from 1998 to 2012 and identified 344 patients with SCC of the parotid gland. They found that SCC represents 1.11% of all parotid malignancies and the average age of presentation is 73 years. Typically, this tumor present as a painless, progressively enlarging mass of 3 to 6 months duration [2]. Cervical lymphadenopathy and facial nerve palsy are common findings. Paraneoplastic syndromes accompanied by the production of ectopic hormones are unusual [11]. However, a case is reported where a 24-year-old female patient with SCC of the palate, developed Cushing syndrome after the disease had metastasized into the liver [12]. Nearly all patients affected are Caucasians and male to female ratio is 4:1. The incidence of regional lymph node metastasis is around 50.8% and adding the occult lymph node metastasis sums up at 65.1%. This is the reason why neck dissection is necessary in the treatment of SCCs [2]. All of these demographics are in accordance with previous case series [8,9]. What is not in accordance is the distant metastasis rate, where Zhan, et al. state distant metastases to be found in 7.3% of all cases. This is explained because it refers in the initial staging of patients [2]. During the course of the disease this figure climbs up to 45% [8,9,11]. Zhan, et al. report that five and 10-year survival rate is 37% and 20% respectively, and median survival is 28.5 months [2], Servato, et al. similarly reports 5-year OS at 36.6% [9], whereas Nagao, et al. found 5 year OS to be worse at 13% and median survival 15.9 months [8].
The latest case series published from Bai, et al. on December 2019, searching SEER Database between 1988 and 2016 and identifying 198 patients with SCC of the salivary gland. 167 were located in the parotid gland, 25 cases were observed in the submandibular gland and 6 in the minor salivary gland. The median overall survival was 25 months and the five and ten-year survival rate was 33% and 22.7% respectively [1].
As an exceedingly rare entity, SCCs of the head and neck region represent a diagnostic and therapeutic challenge in the routine practice. The suspicion of a malignancy in the parotid gland, beyond clinical examination, is raised by imaging modalities like CT and MRI scan [9]. Lesion with irregular and nonspecific borders, lobular contours, heterogenous enhancement after intravenous contrast administration, erosion of adjacent structures and lymph node involvement are characteristics of a malignant lesion [9,13]. It is agreed that there are no distinctive CT or MR imaging characteristics in SCCs [13]. The diagnosis is based on histological, ultrastructural and immunohistochemical criteria, which may be misdiagnosed in small biopsy samples. For that reason, a large core needle biopsy, rather than an FNA is preferred for diagnosis [4]. A complete work- up is necessary to rule out a metastatic origin of the tumor, since SCCs are much more common in other parts of the body [4]. To this direction radiologic imaging with CT, PET/CT and octreoscan are basic [4]. Chernock, et al. reports the difficulties to distinguish primary salivary SCCs from metastases to the salivary glands because morphologic and immunostaining features between cutaneous and salivary NECS may be indistinguishable [10].
Under the microscope, small cell carcinoma is characterized by sheets, cords, or irregular nests of anaplastic cells and a variable amount of fibrous stroma. The cells are 2-3 times larger than the mature small lymphocytes and are round or oval in shape [5,11].
The tumor cell nests immunoreactivity for a) Cytokeratins (CK), which often have a characteristic paranuclear dotlike pattern of reactivity; b) Epithelial membrane antigen (EMA); c) Cluster of differentiation (CD)117; d) Synaptophysin (SYN, neuron-specific enolase) and e) Thyroid transcription factor (TTF)-1. These are all known as neuroendocrine cell markers. A diagnosis of SCC can be determined if a tumor is positive for at least one of these markers [5]. SYN is a specific marker of nerve and epithelial tumors and is often used as a marker for neuroendocrine tumors. TTF-1 is frequently expressed in the epithelial cells of the thyroid glands and lungs [5]. Others report that TTF-1 is expressed in almost all pulmonary SCCs and in slightly less than 50% of extrapulmonary SCCs and is negative in Merkel cell carcinoma [4]. CD-117 is predominantly expressed in gastrointestinal stromal tumors, but may also be expressed in SCC of the lung [5]. In our case, tumor cells were positive for cytokeratin 20 (CK 20) (paranuclear dot-like pattern), epithelial membrane antigen (EMA), synaptophysin (SYN), CD 56, chromogranin and NSE (neuron specific enolase). On the other hand, cells were negative for S-100, TTF-1 and CD 117.
Regarding CK20 Chan, et al. have proposed that the neuroendocrine type of SCC can be subdivided into Merkel cell and pulmonary varieties on the basis of CK20 immunoreactivity. According to their classification, the Merkel cell variety expresses CK20 and the pulmonary variety does not. In detail they conclude that three out of four salivary small cell carcinomas are cytokeratin 20 positive [14]. Positive immunoreactivity for CK20 and neurofilament with a dot like pattern, like our case, strongly favors salivary SCC or Merkel cell carcinoma, features that are not detected in pulmonary SCC, which is the most likely metastatic neoplasm [8]. Consequently, the neuroendocrine type of SCC may be further subclassified into Merkel cell and pulmonary varieties on the basis of cytokeratin (CK) 20 immunoreactivity [8,10].
As far as prognosticators are concerned age, tumor size and distant metastasis are significant and independent predictors of worse survival [2]. Previously Nagao, et al. were the first to report that tumor size > 3 cm, negative immunostaining reaction for cytokeratin 20 and decreased immunoreactivity for neuroendocrine markers reduced overall survival [8]. Servato, et al. confirmed tumor size to be a significant negative prognosticator but failed to prove CK20 or number of neuroendocrine markers to be significant. They were the first to report that patients age is a prognostic factor [9]. Bai, et al. concluded that age, tumor size regional and distant metastases and marital status as well had significant association with survival [1].
Regarding treatment of primary SCC of major salivary glands, data lack sufficient detail to make survival comparisons between modalities yet. Currently most cases are treated by extended total parotidectomy, extended neck dissection and adjuvant radiotherapy, chemoradiotherapy or both [1,2,4,5,9,15]. If the tumor is unresectable or if regional recurrences or distant metastases are present then chemotherapy or chemoradiation is used [2,15]. For SCC head and neck tumors, chemotherapy with a small-cell lung cancer regimen such as cisplatin or carboplatin with etoposide is used [15]. New chemotherapeutics agents, such as taxanes, campothecin derivatives (topotecan, irinotecan) and gemicitabine, as single agents, or in combination, have shown activity against SCC [4]. While PD- L1 inhibitors have shown disease response in Merkel cell carcinomas, their efficacy in salivary SCC is unknown [10].
The incidence of regional lymph node metastasis plus occult metastatic lymph nodes dictate the need for neck dissection in every SCC case [2]. From the 18 out of 44 patients of Servato's case series that are alive without evidence of disease 8 followed that treatment modality [9]. Bai, et al. stated that the combination of radiotherapy with surgery could significantly improve patients' prognosis compared with those with surgery alone (45.0 months vs. 18.0 months: P < 0.01) [1]. They also stated that radiotherapy was an independent factor for favorable survival and this decreased the risk of death by 44% [1]. Experience from gastrointestinal NETs shows that expression of somtostatin receptors through a high uptake of octreotide in scintigraphy could be useful to select tumors that could benefit from the systemic use of somatostatin analogues [4].
The current pathologic classification of neuroendocrine neoplasms (NENs) across different organ systems use a range of site-specific terminologies and criteria, creating significant confusion among pathologists and clinicians [16].
Table 1 shows the terminology used for different site in the Head and Neck region comparing 2005 and 2017 edition [11,16].
Table 1: Comparison of classification systems of Head and Neck NENs between WHO 2005 and WHO 2017 Blue Books. View Table 1
A dedicated consensus meeting was held in Lyon on November 2017, under the auspices of the WHO Classification of Tumors Group, where a 'common classification framework' was developed to standardize concepts among NENs of all different anatomic sites [17]. They agreed that the term NEC is clearly indicative of high-grade malignant histology and biologic behavior. NET, in contrast, is intended to designate well-differentiated neoplasms whose potential to invades and metastasize depends on tumor site and type. For NECs specifically, being the vast majority of this entity in major salivary glands, it was proposed and accepted that NECs are i) Of high grade by definition; ii) Of two separate morphologic types and iii) Defined as small cell neuroendocrine carcinoma (SCNEC) or large cell neuroendocrine carcinoma (LCNEC) [17].
It was also agreed that three grading parameters of prognostic relevance are: i) Mitoses per mm2 area, ideally counted in up to 10 mm2. In lung and pancreatic NENs, it is current practice to express the number of mitoses within an area of 2 mm2. It may also be best practice to specify the number of mitoses counted within the total area assessed for each case (i.e. X mitoses in Y mm2) ii) The Ki-67 cell labeling index performed on regions of most intense labeling and iii) The presence or absence of necrosis, defined by morphological criteria [17].
Finally, it was proposed and agreed that in the pathology report: i) The parameters used for grading be stated clearly; ii) The site-specific tumor nomenclature according to current WHO classification be stated first; and iii) The novel uniform standard classification terminology for NEN (NEN-WHO 2018) be added in brackets when it differs from the currently employed terminology [17].
To conclude salivary SCC is a rare and very aggressive malignancy with histologic and immunostaining overlap with more common pulmonary and cutaneous SCC. From the recently published case series, clinicopathologic and demographic features of this entity are very well defined. Prognosis remain very poor. Prognosticators that have been proved to reduce overall survival are tumor size and older age. Prospective studies are needed to establish better treatment modalities. Until then, treatment plan should be aggressive and encompass extended excision with neck dissection and adjuvant radiotherapy or chemoradiotherapy. Regarding terminology fundamentals have been built for a consented classification.
The authors state that there are no financial or other relationships which may lead to a conflict of interest, and no financial or material support in the submitted manuscript.
The authors state that they are all equally responsible for the content of the manuscript, have agreed to its publication and have given the corresponding author the authority to act on their behalf in all matters pertaining to publication.