In the last decade, the incidence of Human papilloma virus (HPV)-associated oropharyngeal cancer has increased and as high as 70% of all oropharyngeal cancers are caused by HPV. First line health professionals might feel uncomfortable discussing topics related to sexual habits. The objectives of this study are to assess the level of knowledge about HPV-associated oropharyngeal cancer amongst first line health professionals and to evaluate the impact of an educational intervention on communication with patients.
Basic levels of knowledge of HPV-associated oropharyngeal cancer and ease to deal with patient were evaluated for general practitioners (GP), head and neck specialists (HNS), and nurses. Each category of professional was divided into two groups: Participants who receive a single HPV training, and a control group. The training was a one-hour presentation addressing the management of HPV-associated oropharyngeal cancer. Participants filled questionnaires about general demographic information, general knowledge of oropharyngeal HPV, the ease to deal with HPV patients and evaluation of the educational intervention.
The sample consisted of 122 participants consisting of first line health professionals. All groups presented a significant increase of their knowledge following the training session. Post-training nurses out performed control GPs. Nurses with less than 10 years of practice presented higher scores than more experienced nurses. For all categories, the training resulted in a significant increase of their perceived ease to discuss head and neck HPV with patients.
Continuous education on HPV-oropharyngeal cancer is needed for health professionals and it improves immediate knowledge and ease of discussion.
Human papilloma virus, HPV, Oropharyngeal cancer, Counselling, Education
Human papilloma virus (HPV) is the most frequent sexually transmitted infection. The virus is highly prevalent in the general population. It is estimated that in the USA, respectively 84.6% and 91.3% of sexually active women and men will contract HPV at a point or another in their life [1]. The virus will be spontaneously eliminated within 2 years post-infection in 90% of the cases [2]. The HPV might get reactivated in some people, leading to the development of tumors typically taking place either in the anogenital region (cervix, vulva, penis, or anus) or in the oropharynx. Overall, the relationship between HPV and anogenital cancers is well known in the general and medical population, notably thanks to massive vaccination campaigns in most Western countries [3]. However, the incidence of HPV-associated oropharyngeal cancer exceeded that of HPV-associated cervical cancer in the last decade [4]. Nowadays, as high as 70% of oropharyngeal cancers are caused by HPV [5]. In contrast to what is seen for anogenital cancers, the general population is considerably less aware of the association between HPV and oropharyngeal cancer. Furthermore, this is true not only for the general population, but also amongst health professionals [6,7]. Indeed, a survey-based study performed at a middle-size US university demonstrated that only one third of first year medical students, and only 70% of fourth year medical students were aware of the link between HPV and oropharyngeal cancer [6]. Similarly, a recent Italian study showed that less than a fourth of nursing students were aware of this relationship [7].
When receiving an HPV-related cancer diagnosis, patients will come with numerous questions. In addition of coping with cancer and its consequences, patients must manage the emotional burden of being affected by a sexually transmitted infection [8]. Since HPV transmission occurs during oro-genital sexual intercourse, both patients and health professionals might feel uncomfortable discussing topics related to sexual habits. This is especially true for first line health professionals, for instance for general practitioners or when the initial reference is made to a head and neck specialist [8-10]. Obviously, the fact that health professionals might not be comfortable with the subject could represent a problem for patient counselling, and ultimately care in a context of patient empowerment. Thus, this study was designed to evaluate the current state of knowledge of first line health professionals on HPV-related oropharyngeal cancers. We then evaluated the potential of a single 1-hour training session to alleviate both potential lack of knowledge and unease to deal with the topic. Therefore, the first objective of this study was to assess the level of knowledge about HPV infection and cancer amongst general practitioners, nurses, and head and neck specialists. The second objective was to evaluate the feasibility and potential of an educational intervention directed at first line health professionals to improve communication with patients.
Basic levels of knowledge of HPV-associated oropharyngeal cancer and ease to deal with patients were evaluated for the 3 study populations: General practitioners (GP), head and neck specialists (HNS) and nurses. Each study population was divided into two groups, a group of participants who received the 1 hour HPV training and a group who did not receive the HPV training. Head and neck surgeons were defined as otorhinolaryngologist or maxillofacial surgeons. Nurses were coming from intensive care units, surgery floor, outpatient's clinics, or were oncology pivot nurses. Participants were recruited from the medical staffs of urban and rural public hospitals of the Quebec province (Canada). Participants were contacted using a snowball sampling approach. Data were collected from November 2018 to June 2019. Prior to beginning the study, the protocol was approved by the institutional ethics committee of the "CHU de Québec-Université Laval" (approval number: 4397).
In order to assess the effect of the exposition to HPV training on the knowledge of HPV induced oropharyngeal cancer, a specific educational intervention was developed. The selected format was a one-hour lecture-like presentation addressing seven aspects of management of HPV induced oropharyngeal cancer: Pathophysiology, transmission, prevention, vaccination, screening, treatment, and approach to the patient. The presentation was developed by an oncologic head and neck surgeon and a senior resident in otorhinolaryngology and head and neck surgery using the most recent evidence-based studies on HPV. Educational interventions were performed by the designers of the teaching material.
Three questionnaires were used in this study (Annexe 1). A first questionnaire combined general demographic information (gender (male, female, other, undisclosed), age (20-35 years, 36-50 years, 51-65 years, 66 years+), profession, field of practice, years of practice (0-5 years, 6-10 years, 11-15 years, 16 years+)) and an evaluation regarding the ease of the professional to deal with HPV patients. This second part of the first questionnaire was made of five 10-points Likert scale items. A second questionnaire was developed to evaluate the general knowledge of the participants of HPV-associated oropharyngeal cancer. This 10-items questionnaire contained Likert scale-based items. Participants of the 1-hour HPV training groups were tested immediately after the educational intervention. Long-term retention was not evaluated in the present study. Finally, a third questionnaire (which was only used for participants of the HPV training groups) was developed to evaluate the educational intervention itself. This 7-items questionnaire contained four Likert scale-based items (Table 1) (What is your global appreciation of the HPV training? Did the teachers seem competent to teach you? Was the subject taught interesting? Will this training change your practice?). Participants from the control groups completed electronic versions of the questionnaires. Participants of the HPV training groups completed a paper-version of the questionnaires.
Table 1: Evaluation of the HPV training on 10-points Likert scale items. View Table 1
Statistical analyses were performed using Mann-Whitney U-tests. When applicable, results are presented as mean ± SEM.
The final sample consisted of 122 participants consisting of medical staff from hospitals of the Quebec province (Canada). No questionnaires were excluded from the sample. All participants identified themselves to one gender. The sample consisted of 44 GPs (control group: 21 (6 males, 15 females), HPV training group: 23 (23 females)), 24 HNSs (control group: 14 (6 males, 8 females), HPV training group: 10 (6 males, 4 females)), and 54 nurses (control group: 24 (3 males, 21 females), HPV training group: 30 (30 females)). The repartitions of the participants for each of the subgroups depending on their age and number of years in practice are provided in Table 2. Our population consisted mainly of health care professionals working in a university hospital context (GP control group: 62%.; GP HPV training: 87%; HNS control group: 100%; HNS HPV training group: 80%; nurses control group: 79%; nurses HPV training group: 93%).
Table 2: Repartition of the participants depending on their age and numbers of years of practice of the participants. View Table 2
Responses evaluating the ease of health care professionals to discuss with patients about head and neck and non-head and neck forms of HPV-related tumors are summarized in Table 3. There is no difference between GPs and nurses regarding the ease of discussion of head and neck HPV infections with patients (p = 0.2 and p = 0.24 for control and HPV training groups, respectively). Head and neck surgeons were discussing significantly more frequently this topic with their patients when compared to the other 2 groups (p < 0.05 between HNS and GP control groups, p < 0.001 between HNS and nurse control groups, p < 0.001 between HNS and GP HPV training groups, and p < 0.001 between HNS and nurse HPV training groups).
Table 3: Responses evaluating the ease of health care professionals to discuss with patients about ORL and non-ORL forms of HPV-related tumors on a 10-Likert scale. View Table 3
A similar pattern was evidenced for the perceived ease to discuss head and neck HPV infections with patients. There were with no significant differences observed between GPs and nurses (p = 0.67 and p = 0.17 for control and HPV training groups, respectively). Both GPs and nurses were significantly less comfortable than HNSs when discussing head and neck HPV infections (p < 0.01 between HNS and GP control groups; p < 0.01 between HNS and nurse control groups; p < 0.01 between HNS and GP HPV training groups, and p = 0.052 between HNS and nurse HPV training groups).
General practitioners significantly discussed more frequently non head and neck HPV infection than both HNS and nurses (p < 0.05 between GP and HNS control group, p < 0.001 between GP and HNS HPV training group, p < 0.01 between GP and nurse control group, p < 0.001 between GP and nurse HPV training group). General practitioners were significantly more at ease to discuss non head and neck HPV infection than both HNS and nurses (p < 0.01 between GP and HNS control group, p < 0.001 between GP and HNS HPV training group, p < 0.05 between GP and nurse control group, p < 0.01 between GP and nurse HPV training). For all professional categories, the HPV training resulted in a significant increase of their perceived ease to discuss head and neck HPV infections with patients (p < 0.05 for GPs; p < 0.05 for HNSs; and p < 0.05 for nurses).
Initial scores were comparable for GP (score: 6.33 ± 0.32) and HNS (score: 6.79 ± 0.5, no significantly different, p = 0.19) but were significantly lower for nurses (4.42 ± 0.47, p ˂ 0.01 from GP, and p ˂ 0.01 from HNS, Figure 1). All groups presented a significant increase of the immediate knowledge score following the training session (GP, score: 8.57 ± 0.23, different from related control group at p ˂ 0.001; HNS, score: 8.3 ± 0.3, different from related control group p ˂ 0.05; nurses, score: 7.6 ± 0.25, different from at the related control group at p ˂ 0.001). Post-training nurses got significantly higher scores than untrained GPs (p ˂ 0.01). Despite the limited size of some of the age groups, a trend was observed between the initial and post-training scores of nurses as a function of their experience (Figure 2). Nurses with less than 10 years of practice presented higher knowledge scores than more experienced nurses. Furthermore, HPV training-related improvement of the knowledge score was less marked for nurses as working experience increased.
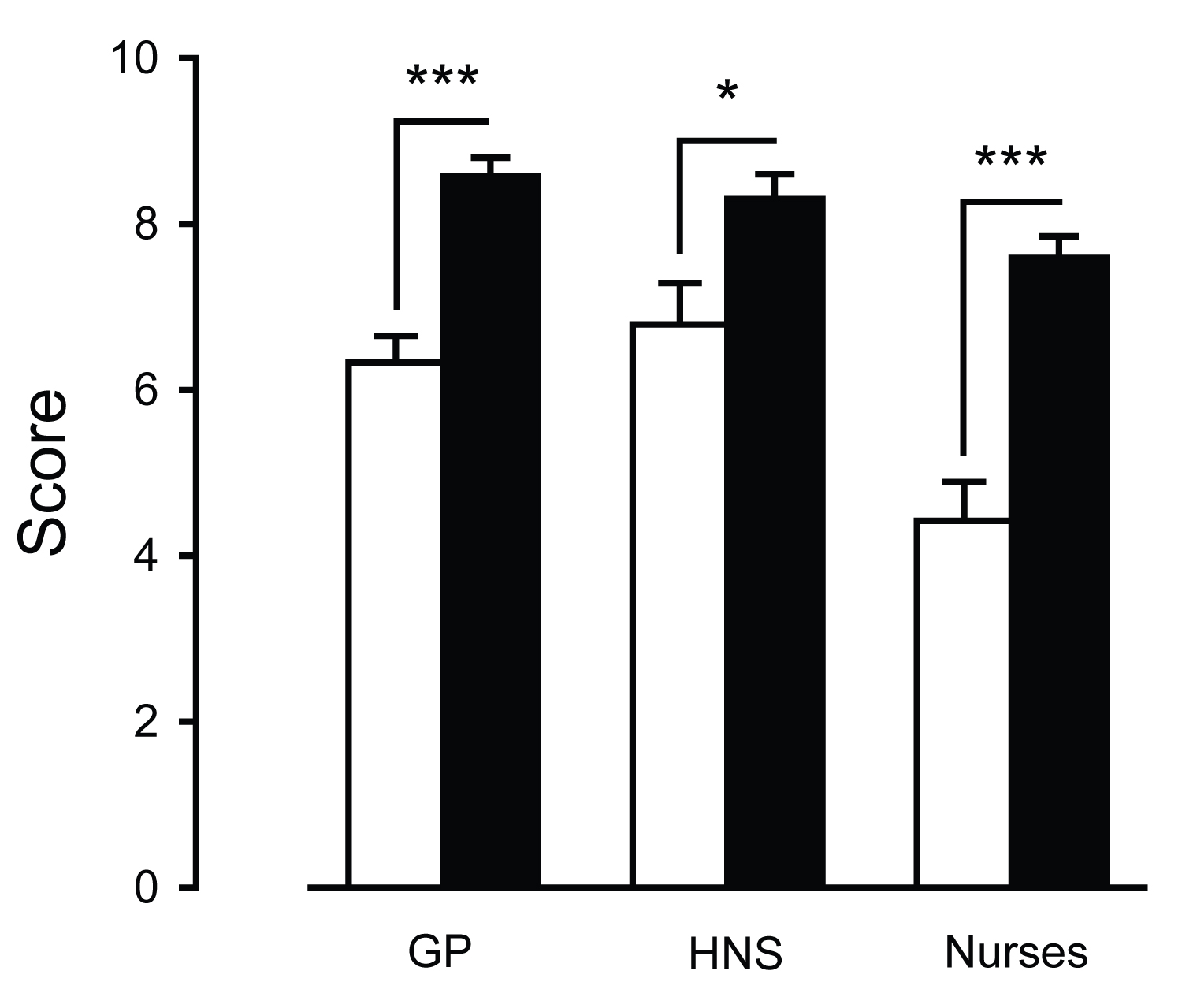 Figure 1: Control and post-training knowledge scores.
Figure 1: Control and post-training knowledge scores.
This figure presents the control (white) and post-training (black) scores on the oropharyngeal HPV cancer knowledge questionnaire (minimal score: 0, maximal score: 10), depending on the profession of the participants (GP: general practitioners, HNS: head and neck surgeons, nurses). Results were presented as mean ± SEM (*p ˂ 0.05, *** p ˂ 0.001).
GP: General practitioners, HNS: Head and neck specialists
View Figure 1
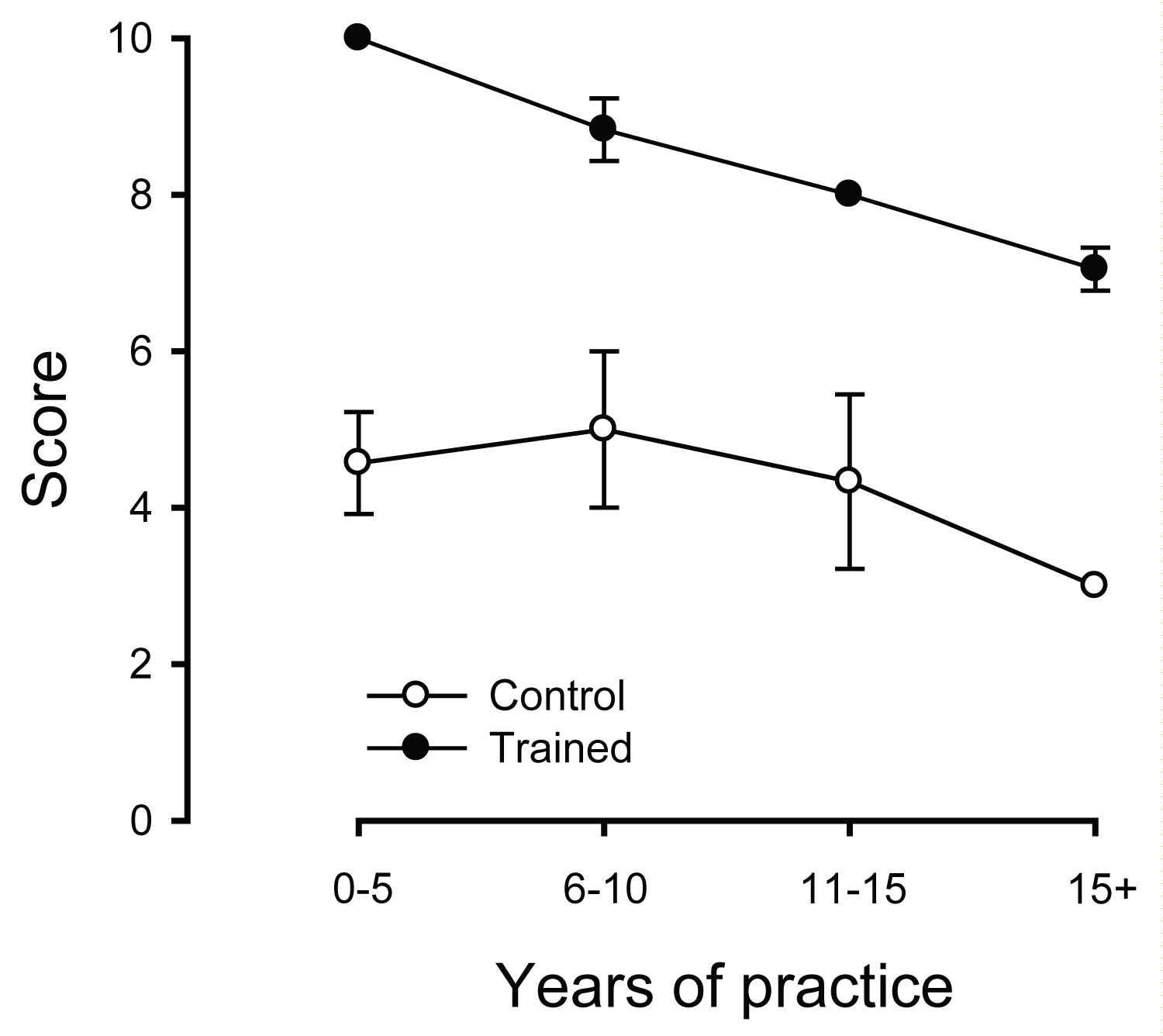 Figure 2: Knowledge score for nurses as a function of the years of practice.
Figure 2: Knowledge score for nurses as a function of the years of practice.
This figure presents the scores on the oropharyngeal HPV cancer knowledge questionnaire (minimal score: 0, maximal score: 10) for nurses as a function of the number of years of practice, for control (white dots) and participants receiving the HPV training (black dots). Results were presented as mean ± SEM.
View Figure 2
Evaluations of the one-hour lecture on HPV-associated oropharyngeal cancer demonstrated high scores for the overall evaluation of the training session (9.65 ± 0.08 on 10, max: Nurses, 9.93 ± 0.05; min: GPs, 9.26 ± 0.17), for the evaluation of the teachers (9.84 ± 0.06 on 10; max: Nurses, 10; min: GPs, 9.61 ± 0.14), or for the pertinence of the presented material (9.79 ± 0.06; max: Nurses, 9.97 ± 0.03; min: GPs, 9.52 ± 0.15). Whichever their group, attendants strongly expressed that the information they received during the training session will modify their future practice (9.16 ± 0.18, max: Nurses, 9.4 ± 0.27; min: HNSs, 8.9 ± 0.43, not statistically different from Nurses, p = 0.12, Table 1).
Our study showed that HPV-associated oropharyngeal cancer knowledge is not optimal in first line health professionals, particularly for GPs and nurses. Furthermore, a 1-hour HPV training session resulted in a significant increase of the HPV-associated oropharyngeal cancer knowledge and of the perceived ease to discuss head and neck HPV infections with patients for all 3 professional categories. Human papilloma virus is a sexually transmitted infection that should concern all medical specialties, ranging from gynecology to otorhinolaryngology, from pediatric to oncologic patients [9,10]. Medical staff is the primary source of information for patients [11]. Doctors and nurses are considered the most trustworthy source of information according to a recent Canadian adult survey [12].
Human papilloma virus related to the head and neck site is seldom discussed as part of HPV related health issues. The first survey of HPV providers' vaccination practices and HPV knowledge in Canada since the introduction of school-based vaccination programs published in 2019 asked which potential consequences/benefit did the physicians counsel their patients about with respect to vaccination [12]. Although more Canadians are diagnosed with oropharyngeal cancer secondary to HPV infection than with cervical cancer [4] oropharyngeal cancer was not addressed by this survey. This reflects reality.
Despite being well documented, the link between HPV and oropharyngeal cancer is known enough by the general population, and to a certain extent by health workers. This was confirmed in this study. Cancer caused by HPV has been mainly associated with cervical cancer. The FDA recommended routine vaccination focused solely on female population until 2011. This led to a feminization of HPV awareness centered upon cervical cancer [8]. However, awareness of oropharyngeal cancer caused by HPV was left behind. This is mainly due to the fact that HPV induced oropharyngeal cancer is more prevalent in males. The absence of a screening method and pre-clinical endpoint make it difficult to establish a clear link between vaccination and oropharyngeal cancer prevention [13]. While the baseline knowledge of HPV-associated oropharyngeal cancer was initially not optimal for all categories of health professionals evaluated in this study, all of them showed a significant improvement following the 1-hour training session. Furthermore, all the participants received the training extremely positively, which suggest that this type of educational approach could represent a valid teaching strategy for continuous education on this topic. This reinforces the necessity to improve head and neck HPV awareness for all categories of healthcare professionals. As the goal of this study was to demonstrate feasibility - especially regarding the capacity to reach various categories of first line health professionals both in urban and rural settings - rather than developing a systematic educational program, long-term retention of the knowledge was not assessed. According to a recent Canadian adult survey, medical doctors and nurses are considered the most trustworthy source of information on HPV [12]. Dodd, et al. identified two main factors why discussing HPV related health issues with patient is difficult for head and neck cancer health professionals: Their lack of knowledge, and their reluctance to discuss sexuality with patients [14]. Our study showed that baseline knowledge was better for medical doctors than nurses. However, post-training nurses outperformed control GPs. As the first-line interlocutors of most patients, nurses play a critical role in counselling. Overall, the levels of knowledge on HPV-associated oropharyngeal cancers of the control nurses were very low. From a practical perspective, medical doctors are often contributing to the informal continuous training of nurses. Yet, the fact that medical doctors themselves were not displaying high degree of knowledge nor- and more problematically-high degree of comfort to discuss these topics with patients argues against an optimal inter-professional transmission of knowledge and best practices. Therefore, this emphasises even more the importance of offering such type of HPV-related specific training to nurses, in addition of medical doctors.
Interestingly, younger nurses displayed better knowledge than more experienced nurses. Although that could seem counter-intuitive at first, their good knowledge about HPV could be explained by public health determinants. Indeed, nurses who recently entered in practice belonged to the first female cohort in Canada to systematically receive HPV vaccine. Indeed, between 2007 and 2010, all Canadian provinces implanted HPV vaccination for young girls in the public vaccination program [15]. Despite the recent debates on vaccination emphasise the need for affirmative actions from the medical teaching community [16], HPV vaccination is the prevalent way to fight against the occurrence of HPV-related health issues [17,18]. Therefore, this early life exposition to HPV campaigns is likely to explain, at least partially, the over-performance of younger nurses compared to more experienced ones. Another contributing factor could be the addition of HPV-specific sections in initial professional curricula.
Due notably to anti-vaccination movements, ongoing vaccination campaigns are facing constant challenges [16]. The importance of the dynamic of the patient-doctor relationship is central in the decision-making process of the patient in order for the patient to submit to vaccination, and should not be underestimated. A recent national survey of Canadian adults on HPV demonstrated that the most important barrier to HPV vaccination was to not have a recommendation from a doctor [12]. In this context, our results might be worrisome, as they suggest that without specific training, doctors (either GPs or HNSs) mastery of the subject is not optimal-thus emphasizing the need to develop continuous medical education material on this topic.
Our study presents a few limitations. A potential bias is our sample of control and study population. The study group had a strong prevalence of clinicians working in a university hospital context. Thus, our study is likely to underestimate the real magnitude of lack of knowledge in community primary care units. Participants in the control group have agreed to answer the questionnaires and thus, might have had more interest regarding HPV-related topics, or more broadly, in continuous medical education in general. The second limit in this study is the absence of evaluation of long-term knowledge retention. Testing was performed directly after the training session. Given the specific objectives of this study and the lack of information regarding feasibility, such an evaluation was not added in the design in order to avoid facing dropout problems that would invalidate the study. Thus, we selected an immediate evaluation strategy over long-term measures. Nonetheless, and despite the very positive results on immediate retention, long-term knowledge retention will have to be evaluated in future studies.
Although the management of HPV-positive patients remains highly compartmentalize, this study clearly reinforces the notion that interdisciplinarity and inter-speciality collaboration is central. Medical specialists dealing with head and neck issues should take advantage of the work already done in other specialties. This long-time experience of other speciality translates not just in their individual expertise, but also in the structuring of their continuous education. For instance, gynaecologists have well-developed teaching and counselling tools, that other specialities would benefit to use. Beside its specific focus on HPV oropharyngeal cancers, this study could - both for its methodology and conclusions on the need of cross-disciplinary talk-contribute to a larger scale debate on interdisciplinarity in continuous medical education, for the greatest good of the population we have the care for.
This study evidenced the fact that basic knowledge of first line health professionals concerning HPV-associated oropharyngeal cancer is not what it should be. In addition to initial education, continuous education on HPV-oropharyngeal cancer is needed for first line health professionals, particularly for nurses, and to lesser extend general practitioners. A single 1-hour HPV training session with health professionals resulted in a significant increase of their immediate knowledge and perceived ease to discuss head and neck HPV infections with patients. Initiatives from the medical profession must be taken to improve this issue.
None.
None.
Not applicable.
The data that support the findings of this study are available from the corresponding author, [NA], upon reasonable request.