Background: Orbital floor reconstruction in total maxillectomy cases is a challenging task. Enophthalmos, ptosis, diplopia, dystopia, and contour deformity may result if there is failure of adequate support by the reconstructive measures. Many options of orbital floor reconstruction are available with their inherent complications and no single option may provide the required results in terms of function and esthetics.
Method: Coronoid process can be easily identified after the maxillectomy and carefully sectioned maintaining the temporalis pedicle intact which can be rotated over the temporalis sling to reach the recipient site at the medial portion of the orbital rim.
Results: The coronoid graft was harvested along with the temporalis as a pedicle which could be easily rotated and secured onto the medial portion of the orbital rim to reconstruct the orbital floor in total maxillectomy cases.
Conclusion: In total maxillectomy cases, it is easy to identify and isolate the temporalis pedicled coronoid process graft that is within the proximity and can be rotated over the temporalis sling to reach the medial portion of the orbital rim for secured fixation. The temporalis sling provides additional support to the globe avoiding postoperative complications and being vascularized is helpful if postoperative radiotherapy is planned.
Coronoid graft, Temporalis pedicle, Orbital floor reconstruction, Total maxillectomy, Vascularized graft
Total maxillectomy creates a breach in the supporting framework of the orbit [1]. Successful reconstruction requires repair of the orbital floor to prevent complications. This article describes the technique of recreation of the orbital floor using a temporalis pedicled coronoid process graft. The total maxillectomy patient for Maxillary Synovial Sarcoma who underwent the reconstruction of the orbital floor was retrospectively reviewed. The outcomes in terms of function and esthetics were evaluated. The authors present a method for reconstruction of the orbital floor using temporalis pedicled coronoid process graft and discuss the advantages and disadvantages of this technique. Temporalis pedicled coronoid process graft is a reliable, easily available tissue which can be modified for reconstruction of the orbital floor. It offers outcomes comparable to other techniques without need for extensive surgery [2].
Multiple surgical innovations described to recreate the horizontal and vertical buttresses of the mid-face include palatal prosthesis, soft tissue pedicled flaps, non-vascularized bone grafts (immediate and delayed) in combination with soft-tissue pedicled flaps, free flaps with bone grafting and vascularized osteocutaneous free flaps, including the scapula, fibula, radius and patient specific implants [3].
We describe the technique of temporalis pedicled coronoid process graft for orbital floor reconstruction in total maxillectomy case that was followed up for more than a year with good functional and esthetic outcome.
Under general anaesthesia after the informed written consent, the surgical plan of right maxillectomy with orbital floor resection, partial zygomectomy, orbital reconstruction with right temporalis pedicled coronoid process graft and free vascularized fibula graft for maxillary reconstruction was executed. After total maxillectomy, the coronoid process of the mandible was palpated through the buccal soft tissue. The coronoid process was exposed by meticulous dissection both sharp and blunt, the aim being to free the coronoid from pterygoid musculature. Sigmoid notch was exposed and coronoid process was osteotomized using an osteotome and mallet. One can also use bur and micromotor or reciprocating saw as per the availability. At this juncture it is imperative to watch for ramus fracture. A broad triangular segment was created by extending the osteotomy anteriorly and inferiorly in the direction of third molar. It is necessary to keep the bony segment fairly larger than a traditional coronoidectomy to form a strut that would support the globe medially and have enough space available for fixation (Figure 1). To get the coronoid temporal complex medially, it is essential that its vascular supply is maintained along with the lateral attachments. Miniplate was used to affix the coronoid portion of the flap to the remaining nasal process of the maxilla medially (Figure 2). The remaining surgical defect was closed primarily.
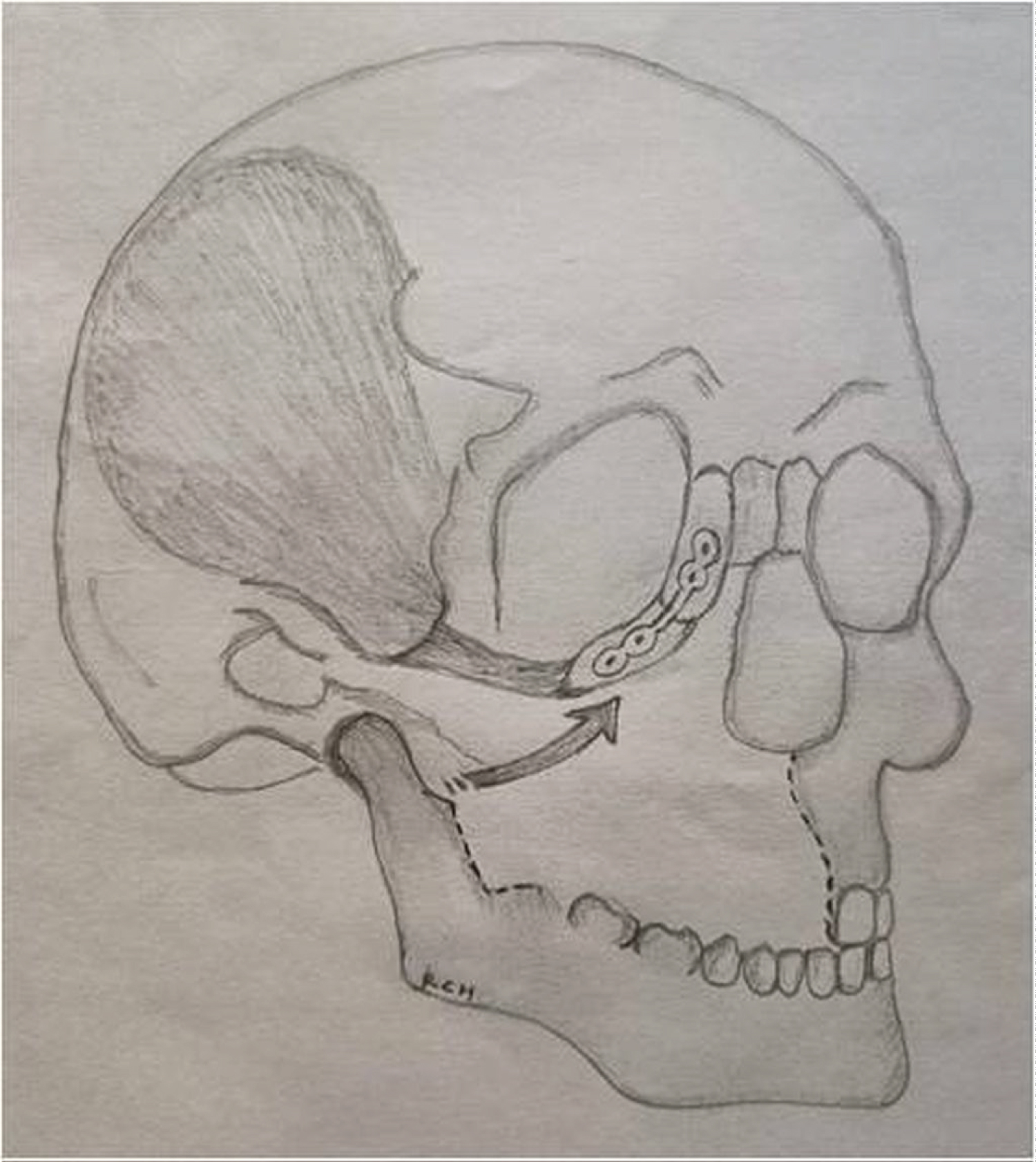 Figure 1: Schematic drawing showing the temporalis pedicled coronoid process graft in situ.
View Figure 1
Figure 1: Schematic drawing showing the temporalis pedicled coronoid process graft in situ.
View Figure 1
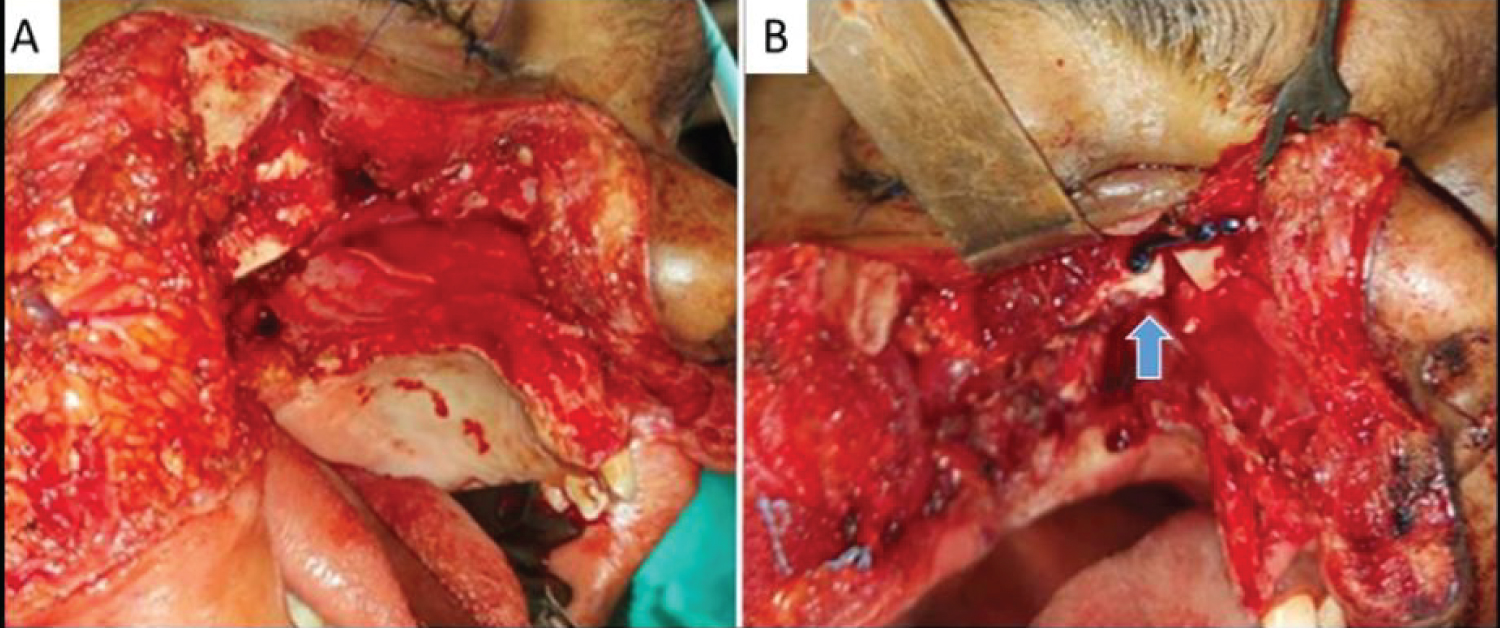 Figure 2: Intraoperative Photos (A) Showing surgical defect post total maxillectomy of right side; (B) Temporalis pedicled coronoid process graft post fixation denoted by an arrow.
View Figure 2
Figure 2: Intraoperative Photos (A) Showing surgical defect post total maxillectomy of right side; (B) Temporalis pedicled coronoid process graft post fixation denoted by an arrow.
View Figure 2
Post-surgical histopathology report of the maxillectomy specimen showed undifferentiated spindle cell tumor suggestive of monophasic synovial sarcoma with all borders free of tumor. Patient is on a regular follow up with good functional and esthetic outcome (Figure 3).
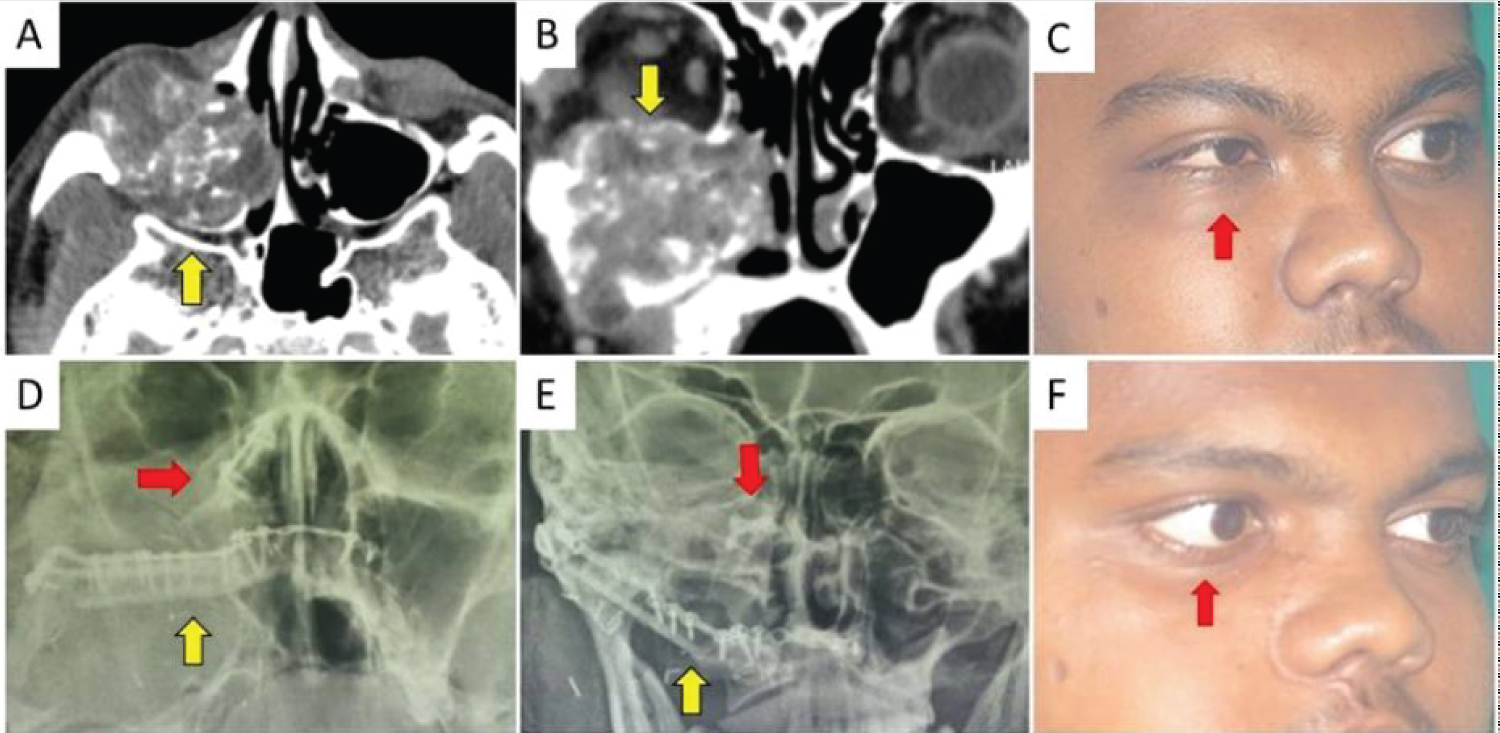 Figure 3: Preoperative and Postoperative comparison (A) Preoperative CT scan axial section showing expansion of posterior maxilla denoted by an arrow; (B) CT scan coronal section showing tumor spreading into intranasal compartment and floor of orbit (arrow); (C) Preoperative right oblique lateral photograph showing proptosis of right eye and right infraorbital swelling denoted by an arrow; (D) Post operative PNS view radiograph showing plate fixing coronoid process to medial nasal bone (horizontal arrow) and plates fixing fibula to right zygoma and left maxilla (vertical arrow); (E) PA view radiograph showing plate fixing coronoid process to medial nasal bone (inverted arrow) and plates fixing fibula to right zygoma and left maxilla (arrow); (F) Postoperative right oblique lateral photograph showing complete symmetry excepting mild ectropion of right eye denoted by an arrow.
View Figure 3
Figure 3: Preoperative and Postoperative comparison (A) Preoperative CT scan axial section showing expansion of posterior maxilla denoted by an arrow; (B) CT scan coronal section showing tumor spreading into intranasal compartment and floor of orbit (arrow); (C) Preoperative right oblique lateral photograph showing proptosis of right eye and right infraorbital swelling denoted by an arrow; (D) Post operative PNS view radiograph showing plate fixing coronoid process to medial nasal bone (horizontal arrow) and plates fixing fibula to right zygoma and left maxilla (vertical arrow); (E) PA view radiograph showing plate fixing coronoid process to medial nasal bone (inverted arrow) and plates fixing fibula to right zygoma and left maxilla (arrow); (F) Postoperative right oblique lateral photograph showing complete symmetry excepting mild ectropion of right eye denoted by an arrow.
View Figure 3
Surgical reconstruction of the orbitomaxillary complex is inherently challenging as it needs to encompass the requirements of preserving and supporting the orbital contents, prevent ascending infection from nasopharynx by obliterating the communication, reconstruct palatal surface and be cosmetic. Complications such as enophthalmos, ectropion, diplopia, dystopia, global ptosis, and severe facial contour deformity may result [4]. A local vascularized temporalis pedicled coronoid process graft restores the support, contour, and projection that the infraorbital rim provides. The coronoid process of the mandible is in close proximity to the maxillectomy defect and minimal dissection is necessary to identify this structure and free it from the surrounding tissues. The technique is similar to coronoidectomy except that the temporalis muscle attachments are to be preserved as it will act a sling and provides vasculature to the graft. It is important to note that the inferior alveolar nerve is placed at risk as it enters the mandibular foramen directly inferior to the base of the coronoid. Basing the pedicle on the temporalis blood supply stemming from the deep temporal artery provides a healthy bed as the patient was planned for post-operative chemo-radiotherapy. The temporalis pedicled coronoid process graft for orbital floor reconstruction in total maxillectomy cases is easy to harvest, reliable as it is a vascularized graft, supports global contents and restores the function and esthetics.
Anatomically based vascularized grafts are known to provide long term functional and esthetic results. Also, the close proximity of the graft has better chances of survival compared to the distant grafts. In total maxillectomy cases, it is easy to identify and isolate the temporalis pedicled coronoid process graft that is within the proximity and can be rotated over the temporalis sling to reach the medial portion of the orbital rim for secured fixation. The temporalis sling provides additional support to the globe avoiding postoperative complications and being vascularized is helpful if postoperative radiotherapy is planned.
Nil.
All the authors have contributed equally to literature search, surgical technique, drafting the manuscript, proof reading and uploading.