Double J or JJ ureteral stents are used daily in urology and have various indications. However, if forgotten or neglected, they can cause serious complications that can jeopardize the functional prognosis of the kidney and the patient's vitality. We are reporting a case of significant calcification and encrustation of bilateral double J ureteral stents that have been neglected for five years causing obstructive pyelonephritis and renal failure, posing a management challenge.
Double J-stent, Complication, Endourology, Pyelolithotomy
Double J ureteral stents have been commonly used in urological practice since their first introduction, but they are not without complications. The complications associated with them are essentially mechanical (catheter migration, encrustation, formation of stones). Double J catheters act as foreign bodies and can cause a urinary infection (pyelonephritis or pyonephrosis which can lead to kidney damage). Therefore, the removal of a double J stent or change should be done as soon as possible to reduce any complications or morbidity [1]. We are reporting a historical case of significant calcification and encrustation of a neglected bilateral double J ureteral catheter over the past five years responsible for an obstructive pyelonephritis and renal failure, first endoscopic management supplemented by conventional surgery.
Patient, 42-years-old, diabetic on insulin for 15-years, followed for bilateralurolithiasis having benefited from an endoscopic bilateral double j ureteral stent for the right renal stones and the left pelvi-ureteral stone and then the patient Lost to follow-up. Consulting at the emergency departements five years after the double J stenting for a febrile lumbar pain and shivering associated with irritative lower urinary tract disorders with cloudy urine. Clinically, the patient was stable, with performance status equal to 1, with bilateral low back pain and positive sign of shivering. The temperature was 38.3 C. The urinary tree showed bilateral double J stents in place with calcification in the proximal and distal ends and ureteral segments.
The additional scans (Figure 1) showed bilateral hydronephrosis with calcification of the bilateral JJ stents more marked on the left, as well as infiltration of bilateral peri-renal fat.
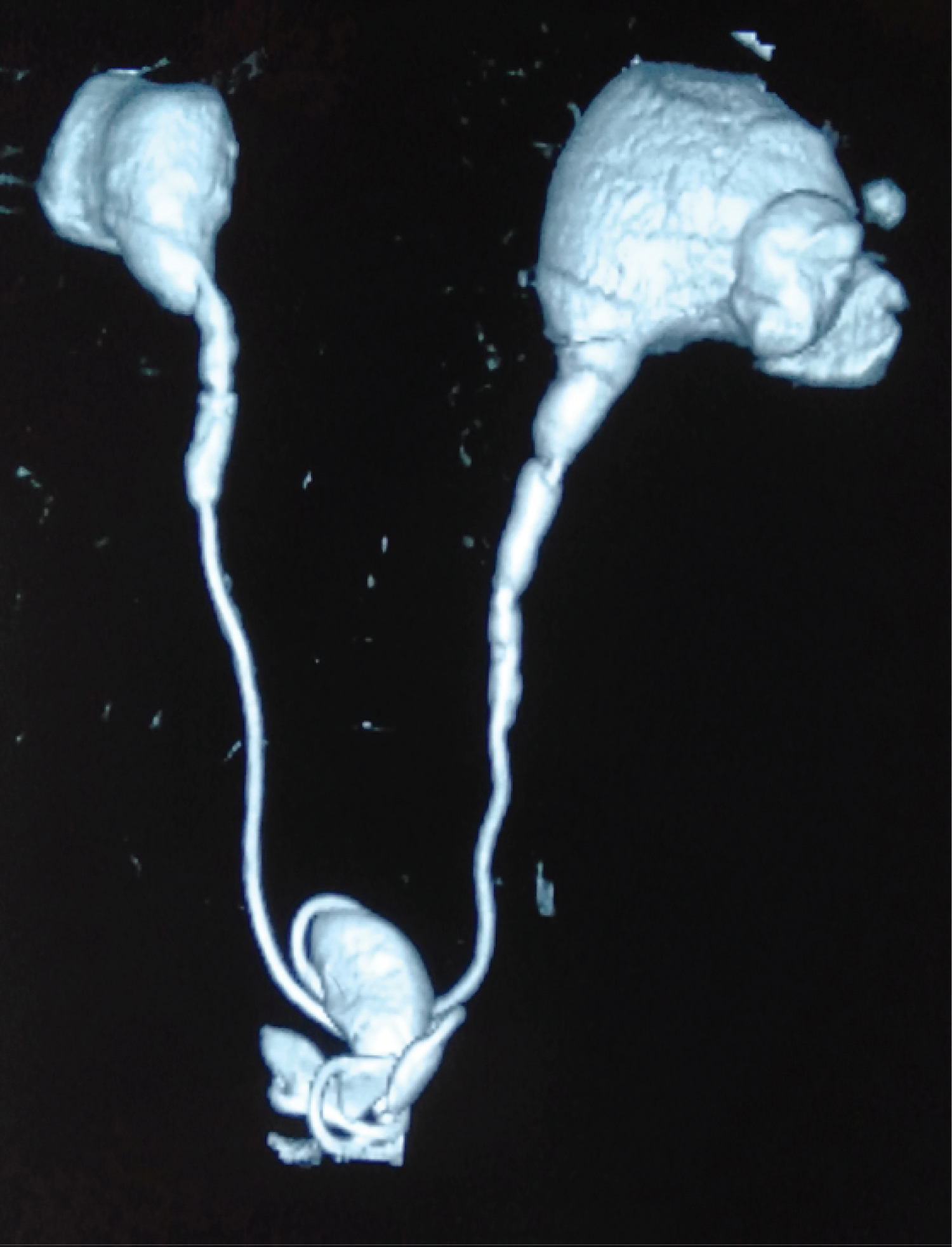 Figure 1: Calcification of bilateral ureteral stents.
View Figure 1
Figure 1: Calcification of bilateral ureteral stents.
View Figure 1
Biologically, an infectious syndrome is associated with renal failure. Capillary blood glucose was 3.2 mg/dl with 7% glycated haemoglobin. The emergency procedure was the setting up of a bilateral nephrostomy, antibiotic therapy, rehydration and glycemic control. At a distance from the acute episode, a laser fragmentation (Figure 2) of the intra bladder and ureteral calcification was first performed and then a pyelolithotomy for extraction of the encrusted renal stones with double J stenting (Figure 3).
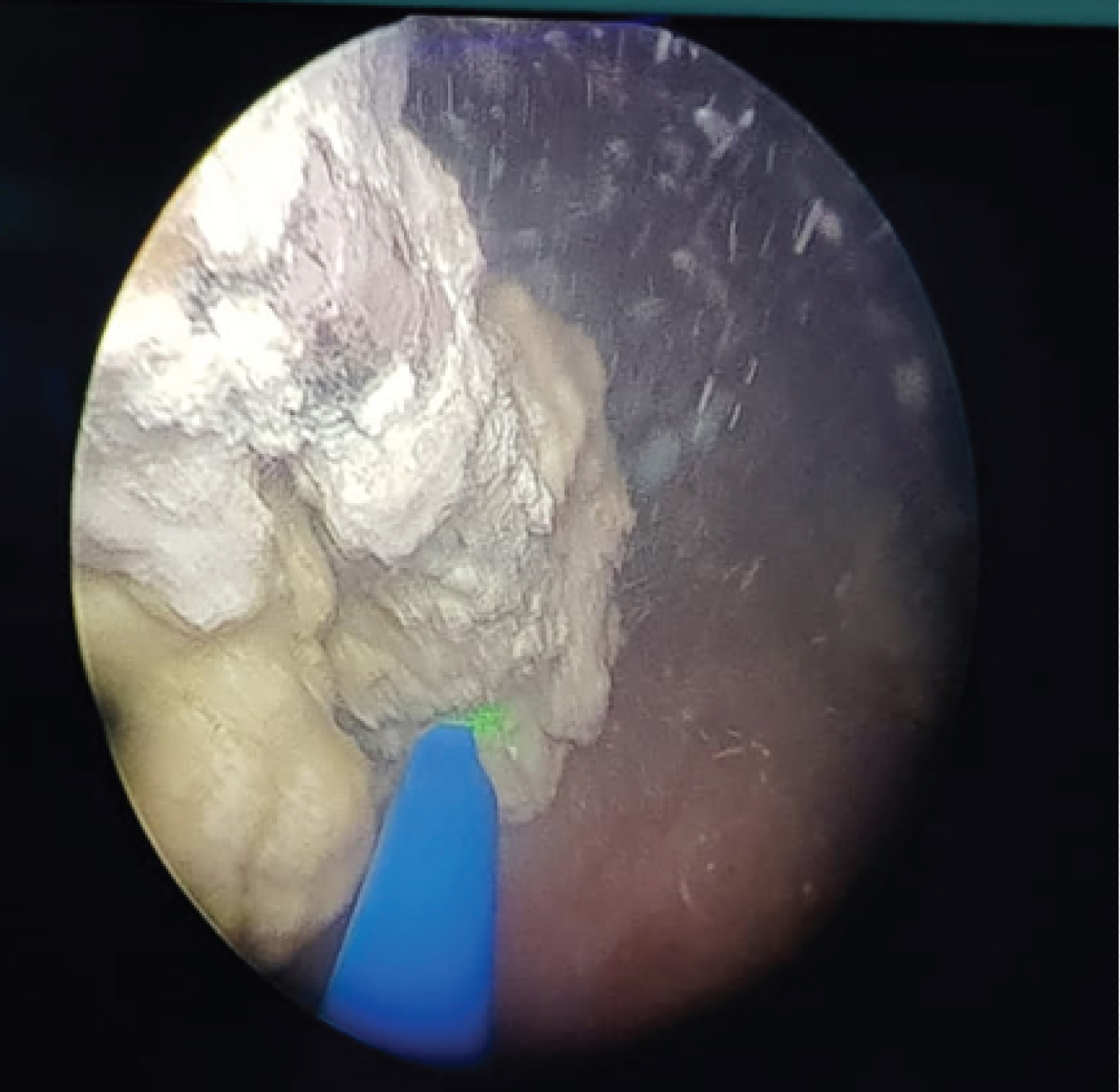 Figure 2: laser fragmentation of calcifications.
View Figure 2
Figure 2: laser fragmentation of calcifications.
View Figure 2
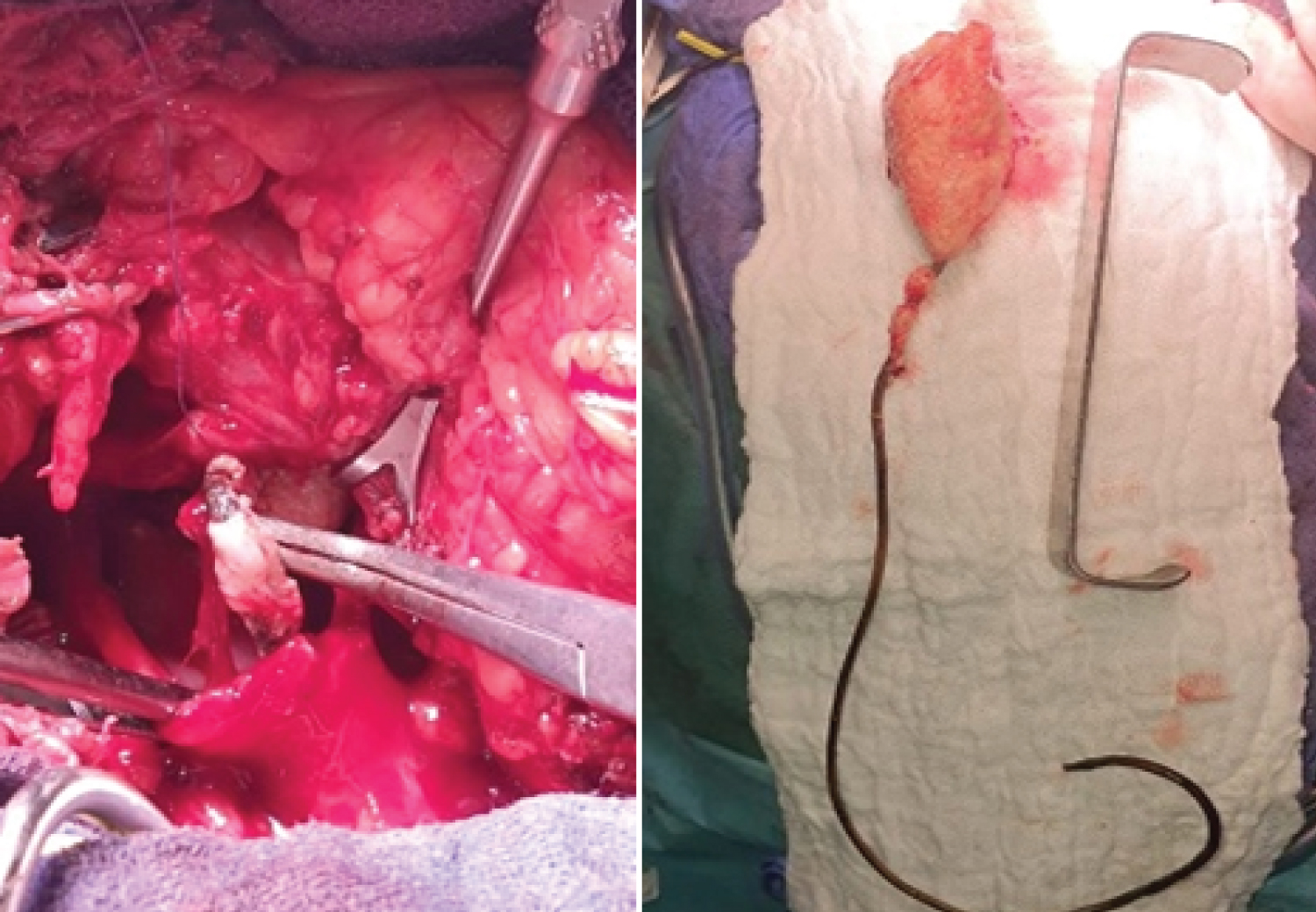 Figure 3: Intraoperative vision and the extracted stent.
View Figure 3
Figure 3: Intraoperative vision and the extracted stent.
View Figure 3
The post-op follow-up was simple. The evolution was favourable.
The double J ureteral stent is commonly used in urological practice. It can be inserted for a short period of time (4-6 weeks) to help the ureter to heal, drain urine and prevent shrinkage during healing. In the long term, especially if kept for more than 6 months, it can lead to serious complications [2]. The duration of the double J stents in our patient was 5-years.
Long-term complications are associated with the length of time that the double J stent is worn. Forgotten or neglected stents over a period of time can endanger easily the kidney function. Over time, the double Jstents will lose their function and can cause complications [3].
Several factors can lead to calcification or encrustation of the stent: prolonged duration of the JJ stents, history of lithiasis, urinary tract infections, chemotherapy, metabolic or congenital abnormalities, and chronic kidney failure [4]. Five of these factors were present in our patient: prolonged duration of JJ stenting, history of lithiasis, urinary tract infections, metabolic abnormalities, and chronic renal failure.
The clinical presentation of complicated JJ stents is varied. Ranging from migration in 9.5% of cases, higher fever in 12.3% of cases, haematuria in 18.1% of cases, lower urinary tract irritation in 18.8% of cases, encrustation in 21.6% of cases and lumbar pain in 25.3% of cases [5]. We have reported low back pain associated with fever and irritating lower urinary tract disorders. In addition to the described signs, a shivering was encountered in our patient.
The management of complicated ureteral stent requires a combination of medical, endourological and/or open surgical techniques. Complications related to JJ stents are mainly managed by endoscopic procedures with a high success rate. Open or laparoscopic surgery is only indicated if endoscopic techniques have failed. In case of a non-functional kidney, a nephrectomy may be indicated [1]. Our emergency treatment consisted of bilateral urinary diversion by nephrostomy. At a distance from the acute episode (pyelonephritis), laser fragmentation of the intra vesical and ureteral calcifications was carried out in the first stage followed by extraction of the encrusted right renal stones by lombotomy in a second stage.
There are no clear recommendations on the management of calcified and inlaid double J stents. In the case of calcification associated with an inlay, laser endoscopic management can be performed for bladder and ureteral calcification. Open surgery can be performed for the removal of the inlay.