Anaesthetic challenges involving removal of endobronchial growths are numerous. Use of rigid bronchoscopy, electrocautery, cryoprobe apart from the need of continuous communication and monitoring are essential part of this unique anesthetic care. We report two cases of endobronchial tumors which were removed under general anesthesia.
Bronchial neoplasm, Bronchoscopic surgery, Electrocautery, Intravenous anesthesia
Bronchial neoplasms are difficult to treat and can cause hypoxia, haemoptysis or post-obstructive pneumonia [1,2]. In such a case, bronchoscopic surgery is a safe and effective treatment modality [3-6]. Anesthetic management in these cases is very challenging with problems in oxygenation, ventilation, bleeding into airways, airway burns, airway edema, airway trauma and exaggerated hemodynamic responses [7]. We discuss anesthetic management of two cases of endobronchial growth which was removed using rigid bronchoscope aided by electrocautery and cryoprobe [8,9]. Use of newer equipments with rigid bronchoscope poses specific challenges which need special precautions as they may be unfamiliar [2].
A 66-year-old male, diabetic and hypertensive presenting with fever and cough for a week was diagnosed to have right endobronchial growth (Figure 1) and post obstructive pneumonia in right lower lobe, confirmed with Chest X-ray (Figure 2), Computed Tomography (CT) Thorax and flexible bronchoscopy (Biopsy - squamous metaplasia). Pre-operative optimization included a course of antibiotics and bronchodilator therapy. Consent included explanation of risks of airway bleeding, trauma, perioperative airway oedema and remote chances of postoperative ventilation. Sedation the day before surgery was avoided. Standard monitoring was done. Well-functioning suction apparatus, Double lumen tube (DLT) and bronchial blocker were kept standby for lung isolation in case of massive airway bleeding. Maximum allowable neck extension was checked prior to induction with shoulder roll and head ring. Patient was preoxygenated with 100% Fraction of Inspired Oxygen FiO 2 , premedicated with glycopyrrolate 10 µg/kg, ondansetron 0.15 mg/kg, fentanyl 2 µg/kg and induced with propofol 2 mg/kg and paralyzed with atracurium 0.5 mg/kg. 11 mm rigid bronchoscope was passed after positioning with neck extension by pulmonologist. Ventilation was done via side port with intermittent apnoeic periods. Arterial line was secured and transduced. Anaesthesia was maintained with propofol infusion 10-15 mg/kg/hr throughout the case, depth of anaesthesia monitored by Bispectral Index (BIS) adjusted to 40-60. Analgesia was provided with repeated doses of fentanyl 0.5 µg/kg at half hourly intervals and IV paracetamol 1g. FiO 2 was kept at 0.5 and reduced to 0.3 at the times of cautery use to prevent airway burns. Higher flows of 5 to 6 litres/minute were used throughout the case. Atracurium boluses of 10 mg was given every 30 minutes. Blunting of sympathetic responses was done with esmolol infusion, bolus of 500 µg/kg over 10 minutes followed by infusion of 50-100 µg/kg/min. Steroids in the form of intravenous hydrocortisone 100 mg and dexamethasone 8 mg was given to prevent airway oedema. Endobronchial mass was detached using electrocautery and extraction was done piecemeal using cryoprobe as it was difficult to remove en masse. Minimal bleeding was noted, managed by suctioning. Final check scopy showed patency of all bronchi. Thorough suctioning and xylocard 1 mg/kg sprayed into the airway at the end of procedure. After removal of bronchoscope intubation with size 8.0 mm endotracheal tube was done and ventilated for about 15 minutes. Arterial Blood Gas (ABG) done following the procedure was normal. Patient was extubated uneventfully and was monitored in Intensive Care Unit (ICU) for 24 hours. We did not encounter any significant postoperative complications.
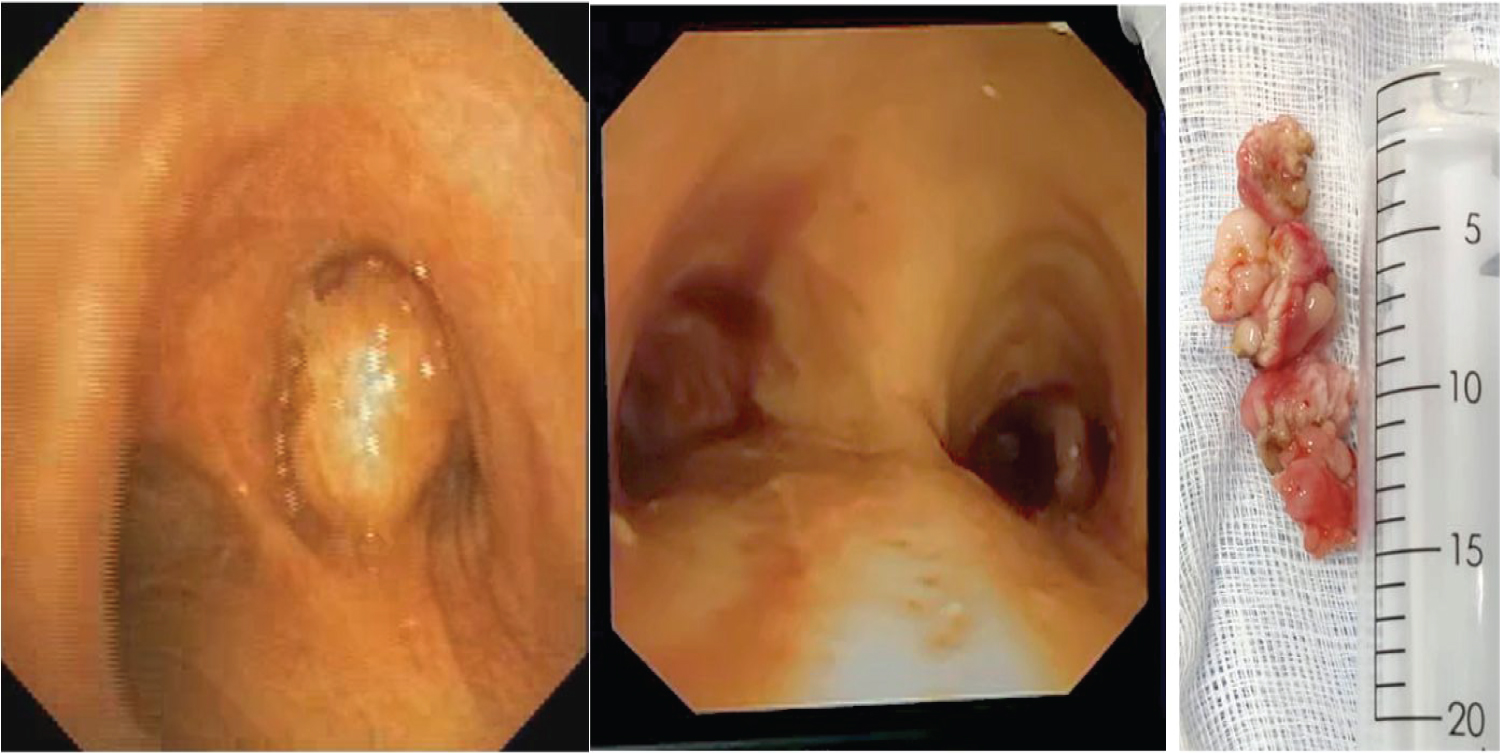 Figure 1: Bronchoscopic view of carina before and after removal of right endobronchial tumor and picture of gross specimen (case 1).
View Figure 1
Figure 1: Bronchoscopic view of carina before and after removal of right endobronchial tumor and picture of gross specimen (case 1).
View Figure 1
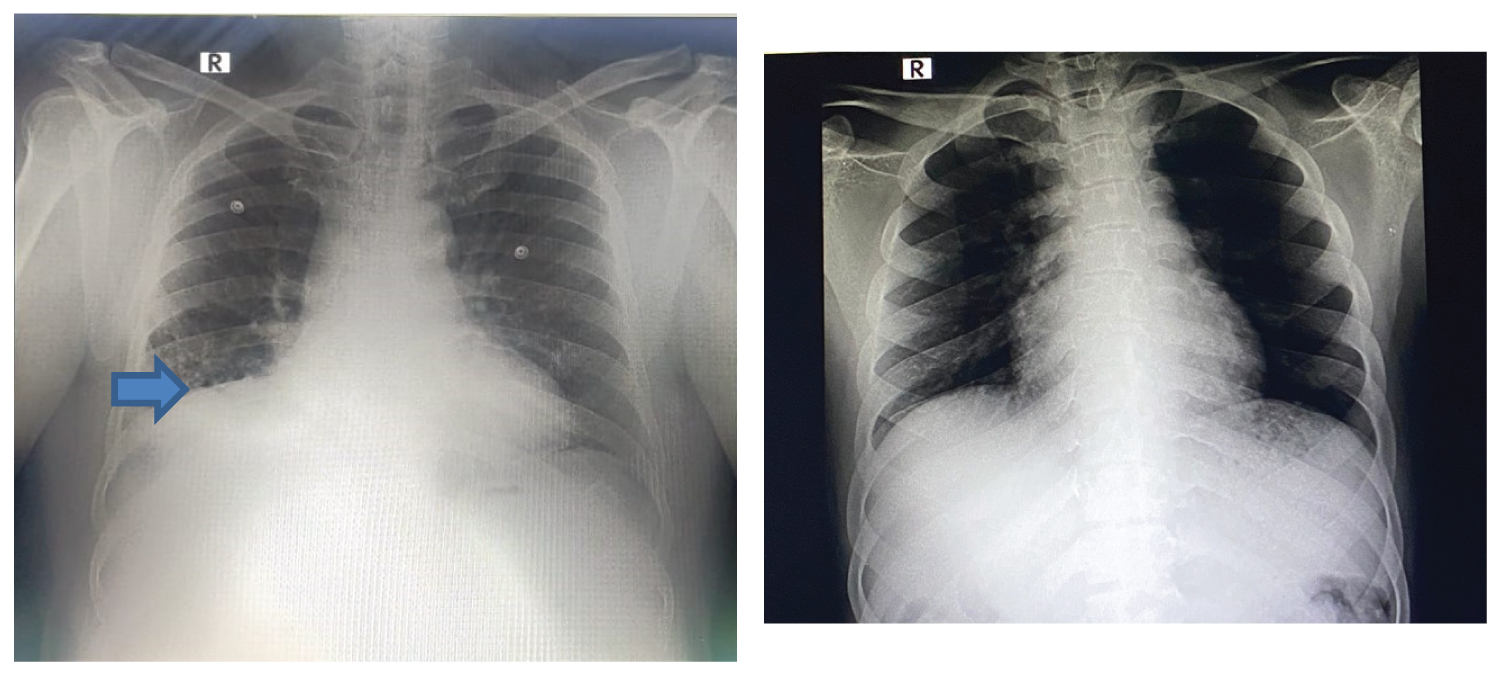 Figure 2: Chest X-ray before and after debulking of tumor. Blue arrow indicates the non-homogenous opacity in the right lower zone (case 1).
View Figure 2
Figure 2: Chest X-ray before and after debulking of tumor. Blue arrow indicates the non-homogenous opacity in the right lower zone (case 1).
View Figure 2
A 35-year-old male, presented with respiratory symptoms was diagnosed to have left main bronchus growth, confirmed with CT Thorax and bronchoscopy (Figure 3). Antibiotics and bronchodilators were given. Written informed consent was taken. Patient was shifted to Operation Theatre (OT); standard monitoring including invasive arterial monitoring was done. The extent to which cervical extension was comfortable to the patient was checked preoperatively. After induction of anesthesia with propofol and atracurium, 11 mm rigid bronchoscope was passed, ventilation via side port was done. Anaesthesia was maintained with propofol infusion 10-15 mg/kg /hr with BIS monitoring. Intraoperative analgesia was with fentanyl and paracetamol. FiO 2 was reduced to 0.3 at the times of cautery. Higher flows were used. Atracurium boluses were given. Sympathetic responses were blunted with dexmedetomidine infusion (bolus 1 µg/kg followed by infusion of 0.3 µg/kg/min) and esmolol infusion of 50-100 µg/kg/min was used as rescue. Steroids were gives. As the mass was in the left bronchus (larger angulation) the access was difficult to remove by electrocautery. Only part of Endobronchial mass could be detached from the wall and piecemeal extraction with cryoprobe was done. Significant bleeding was noted, managed by suctioning and cautery. No desaturation was observed. DLT and bronchial blocker was kept standby for lung isolation in case of massive airway bleeding. Final check scopy showed patency of all bronchi. Post procedure intubation was done and patient was extubated uneventfully and monitored in ICU for 24 hours. We did not encounter any significant postoperative complications.
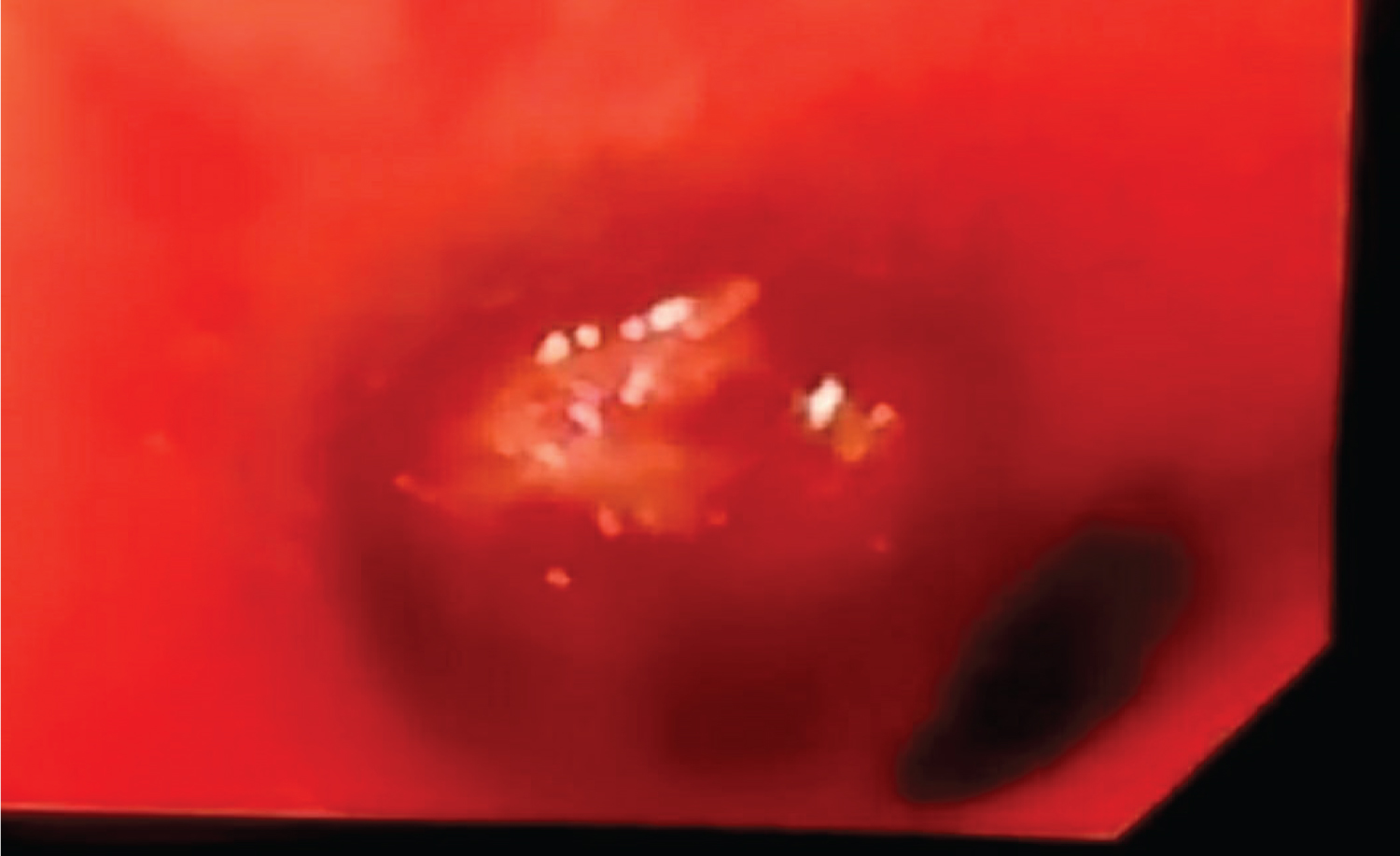 Figure 3: Bronchoscopic view of left endobronchial tumor (case 2).
View Figure 3
Figure 3: Bronchoscopic view of left endobronchial tumor (case 2).
View Figure 3
Anesthetic challenges were many including preoperative preparation, intraoperative mode of ventilation, choice of anesthesia, use of newer devices and continuous communication and patient monitoring. Preoperative evaluation (CT scan and bronchoscopy), nebulization with beta2 agonists and antibiotic course was necessary in both cases [3,8]. Pre-anaesthetic evaluation involved complete assessment of patient’s airway, ruling out an active lower respiratory tract infection, explaining the chances of intraoperative and post-operative airway oedema and need for postoperative mechanical ventilation and need for an intensive care unit stay. Prevention of airway edema is of utmost importance in rigid bronchoscopy and therefore steroids were used. Patients during bronchoscopy are positioned in neck extension.
Assessment of range of neck extension in an awake patient helps us understand the allowable limit so as to avoid any cervical spine injury [2]. Preoperative sedation was avoided to prevent any hypoventilation. There are different methods of ventilation through rigid bronchoscope including side-port ventilation, intermittent apnoea and ventilation, jet ventilation techniques, etc [2]. In both the cases we adopted for hand ventilation via side port as it gives us better judgement of ventilation in the absence of End tidal carbon dioxide (ETtCO2). Total intravenous anesthesia (TIVA) was used with propofol in both cases to avoid OT pollution, wastage of anesthetic gases and to maintain steady depth of anesthesia [2]. BIS was used in both the cases for depth of anaesthesia monitoring [2]. Arterial monitoring was done to have a better control of systemic pressures and to titrate doses of antihypertensive agents as exaggerated sympathetic responses are common during rigid bronchoscopy [2]. Blunting of hemodynamic responses was done with esmolol infusion in the first patient while dexmedetomidine along with esmolol in the second patient. First patient being elderly and hypertensive had more hemodynamic responses. Caution was taken to make sure FiO 2 was 0.3 during the use of cautery to prevent airway burns [2]. Bleeding during the rigid bronchoscope and difficulty in retrieval was more in the second patient as tumor was in left bronchus (larger angulation). Bleeding in both cases could be controlled with effective suctioning and cautery [1,7]. There was no need for the use of lung isolation techniques. These patients have irritant cough post procedure which needs effective prevention. Use of local anesthetic spray helped in both cases. Care was taken in both cases to avoid any airway injury. Effective communication between anaesthesiologist and pulmonologist was necessary during crucial phases of procedure like insertion and removal of bronchoscope, use of cautery and cryoprobe, retrieval of tumour as it is important to prevent lapses [1,3,7].
Anaesthetic management of rigid bronchoscopic guided removal of endobronchial tumours involves challenges with regards to airway burns, airway bleeding and issues with use of newer therapeutic devices in addition of well-known challenges relating to oxygenation, ventilation, airway oedema, trauma and exaggerated hemodynamic responses. These can be successfully managed without major complications with proper preoperative planning and optimization and effective implementation including good communication among the personnel involved.