Posterior reversible encephalopathy syndrome (PRES) is a neurological ailment with specific radiological findings [1]. PRES is an aggregate of focal reversible vasogenic oedema in brain imaging along with neurological signs and symptoms of headache, seizures, encephalopathy and visual disturbances. The radiographic lesions in PRES commonly involve the posterior parieto-occipital white matter bilaterally, however might also extend to the cortex, frontal lobes, basal ganglia and brain stem [2]. Here, we are presenting two patients who developed PRES after delivery.
The first patient, a 20-year-old woman who underwent a caesarean section under spinal anaesthesia complained of a headache immediately after surgery and experienced a generalised tonic-clonic seizure 4 hours later. Vitals remained stable. Supplemental oxygen, midazolam, magnesium sulphate, levetiracetam, mannitol, furosemide, and steroids were used to treat the patient. The results of a brain MRI showed subcortical vasogenic edoema suggestive with PRES and bilaterally symmetrical areas of altered signal intensity in the fronto-parieto-occipital and right basal ganglia. Within 4 days, the patient had improved (Figure 1 and Figure 2).
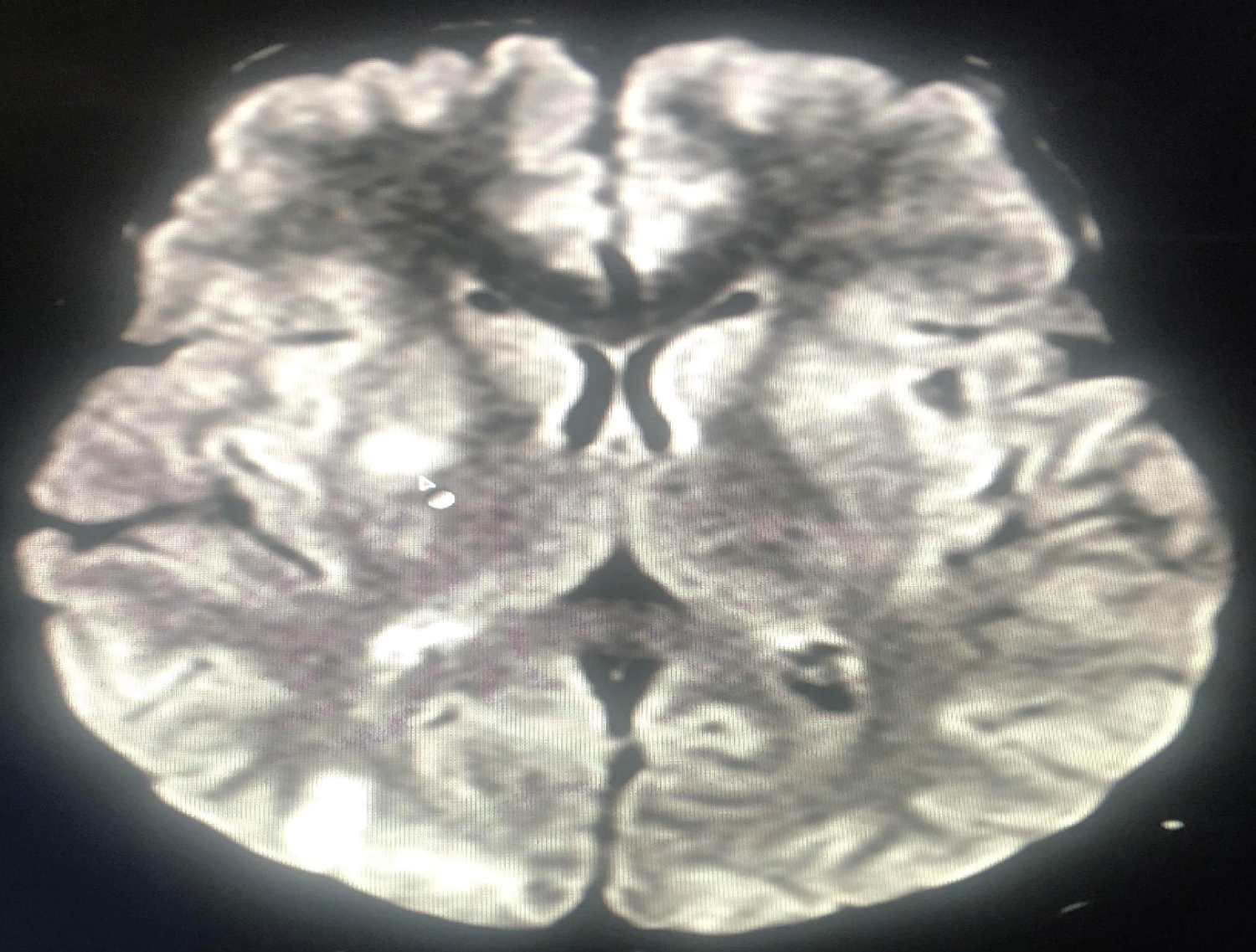 Figure 1: MRI Brain depicting areas of altered signal intensity in right basal ganglia region.
View Figure 1
Figure 1: MRI Brain depicting areas of altered signal intensity in right basal ganglia region.
View Figure 1
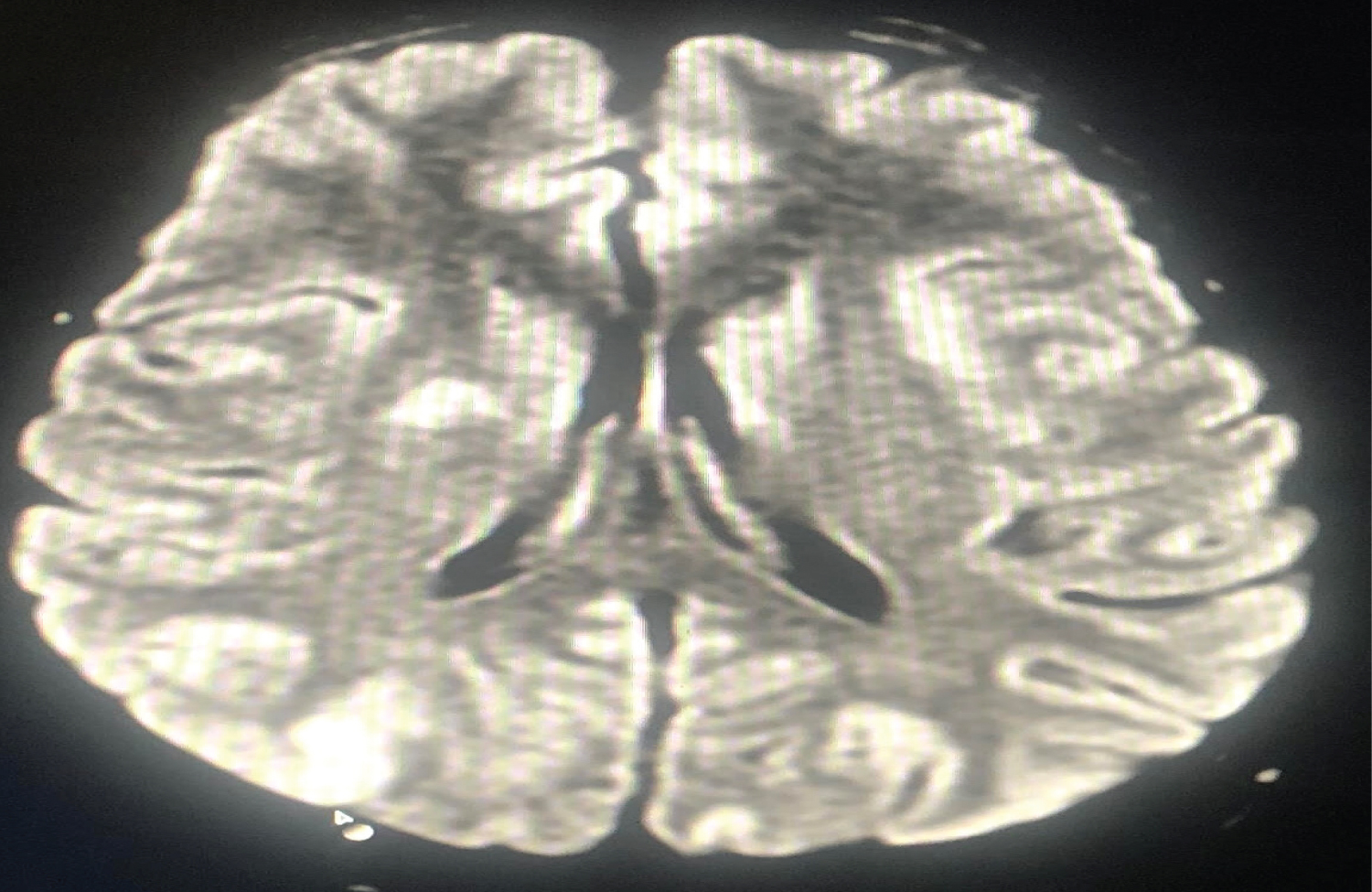 Figure 2: MRI Brain depicting symmetrical areas of altered signal intensity in right parieto-occipital region.
View Figure 2
Figure 2: MRI Brain depicting symmetrical areas of altered signal intensity in right parieto-occipital region.
View Figure 2
Another patient with a history of postpartum generalised tonic-clonic seizures was admitted to the emergency department. Patient was unconscious, with a pulse rate of 105 beats per minute, a blood pressure of 190/110 mmHg, and a GCS of 7/15. There was no prior history of pregnancy-related hypertension or epilepsy. The patient was managed with magnesium sulphate, levetiracetam, mannitol, furosemide, steroids and was started on nitroglycerin infusion for 24 hours while still on ventilator support. Thereafter, labetalol infusion was administered. The NCCT brain revealed bilateral parieto-occipital cortical and subcortical regions with symmetrical hypodense areas, which is suggestive of PRES. Patient spent 10 days in ICU without any incidence of seizures before being transferred to the ward (Figure 3).
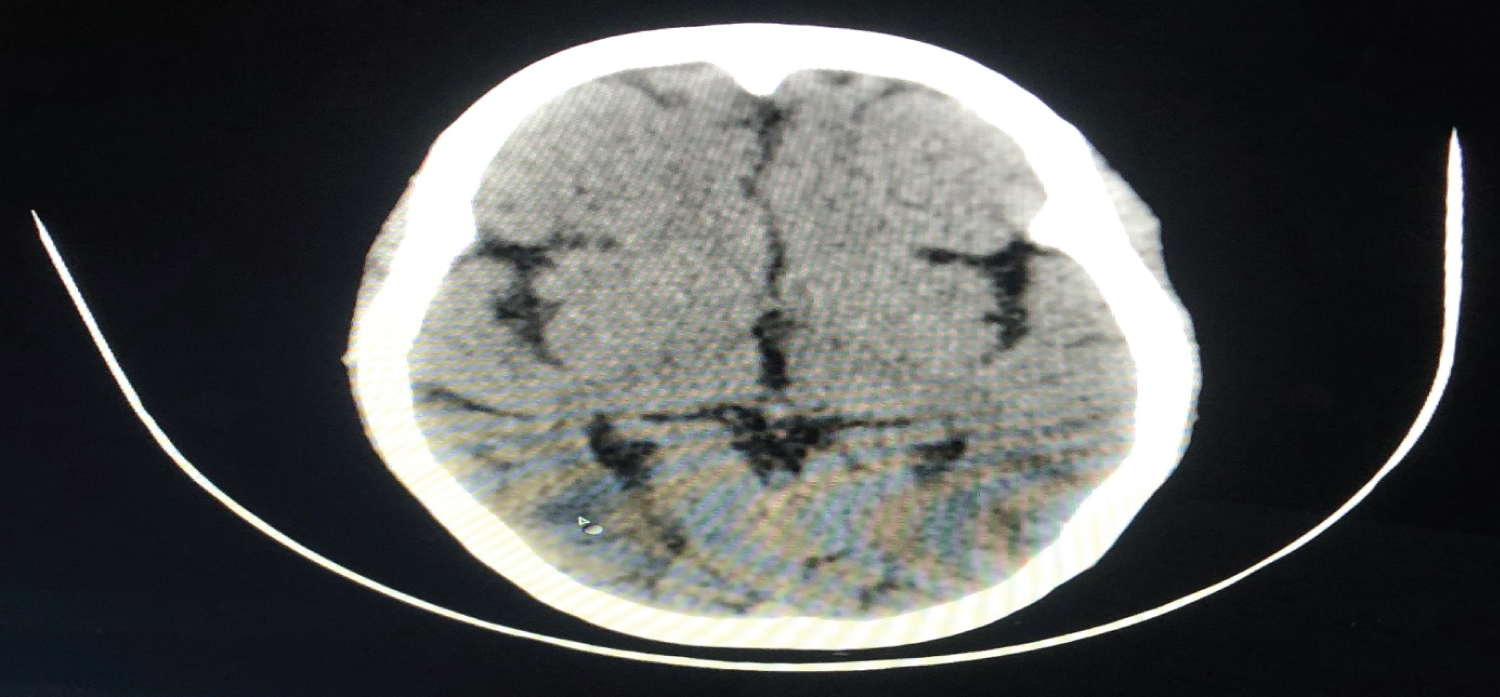 Figure 3: NCCT head showing symmetrical hypodense areas involving cortical and subcortical region of bilateral parieto-occipital region.
View Figure 3
Figure 3: NCCT head showing symmetrical hypodense areas involving cortical and subcortical region of bilateral parieto-occipital region.
View Figure 3
PRES has been reported in nearly all age groups, however is considered more commonly in young- or middle-aged adults with a preponderance of female patients, which would possibly be attributable to etiological aspects [3]. Various conditions associated with PRES include hypertension, preeclampsia, eclampsia, immunosuppressant therapy, chemotherapy or autoimmune disorders [4]. Pronounced fluctuations of blood pressure, rather than absolute blood pressure increase, might precede the syndrome [5].
Clinical symptoms and signs include encephalopathy, seizures, headache, visual disturbances, focal neurological deficit, and status epileticus [5]. Although, most typically viewed in patients with hypertension and preeclampsia/eclampsia however in our cases, patients had no history of hypertension and seizures during pregnancy.
The pathophysiology of PRES stays incompletely understood. One principle postulates that acute hypertension exceeding the autoregulatory potential of the cerebral vasculature leads to hyperperfusion, which in turn causes a breakdown of the blood-brain barrier, allowing the formation of vasogenic oedema. An alternative principle posits that vasoconstriction secondary to evolving hypertension producing hypoperfusion should be accountable for the development of PRES [6]. MRI is the modality of choice for analysis of PRES. It usually suggests bilateral symmetrical vasogenic subcortical edema in the parieto-occipital areas of both cerebral hemispheres. Other frequently seen patterns include patchy edema in the frontal lobes or confluent vasogenic oedema of the frontal, parietal and occipital lobes with sparing of the temporal lobes. Hypodensities in the typical topographical distribution in CT are suggestive of PRES [6].
Therapeutic techniques consist of generalized supportive therapy with blood pressure regulation, management of seizures and anti-edema therapy. 40% of the cases may additionally require mechanical ventilation to prevent cerebral hypoxia, hypercarbia and increased intracranial pressure and the related adverse neurological outcome [6].
PRES is a reversible syndrome which requires high degree of suspicion for early diagnosis. Clinician need to be vigilant when patient develops headache, seizures, visual disturbances or neurological deficit. Brain imaging is vital for its diagnosis. If recognized at an early stage and managed timely, the underlying pathology can be reversed, thereby, preventing the irreversible neurological sequelae and fatalities.