All stages of general anesthesia have a dose-dependent effect on the redistribution of body heat from core to peripheral regions with various mechanisms by peripheral vasodilation, arteriovenous shunt expansion, increased sweating threshold and shivering. Normally the body core temperature is just regulated within 0.2 ℃ but this temperature control range becomes wider under general anesthesia. As a result; body core temperature decrease due to impairment of the normal thermoregulatory control.
It is well known that female reproductive hormones affect the body core temperature during the menstrual cycle. In luteal phase; progesterone level increases and reaches the highest values in the middle of the luteal phase after that body core temperature is influenced by thermogenic effect of progesterone and increases 0.4 ℃ approximately [1]. Some studies have found that the concentration of progesterone is correlated with the threshold for sweating and skin blood flow during exercise beside the elevated core temperature [2-4]. Also in luteal phase of menstrual cycle increased threshold for cutaneous vasodilatation during passive heating or cooling [5,6]. Therefore increased core temperature may associated with altered thermoregulatory control in the luteal phase of menstrual cycle. In addition; there is no studies on how various stages of menstrual cycle influence thermoregulatory responses to anesthesia. In our study we compared the both skin and core temperature changes between the follicular and luteal phases of the menstrual cycle during general anesthesia procedure.
This study was registered to Australian New Zealand Clinical Trial Registry with serial number ACTRN12614000286640. After institutional review, board approval and informed consent 50 female patients; ASA (American Society of Anesthesiologists) class 1, ages between 18-45 years old were enrolled in this study. The surgeries performed were septorhinoplasty and tympanoplasty. 25 patients with menstrual cycle days from 1 to 10 (follicular group), 25 patients with menstrual cycle days from 18 to 24 (luteal group) were included in the study. Exclusion criteria were diabetes, thyroid disorders, obesity, irregular menstrual cycle and oral contraceptive usage.
None of the patients was premedicated. All of the patients were monitored "Dräger infinity delta XL" to measure continuous noninvasive blood pressure, electrocardiograms, capnograms, core temperature and skin temperature. The skin temperature probe was installed in the middle of the forearm where the non-invasive blood pressure cuff was not bound. The intravenous fluid was used at the room temperature intraoperatively and fluid administration was given from the arm that skin temperature probe was not installed. The core temperature was measured with esophageal probe immediately after the intubation. The operating room temperature was maintained between 21-22 ℃. Anesthesia was standardized in all patients and induced with propofol 2 mg/kg IV and rocuronium 0.5 mg/kg IV. Anesthesia was maintained with remifentanil infusion and sevoflurane in a mixture of nitrous oxide 1 L/min and oxygen 1 L/min. The entire body was covered with the sheet of surgical drape except for the field of the surgery performed. Post-anaesthetic shivering seen at the end of the operation after extubation was evaluated by 4-degree scale at recovery room (Table 1). All measurements were recorded at 15 minute intervals.
Table 1: Shivering Scale. View Table 1
Data analysis was performed using SPSS v.16.0 software. The student T-test used to analyze core and skin temperature, BMI (Body Mass Index), age, mean blood pressure between groups. Paired Samples test was used to compare for core and skin temperature in groups. P value of less than 0.05 was considered as statistically significant.
The patient characteristics of the groups did not differ except for the menstrual cycle days (Table 2). No significant differences were found mean arterial blood pressure, heart rate, operating room temperature between the two groups.
Table 2: Patient Characteristics. View Table 2
Initial core temperature was different in both groups. The core temperature decreased after the anesthesia induction and was different in both groups at all time intervals (Figure 1). Core temperature decreased significantly in both groups due to initial core temperature. In contrast there was no significant difference for skin temperature at all time intervals in both groups (Figure 1). Skin temperature increased at 15 and 30 minutes significantly in follicular group (P respectively 0.0001, 0.001). Skin temperature significantly increased at 15, 30 and 45 minutes in luteal group (P respectively 0.0001, 0.015, 0.011). The skin temperature differences from baseline were similar in both groups at 15-60 minutes (Figure 2). It significantly increased in luteal group compared to follicular group at 75 and 90 minutes (P respectively 0.095, 0.024). There was no significant difference between the two groups for shivering scores (P: 0.459) (Table 2).
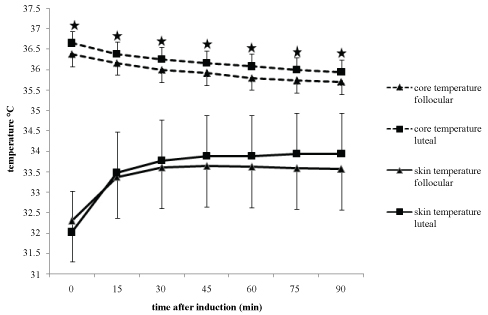 Figure 1: Core and skin temperatures change during anesthesia are shown. The core temperature of Luteal Group was significantly higher than that of Follicular Group at all times. *P < 0.05 compared with Follicular Group. Skin temperature increased at 15 and 30 minutes significantly in Follicular Group and significantly increased at 15, 30 and 45 minutes in Luteal Group. #P < 0.005 significant increases in groups.
View Figure 1
Figure 1: Core and skin temperatures change during anesthesia are shown. The core temperature of Luteal Group was significantly higher than that of Follicular Group at all times. *P < 0.05 compared with Follicular Group. Skin temperature increased at 15 and 30 minutes significantly in Follicular Group and significantly increased at 15, 30 and 45 minutes in Luteal Group. #P < 0.005 significant increases in groups.
View Figure 1
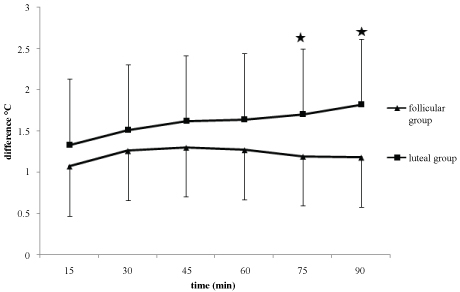 Figure 2: The skin temperature differences from baseline are shown in both groups. *P < 0.005 compared with Follicular Group.
View Figure 2
Figure 2: The skin temperature differences from baseline are shown in both groups. *P < 0.005 compared with Follicular Group.
View Figure 2
In this study we found that the core temperature was higher in luteal group and decreased significantly in both groups after anesthesia. The skin temperature significantly increased at 15 and 30 minutes in follicular group and at 15, 30, 45 minutes in luteal group after anesthesia. While in both groups the skin temperature differences were similar at 15-60 minutes, it significantly increased at 75-90 minutes in luteal group.
During a general anesthesia hypothermia occurs due to several mechanism like redistribution of heat, cool environment, loss of heat from surgical incisions e.g. Especially the redistribution of heat from core to the peripheral regions of the body by inhibition of tonic thermoregulatory vasoconstriction causes the core temperature decrease rapidly but skin temperature increase due to peripheral vasodilation after anesthesia [7].
It is widely known that sex steroids already cross the blood brain barrier and may effect on thermoregulation modulation in central nervous system. Especially in the brains of animals sex steroid receptors have significant action on thermosensitive neurons [8-10]. Warm sensitive neuron activity is inhibited by progesterone, thereupon body temperature increases under the influence of inhibited heat loss mechanisms [8]. On the other hand estrogen inhibits cold sensitive neuron activity and stimulates warm sensitive neurons therefore regulated body temperature decreases via activated heat loss mechanisms and inhibited heat retain mechanisms [9]. During the menstrual cycle hormonal pattern changes that may affect skin blood flow during exercise or heat stress [11]. For that reason cutaneous vasodilation threshold temperature and the onset of vasodilation were variable between follicular and luteal phases of the menstrual cycle [12-14]. In addition a study showed that women present with reduced α2-adrenergic vasoconstriction during exercise at 15% effort during the luteal phase compered with the follicular phase of menstrual cycle [15]. Body's thermostat is reset to higher temperature that increases cutaneous vasodilation and sweat rates during the luteal phase when progesterone level is high [16,17].
In our study we showed that different core temperatures were found for two menstrual cycle phases. Therefore decreased core temperature after anesthesia was different between groups. Although there was no statistically difference between two groups for skin temperature, the difference of skin temperature was significantly increased according to initial value at 75-90 minutes in luteal group. In addition the skin temperature increased at first 30 minutes in follicular group and at 45 minutes in luteal group. This may explain as peripheral blood flow differences in menstrual cycle phases. In women vasodilatory responses changed due to menstrual cycle phases. For example during exercise there was a lower α2-adrenergic vasoconstriction at luteal phase compared with follicular phase [15]. In contrast, during luteal phase resting sympathetic nerve activity has been shown to be higher [18]. These responses might be influenced by anesthesia which inhibit the tonic thermoregulatory vasoconstriction. The luteal phase of menstrual cycle may less inhibit the tonic thermoregulatory vasoconstriction during anesthesia.
Forearm blood flow measurement provides an index of skin blood flow that is important in the assessment of thermoregulatory effector function [19,20]. During luteal phase of menstrual cycle forearm blood flow could approximately be 50% higher [4]. By the way during general anesthesia skin blood flow and skin temperature increased. In this study, we used forearm temperature measurement method which is the limitation for assessment of the thermoregulation.
We assessed whether menstrual cycle phases alter thermoregulatory responses during anesthesia. Our results show that skin temperature differences are higher in luteal phase of menstrual cycle. Further studies are necessary to determine the exact mechanism of the thermoregulation during menstrual cycle phases under anesthesia.