Chronic postsurgical pain (CPSP) can be a devastating complication of surgery. Only recently has chronic postsurgical pain been included in International Classification of Disease with a separate code (MG30.21) [1].
Its prevalence is reaching up to 50-60% based on the literature (depending on surgery type). Regarding hernia surgery the estimated frequency of postsurgical moderate to severe pain is around 10-12%. Neuropathic pain prevalence is higher up to around 30%. If we take into account the number of hernia operations done we can understand the magnitude of the problem and the usefulness of treating these patients [2].
The dual nature of CPSP -both nociceptive and neuropathic- can cause confusion regarding comparisons of pain in the literature. Treating this condition can be complicated and difficult. There is a variety of modalities, ranging from medication in pain clinic, revision surgery or invasive procedures (neurolysis, nerve blocks). A feasible and reproducible solution seems to be ultrasound guided nerve block. Nerve blocks might work in multiple ways. First of all providing a temporary break of the vicious cycle of chronic pain development pathophysiology (sensitization, hyperalgesia and allodynia). Secondly, there have been reports in the literature regarding the beneficial effects of hydrodissection (the mechanical effect of injecting fluid around entrapped nerves and providing relief by reducing pressure). Hydrodissection seems advantageous compared to revision surgery since its much less invasive and more practical to be repeated. Also, injection of long acting steroids might prove to be of some benefit to inflamed nerves [3-5].
The nerves in the inguinal area that are usually involved in complications during herniorrhaphy are mainly three:
1. The iliohypogastric, (IHN)
2. Ilioinguinal (IIN) and
3. Genitofemoral (GFN)
The IHN is a mixed sensorimotor nerve and originates from the ventral ramus of L1 emerging from the upper lateral border of the psoas major.
The IIN is a mixed sensorimotor nerve arising from the first ventral lumbar ramus.
The GFN is a mixed sensorimotor nerve originating from the L1 and L2 ventral rami and forms within the psoas muscle [1].
The distribution of the abovementioned nerves (in the commonest distribution) in the inguinal area can be seen in (Figure 1).
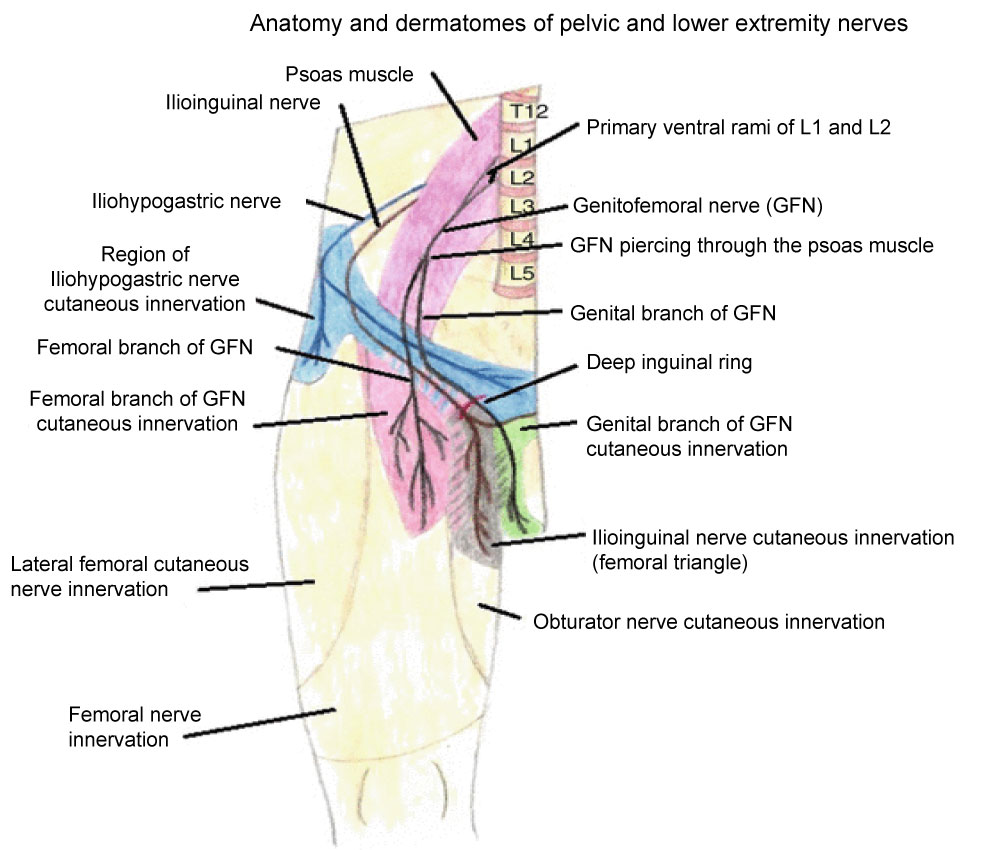 Figure 1: Innervation of inguinal area (commonest). View Figure 1
Figure 1: Innervation of inguinal area (commonest). View Figure 1
Neurolysis is an extreme solution to relieve pain intractable by other means like medication. Nowadays neurolysis is usually offered to terminally ill patients with intractable pain. Using neurolysis for intractable postsurgical pain in otherwise healthy patients remains unclear regarding benefit/risk ratio [6].
If finally a decision for neurolysis is taken, it should be preceded by a "diagnostic" ultrasound guided peripheral nerve block to specify the nerve branch causing the problem.
In the case we describe the patient was referred to anaesthesia department with request for neurolysis because of intractable pain after inguinal hernia repair. The pain was affecting his everyday activities.
We describe the case of a 48-year-old male patient who had undergone inguinal hernia repair 8 months ago. After multiple visits to the surgeon we received a referral to perform a neurolysis of the affected branches.
Discussing the case with the surgeon and the patient we explained the possible complications of a neurolysis and the smaller benefit/risk ratio in an otherwise healthy patient. After our suggestions and explanations patient and surgeon agreed to perform a "diagnostic and treating nerve block" to initially assess the pain origin and follow up with the patient for a period of 20 days before proceeding to more invasive measures.
Patient was an otherwise healthy adult, 106 kg body weight and 1.73 m height.
in order to have a more robust effect of hydrodissection and nerve block, we usually prefer to do individual nerve block. Due to his obesity and maybe because of preceded surgery, the localization of individual nerves was very poor.
Instead of aiming on separate branches block we decided to perform a TAP block which is known to cover the desired neurotomes. The plan was if-possible- to have a "hydrodissecting effect" by dilating the transverse abdominis plane, relieving possible entrapped nerves. To maximize our potentials, we decided to use a relatively large volume of injectate (40 ml). The mixture would include analgesic concentration of ropivacaine (0.2%) plus a potent steroid (dexamethasone) for its anti-inflammatory properties.
On the day of procedure patient was fasted for 6 h.
The initial pain score was checked and recorded using the numerical rating scale (NRS) with patient lying supine and during exercise effort to perform a "sit-up" The pain score was 2 on resting and going up to 6 during activity. We also applied the DN 4 questionnaire for neuropathic pain. Patient scored 5/10 in DN4 (positive for neuropathic pain). Sensory checking with cold test and pinprick showed an area of hypesthesia over the entire right inguinal area.
All standard monitoring as per ASA was applied and patient was given a mild sedation to remain calm and comfortable during the procedure. Aseptic technique was used. We scanned the subcostal area and decided the best plane where our landmarks (muscle layers/external-internal oblique and transverse abdominis) were identified easily.
We used a 100 mm 22 g needle, and in plane technique.
When the needle was in plane between internal oblique and transverse abdominis a total of 40 ml 0.2 ropivacaine (containing 4 mg dexamethasone as additive) were given with all precautions (small increments, US observation, injection pressure and frequent aspirations).
After the procedure, patient was kept for 2 h in recovery for post procedure observation.
Pain score was checked with NRS score every 15 min (time zero being time transferred to recovery).
The pain scores for the two hours in recovery can be seen below in Table 1.
Table 1: NRS pain scores post-procedure. View Table 1
A detailed physical examination with sensory testing (cold test/pinprick) and patient reporting revealed patient had pain relief on the majority of the inguinal area with a small area medially that was slightly painful (Figure 2).
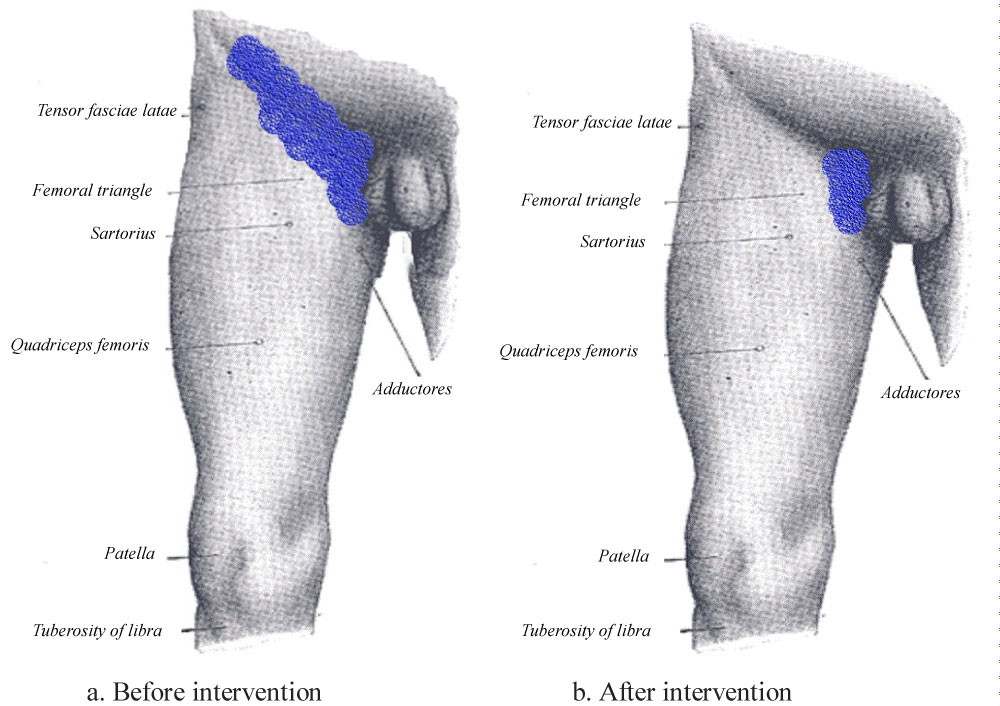 Figure 2: Patient self-reported pain area pre a) and post procedure; b) The reported as painful area is the "blue-colored" area. View Figure 2
Figure 2: Patient self-reported pain area pre a) and post procedure; b) The reported as painful area is the "blue-colored" area. View Figure 2
The patient was released home after 2 hours in recovery and informed about possible complications. He was given all communication details of the two anaesthetists who performed the block.
We informed the patient to communicate for feedback after every 5 days for 20 days. He was informed how to describe his symptoms in rest and activity before communication.
The patient communicated 3 times. He mentioned having relief at rest (NRS 0-1) and a NRS score of 2-3 on activity but limited to the medial part of the inguinal area. Unfortunately follow up was lost due to lack of further patient feedback.
In this case report the interesting part is we achieved a partial pain relief (only a small area probably innervated by the genitofemoral nerve did not respond).
The question in this case is if this effect of relief was due to a "hydrodissection" effect or the effect of dexamethasone (since duration of action of ropivacaine is much shorter than 15 days in which we had a relatively beneficial effect).
The biological half -life time of Dexamethasone is up to 72 h. This reflects the duration of influence on target tissues and roughly correlates with anti-inflammatory activity.
In this case report there are some possible benefits and advantages shown in treating patients with chronic postherniorraphy pain. The possibility of providing some pain relief with a relatively easy to perform block like the TAP block (individual nerve blocks may be troublesome to localize in obese patients), seems promising. Ofcourse there are details to be clarified like if this effect lasting for 15 days was due to the anti-inflammatory effect of dexamethasone on nerves or due to some kind of "hydrodissection effect" opening spaces of nerve entrapment of the inguinal area.
Our approach with the TAP block probably did not achieve blocking the genitofemoral completely. This conclusion is based on the persistence of residual pain (although decreased compared to baseline) in a small area of the medial inguinal area.
More research is necessary to evaluate the feasibility and effectiveness of a simple block like TAP block to treat patients with chronic postsurgical pain.
It is very important to clarify the possibility of achieving some pain relief of patients with post herniorrhaphy chronic pain, especially if this can be done with minimally invasive and easy to perform procedures like a TAP block. Ideally, we would aim for individual nerves. The localization of these nerves though can be challenging in cases of distorted anatomy due to surgery or obesity. Although in our case it is not clear if the analgesic effect is due to space opening ("hydrodissection effect") or due to anti-inflammatory effect of dexamethasone, the fact of patient pain relief is a positive outcome.