Background: Spontaneous intracranial hypotension (SIH) is uncommon and postulated to occur due to spontaneous cerebrospinal fluid (CSF) leak. Subdural hemorrhage is a rare but serious complication of intracranial hypotension. With a paucity of high-level evidence to guide treatment, its management remains challenging.
Case presentation: We report a case of spontaneous intracranial hypotension which was successfully treated with an epidural blood patch. The patient is a 59-year-old man with poorly controlled diabetes and hyperlipidemia who presented with left trochlear nerve palsy and bilateral acute subdural haemorrhage (SDH) secondary to SIH. He underwent bilateral burr hole drainage of acute SDH under general anaesthesia. Post-extubation, an epidural blood patch was performed which resulted in resolution of his symptoms.
Conclusion: We highlight an interesting case of SIH presenting atypically with cranial nerve IV palsy and its successful management with epidural blood patch.
Spontaneous intracranial hypotension, Epidural blood patch
Spontaneous intracranial hypotension (SIH) is an uncommon condition. The non-specificity and variety of the presenting symptoms often lead to delayed diagnosis and treatment of SIH.
Epidural blood patch (EBP) is the gold standard treatment for post-dural puncture headache where there is a known precipitant for cerebrospinal fluid (CSF) leak and the likely level of the dural hole is also known. However, the role of EBP is less clear in SIH where CSF leak occurs spontaneously without any precipitating factors with unknown location of CSF leak.
We describe a case of SIH presenting atypically with cranial nerve IV palsy and subsequent resolution of symptoms after burr hole drainage of bilateral subdural haematomas (SDH) and the administration of epidural blood patch.
Written informed consent for the use of images and details of the case for publication of this case was obtained from the patient.
A 59-year-old man with hyperlipidaemia and diabetes mellitus presented to the emergency department (ED) with headache and diplopia. He had been referred by his Primary Care Physician with concerns of a possible cerebrovascular event. Computed tomography (CT) of the brain was unremarkable. Magnetic resonance imaging (MRI) of the brain also did not reveal any acute infarct, intracranial hemorrhage or mass lesion. He was admitted and observed for 2 days. The headache improved with simple analgesics and the patient was discharged home with outpatient Neurology and Ophthalmology follow up.
Three weeks later the patient returned to the ED with non-vertiginous postural giddiness that was better on lying down and worse on sitting or standing. It was associated with an unsteady gait and 2 episodes of vomiting on the morning of admission. The headache and diplopia had also recurred. There was no history of head injury or loss of consciousness.
On this second presentation, clinical examination demonstrated diplopia that exacerbated with right gaze and left head tilt, consistent with worsening left trochlear nerve palsy. There were no other neurological deficits. CT-brain revealed bilateral subdural haematomas and mild obliteration of the suprasellar cistern with suggestion of sagging of the brain stem (Figure 1). Magnetic resonance imaging (MRI) of the brain showed bilateral holo hemispheric subdural haematomas (right 0.7 cm, left 1 cm) and sagging of the hypothalamus which raised the suspicion of intracranial hypotension. Diffuse pachymeningeal enhancement was seen (Figure 2). MRI whole spine was done. However, this failed to reveal any dural abnormality or extradural CSF fluid collection that would suggest a high flow CSF leak.
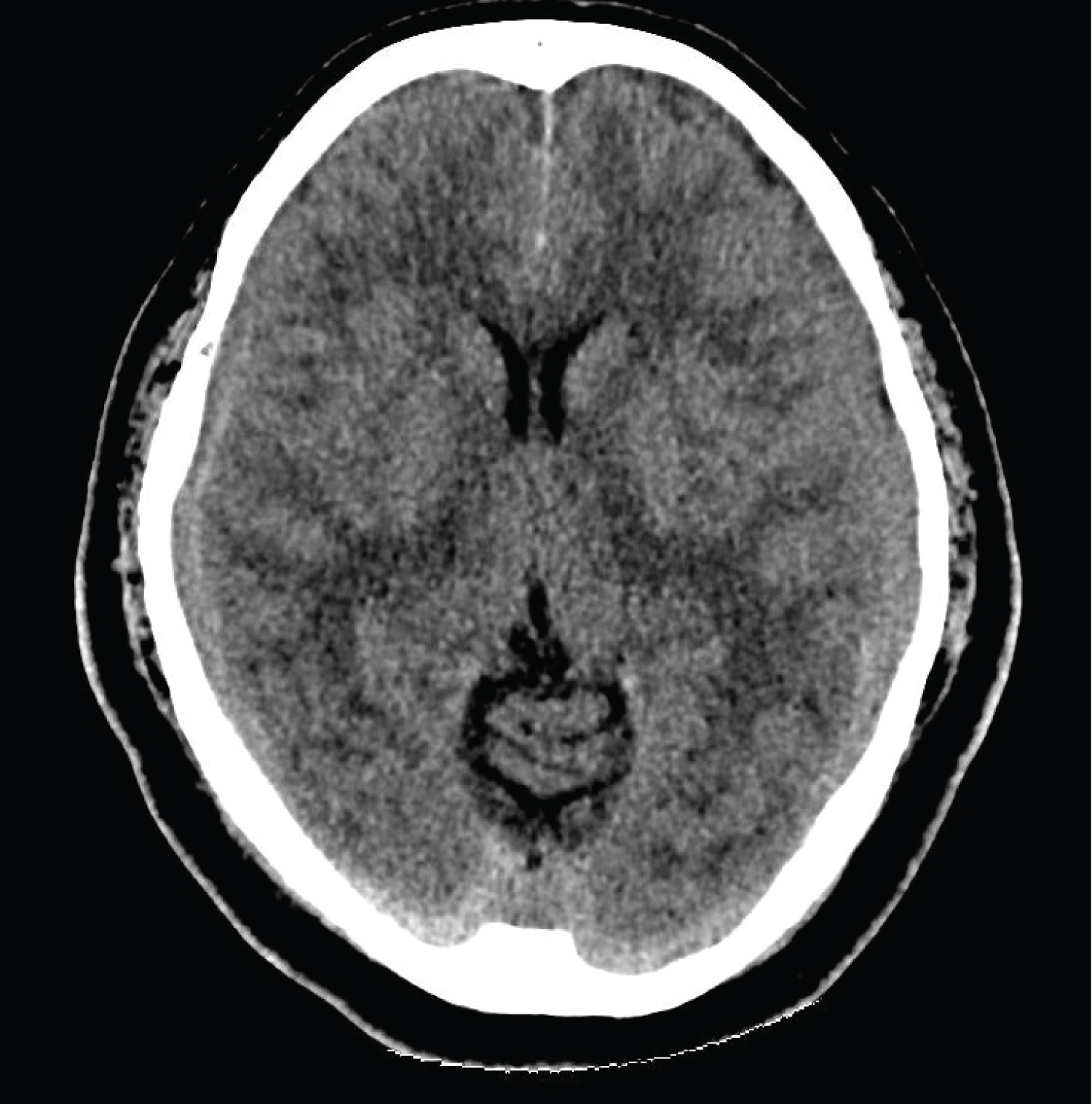 Figure 1: CT-brain: Axial image showing bilateral subdural haematomas.
View Figure 1
Figure 1: CT-brain: Axial image showing bilateral subdural haematomas.
View Figure 1
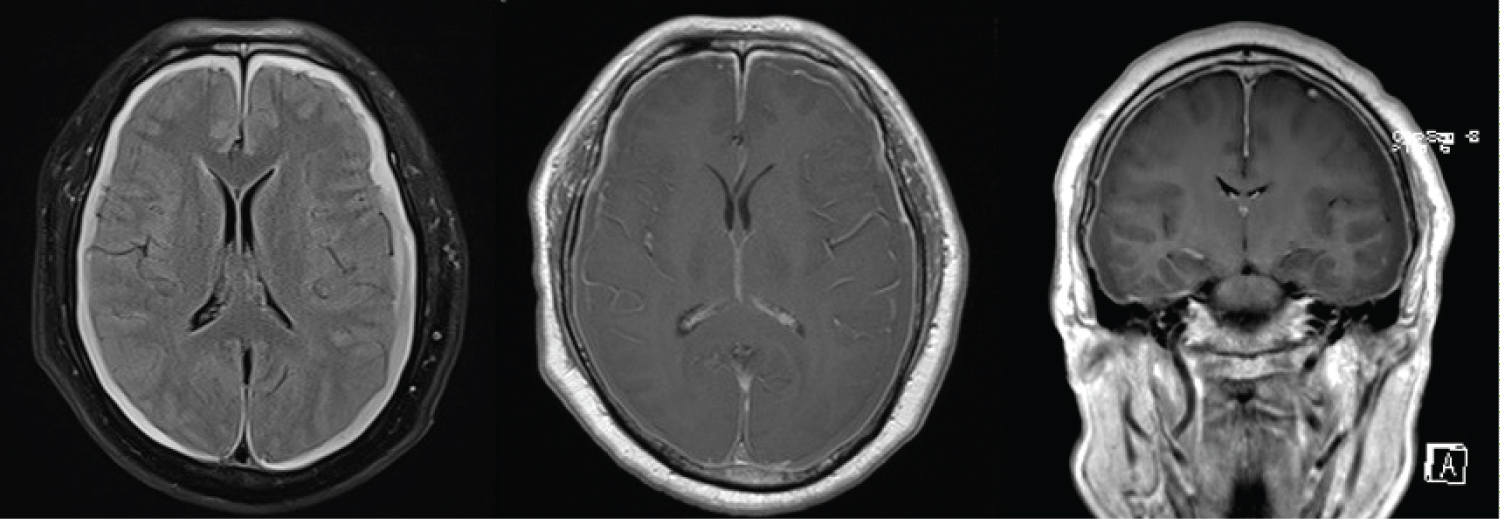 Figure 2: MRI-brain (A) Bilateral holohemispheric subdural haematomas; (B) Diffuse pachymeningeal enhancement; (C) Sagging of hypothalamus.
View Figure 2
Figure 2: MRI-brain (A) Bilateral holohemispheric subdural haematomas; (B) Diffuse pachymeningeal enhancement; (C) Sagging of hypothalamus.
View Figure 2
The clinical suspicion for spontaneous intracranial hypotension was high in view of the history of postural symptoms, focal neurological symptoms and bilateral SDH with a mildly sagging hypothalamus. Therefore, the patient was offered bilateral burr hole drainage of SDH under general anaesthesia and an awake epidural blood patch.
Burr hole craniotomy released dark red SDH under moderate pressure; the brain expanded quickly after drainage. He was extubated uneventfully and a detailed neurological examination was performed which did not show any new deficits. When fully awake, the patient was positioned in the right lateral position with right arm extended and placed on continuous monitoring. Both lumbar region and right antecubital fossa were prepared under aseptic technique. 20 ml of blood was withdrawn from the right basilic vein. Meanwhile, the lumbar L3/4 region was infiltrated with local anaesthesia (1% lignocaine 5 ml) and an 18G Tuohy needle was inserted until loss of resistance to saline was felt. The blood (20 ml) was then injected into the epidural space in 5 ml aliquots. Following the EBP the patient reported complete resolution of headache and tinnitus and some subjective improvement in diplopia.
The patient was monitored in the high dependency unit postoperatively where he remained stable. He was asked to lie flat in bed for 48 hours postoperatively. On the third postoperative day, he was allowed to sit up in bed. As the headache did not recur, he was subsequently encouraged to ambulate. On postoperative day 7, CT-brain showed satisfactory evacuation of bilateral SDH and the patient was discharged home on postoperative day 9.
During subsequent outpatient follow-up appointments, the patient did not experience recurrence of symptoms. The left trochlear nerve palsy gradually improved and was found to have resolved completely at follow-up 5 months post-EBP.
Spontaneous intracranial hypotension is an uncommon diagnosis with an incidence of approximately 5 in 100,000 persons [1]. This means that it is even more uncommon for Anaesthetists to see such patients as only a subset of patients will be referred for our expert opinion with a view for EBP. Hence, we report this interesting case so as to highlight the salient features of the diagnostic challenges as well as the controversial use of a "blind" epidural blood patch in the management of SIH with an unknown level of CSF leak.
Incidence, Postulated Pathogenesis and Variable Presentations Leading to Diagnostic Dilemmas SIH can be associated with hereditary connective tissue disorders (which may cause inherent weakness of the spinal dura), as well as calcified spinal discs or bone spurs that can tear the dura. There should be a significant absence of a history of dural puncture or other causes of CSF fistula. It is more common in women, and incidence usually peaks at around age 40 [1].
Spontaneous intracranial hypotension is believed to occur due to a CSF leak through a hole or tear in the spinal dura [2]. Patients with SIH most commonly present with orthostatic headache, nausea, vomiting, giddiness, tinnitus and cranial nerve palsies [3,4]. Cranial nerve palsies in SIH are thought to be caused by the low CSF volume. The loss of buoyancy and downward displacement brain structures applies traction to cranial nerves. Ophthalmoplegia due to cranial nerve palsies are most widely reported. In patients with SIH who present with diplopia, the most common cranial nerve palsies are unilateral CN VI, followed by bilateral CN VI, unilateral CN III and bilateral CN III palsies at 60%, 24%, 9% and 5% respectively [4]. However, there are only a few case reports which describe CN IV palsies related to SIH [2,5,6]. Thus, the non-specific presenting complaints often delay diagnosis and treatment of SIH.
As in the case of our patient, we postulate that the traction on the brain caused the characteristic positional headache, characteristically exacerbated by an upright position and relieved with a supine position. However, our patient's male gender and lack of a classical history presented a diagnostic conundrum. We wish to emphasize the need for a high degree of suspicion for variable presentations of SIH. In particular, his presentation of CN IV palsy is noteworthy and highlights the importance of keeping this unusual presentation in mind. Failure to recognise that CN IV palsies can be related to SIH can delay diagnosis resulting in adverse outcomes. In this case SIH was diagnosed 3 weeks after the initial onset of diplopia when the patient returned to hospital with worsening symptoms and was found to have developed bilateral subdural haematoma which is a rare but serious complication of SIH.
Confirmation of the diagnosis requires imaging evidence of a dural leak or low CSF pressure. This can most often be obtained by MRI or radioisotope cisternography. These imaging modalities may reveal the following features suggestive of low CSF pressure: Diffuse pachymeningeal enhancement, sagging of the brain, tonsillar descent, posterior fossa crowding and dilated cervical epidural veins [7].
The evidence for treatment options of SIH remain at the level of expert opinion and anecdotal experiences [7]. Management options include bed rest, adequate hydration, abdominal binders, oral caffeine, intravenous caffeine and more invasive options of epidural injections of saline, dextran or fibrin glue [8].
The injection of autologous blood into the lumbar epidural space was initially suggested in 1960 by Gormley, [9] and later introduced by Di Giovanni and Dunbar [10]. The mechanism of action is postulated to be similar: Injected blood creates a clot that seals the hole in the dura to prevent further CSF leak [11]. The volume of blood injected into the epidural space helps to increase CSF pressure while decreasing the downward traction on the brain and meningeal structures, thus alleviating symptoms [12].
An epidural blood patch has a high success rate of 70 to 90% in patients with post-dural puncture headaches where a precipitating trauma has led to a known hole in the dura [13,14]. However, the role of EBP is less clear in SIH where CSF leak occurs spontaneously without any precipitating factors with unknown location of CSF leak. The success rate of an EBP for patients with SIH is estimated at only 30% and this includes patients with a known level of CSF leak. Even so, some of these patients require repeat EBP up to six times for sustained relief [8].
Theoretically, knowing the level of CSF leak would allow a more targeted sealing of the CSF leak by the injected blood. Published literatures have advocated the use of CT-guided epidural blood patch to be performed at the level of the CSF leak [11]. However, there remains no consensus as to the level at which the EBP should be performed even if the level of CSF leak is known [12]. There are reports of administering a "blind" EBP without a known level of CSF leak [8].
In our patient, no dural abnormality could be identified by MRI-whole spine. There were differing opinions amongst the Senior Anaesthesia Consultants as to the appropriateness of performing an EBP for our particular patient. Reasons against performing an EBP included- a lack of evidence of dural abnormality, an unknown level of dural abnormality if this existed a relatively low success rate of the procedure and possible need for repeat procedures, as well as the risk of further dural puncture with the procedure. However, upon joint discussion with the Neurosurgical Team and the patient, decision was made to offer an EBP performed awake after the burr hole drainage of the bilateral SDH. Our decision was made due to the severity of the patient's condition and the low level of evidence for management options of SIH. With the patient awake we could assess his neurological functions post-burr hole drainage of bilateral SDH and document any changes in baseline neurology. We performed the "blind" EBP at the lumbar region due to the familiarity of lumbar epidurals to us as Anaesthetists and the wider margin of safety.
We describe a good outcome following EBP for a patient with SIH whose diagnosis had been delayed by his atypical presentation with trochlear nerve palsy. It was only after further imaging demonstrated findings suggestive of SIH that the patient received appropriate treatment. It is therefore important to have high level of suspicion for SIH in patients with an orthostatic headache and unexplained cranial nerve palsies. Our case has also demonstrated that EBP can be effective even if the exact location of the CSF leak is unknown. Further studies are required to evaluate the efficacy of the different management options of SIH.
No potential conflict of interest relevant to this article was reported.
Li Weiling Lydia (Conceptualization; Writing-original draft; Writing-review & editing); Lim Yiqi Ofelia (Writing-original draft); Chan Lijuan Jasmine (Writing-review & editing); Alex Joseph (Supervision; Writing-review & editing).