Objective: This study aimed to estimate the incidence rate and determine the possible associated factors for postoperative sore throat following surgery conducted under general anesthesia using endotracheal intubation.
Methods: Hospital-based prospective observational study design was conducted from June to September 2018 in the referral hospitals in Asmara. The study was conducted at the Ear Nose Throat, Obstetrics and Gynecology and General Surgery departments of Orotta National Referral and Teaching Hospital and the Orthopedic, Burn and General Surgery departments Halibet National Referral Hospital. Data was collected using a structured questionnaire. Data analysis was done using SPSS version 22. Descriptive results were summarized in frequencies and percentages using tables and graphs. Moreover, a modified logistic regression was used to estimate the adjusted relative risk instead of the ordinary logistic regression in order to find out the magnitude and direction of association of postoperative sore throat and the independent variables.
Results: Out of the 336 participants who underwent surgery under general anesthesia using endotracheal intubation, one hundred and three patients (30.7%) have developed postoperative sore throat. Body weight of more than 70Kg (ARR = 2.543, 95% CI: 1.13 - 5.75, p-value: 0.025) and multiple intubation attempts (ARR = 2.19, 95% CI: 1.20- 4.00, p-value: 0.01) were the sole factors influencing the occurrence of POST.
Conclusions: The incidence of postoperative sore throat was found to be high in the national referral hospitals in Asmara. Number of intubation attempts and body weight of the participants were identified as the main risk factors. Reduction of multiple trials during tracheal intubation might help in the reduction of postoperative sore throat.
Sore throat, Risk factors, Tracheal intubation
ACHS: Asmara college of health sciences; AOR: Adjusted Odds Ratio; ARR: Adjusted Relative Risk; ASA: American Society of Anesthesiology; BMI: Body Mass Index; CI: Confidence Interval; Cm: Cent-meter; ENT: Ear Nose Throat; ETI: Endotracheal Tube Intubation; ETT: Endotracheal Tube; GA: General Anesthesia; GVL: Glide Scope video-laryngoscope; IQR: Inter Quartile Range; LMA: Laryngeal Mask Airway; M: mean; Mm: Mill -Meter; NGT: Naso-gastric Tube; OR: Odds Ratio; POST: Postoperative Sore Throat; PVC: polyvinylchloride; RR: Relative Risk; SA: Spinal Anesthesia; SPSS: Statistics Package for Social Sciences
Postoperative sore throat (POST) has been a known complication after general anesthesia using endotracheal intubation (ETI) [1]. Causing dissatisfaction and discomfort, POST has been rated by patients as the eighth-most adverse effect during the postoperative period [2]. It is a common problem following the use of ETI during general anesthesia (GA) [3]. Despite the improvement in anesthesiology, POST following ETI remains a concern [4]. Even though the causation of POST is unknown, the etiology is multifactorial, including patient-related factors such as age [5], sex [6-12], smoking [6,13] , and intubation factors, including duration [1,14,15], tube size [1], type of laryngoscope used [14,16], cuff pressure, [4,17] and multiple intubation trials [1,8]. POST increases analgesic use and other health care costs [18]. Despite its disadvantage in triggering POST, utilization of endotracheal intubation (ETI) during general surgery becomes inevitable as it protects the lungs from aspiration and leakage of air during mechanical ventilation. In Eritrea, published research on this topic is extremely scarce. So the incidence of POST is not known in the country. Knowing the incidence of POST and its influencing factors in our situation helps recognize the magnitude of the problem and initiate actions to reduce its occurrence. This research can also help as a background for future research on the related topics by indicating the incidence rate and associated risk factors of POST. This study aimed to assess the prevalence and factors related to POST among patients who were operated under general anesthesia with endotracheal intubation in the referral hospitals in Asmara.
A prospective observational study design was utilized from June 2018 through September 2018 in national referral hospitals in Asmara. The study was conducted at the Ear Nose Throat (ENT), Obstetrics and Gynecology and General Surgery departments of Orotta National Referral and Teaching Hospital situated at the centre of the capital city of Asmara and the orthopedic, burn (skin graft), and general surgery departments of Halibet National Referral Hospital situated at the periphery of the capital city. These are the two main national referral hospitals owned by the government where the majority of surgical procedures in the country are conducted.
All adult patients, who visited the selected hospitals during the study period (from June 1st 2018 to September 30th 2018) for surgical intervention under general anesthesia using endotracheal intubation technique, were the study population. All patients who visited the hospitals fulfilling the inclusion criteria were taken as participants in this study. All patients aged 18 years and above who underwent surgeries under general anesthesia using endotracheal intubation technique, with ASA classification of two and less than two, were included in the study. The exclusion criteria for participation were when patients were unwilling to participate, unable to communicate due to critical illness (Comatose, semiconscious, etc…), with an acute upper respiratory infection or with a sore throat before, underwent oro-laryngeal surgery, pregnant mothers and those with a history of psychiatric disorder and currently receiving psychological treatment or sedative, antidepressant, or antianxiety medications (Figure 1).
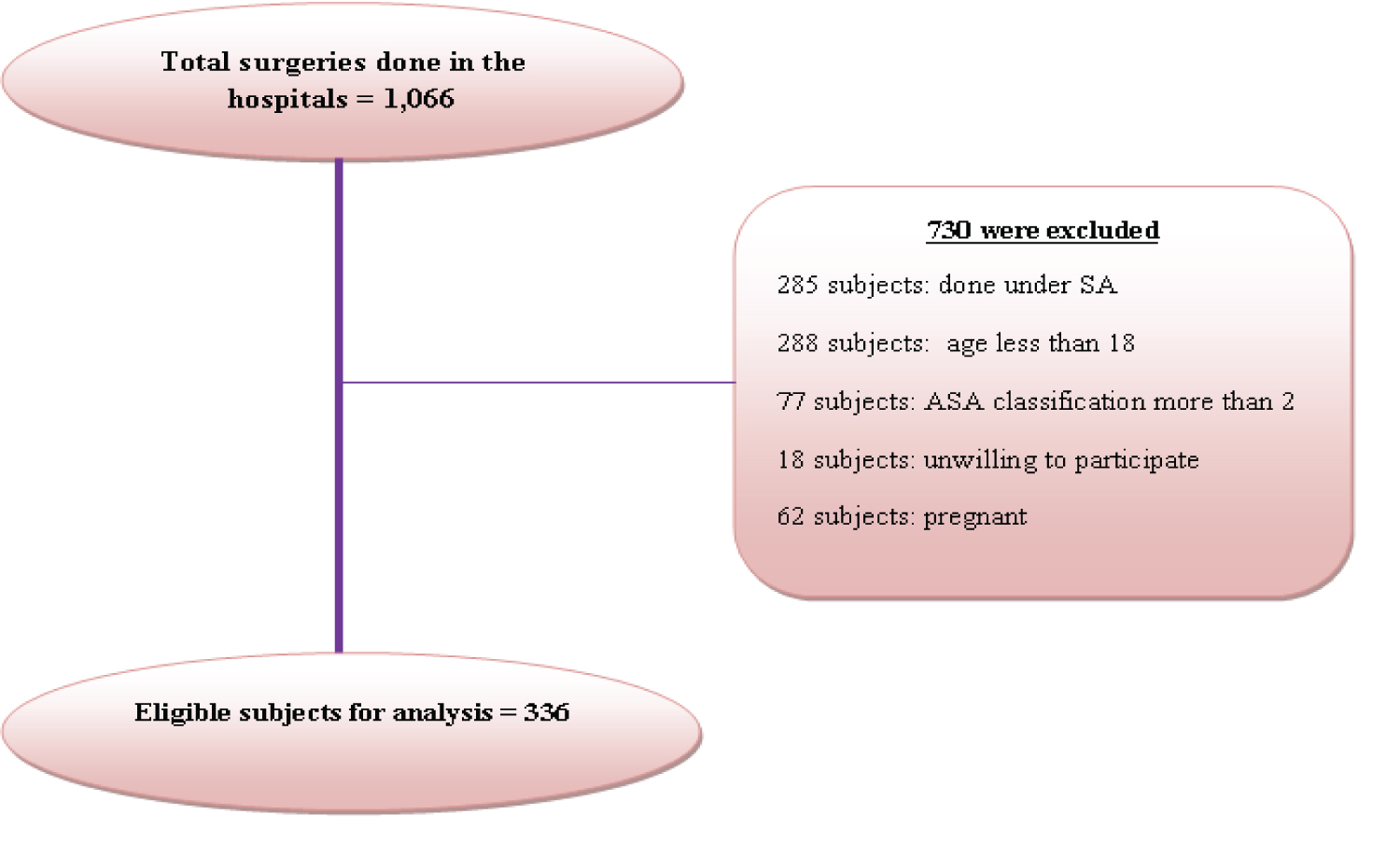 Figure 1: Participants' enrollment process.
View Figure 1
Figure 1: Participants' enrollment process.
View Figure 1
The dependent variable was a postoperative sore throat. The independent variables included: socio-demographic characteristics (age, sex, smoking status, BMI, body weight and height), the experience of anesthetist in charge, anesthetic techniques (type of muscle relaxant and analgesic used, ETT size and type, type of laryngoscope and size of blade, use of airways, use of lubricant for ETT, intubation attempts, insertion of throat pack, insertion of NGT, blood on ETT and duration of intubation time), type of surgeries (obstetric, gynecological, orthopedic, breast, thyroid, abdominal, nasal and ear problems etc…), and position of the patient during surgery.
Data collection was done using a pretested structured questionnaire covering five main portions: background characteristics, the experience of anesthetist in charge, anesthetic techniques, type of surgery and position of the patient during surgery. The face and content validity of the questionnaire was assessed by a team of experts in the profession. Before the main study was conducted, the questionnaire was tested on 20 participants at Sembel Polyclinic (a private hospital located Southwest of the city) to assess its language clarity, flow, consistency and readability. The dependent variable i.e. development of POST was assessed clinically using ‘yes' or ‘no' responses. During the pilot study, four responses were used to assess POST, however, it was difficult to differentiate the responses clearly. Hence, only two responses, ‘yes' or ‘no' were used i.e. patients who were clinically diagnosed with POST at the post-operative ward were coded as ‘yes' for POST development. The data collection procedure was conducted through direct face to face interviews with those participants who consented to participate. All patients were followed starting from the preoperative period until 24 hours after surgery to develop POST by the nurse anesthetists assigned at the respective hospitals.
After data collection was completed, questionnaires were checked for their completeness and consistency; and the variables of interest were coded and entered into SPSS (statistics package for social sciences, Version 22). The entered data was cleaned to look over the accuracy, consistency, and avoidance of missed values during entry. Data were presented using tables and graphs. Furthermore, mean (Standard Deviation) and median (Inter Quartile Range) was utilized to summarize continuous variables as appropriate after checking normality. Relative risks (95% CI) of the POST by various demographic and clinical variables were computed at bivariate level. Variables that were significant at bivariate level were further used for multivariate analysis using logistic regression. Multivariate logistic regression was used to find out the magnitude and direction of association of POST and various categories of the predictor variables after controlling the effect of background information. Adjusted Relative Risk (95% CI) was presented and p-values less than 0.05 were considered as statistically significant during the analysis. There is no currently available statistical tool that enables to compute adjusted relative risk. Hence, a modification of the logistic regression in SPSS was highly recommended to approximate the relative risk.
A modification of the logistic regression for estimation of adjusted relative risk was proposed by Diaz–Quijano [19].
Briefly, the modification was done to address the overestimation of the odds ratio for relative risk. Hence, the comparison of cases and non-cases in logistic regression was replaced by comparing cases and cases plus non-cases in the modified one, binomial regression. In a binomial regression model with k covariates, the function is written as: Log [a/ (a+b)] = ß0 + ß1X1+……ßixi . Where a, is the number of cases and b is the number of non-cases, and X the covariates. Thus, a/ (a + b) is the probability of success (e. g., the proportion of POST in a group), and the ARR (or APR) estimated of a given covariate Xi is eβi. On the other hand, in a logistic regression model, the function is written as: Log (a/b) = ß0 + ß1X1+ ... + ßkXk. Where a/b is the odds of success and the OR estimated of a given covariate Xi is eβi.
Out of the 336 participants, almost half (49.7%) of them were aged 18 to 40 years, whereas 30.7% were in the age group of 41 to 60 and the remaining 19.6% had an age of ≥ 61 years. Median age of the study participants was 41.5 years (IQR=29), and more than half (56.3%) of them were females. The average height and weight of the participants were 162 centimeters (SD ± 8.4) and 56.3 kg (SD ± 9.6), respectively. Three-fourths (75%) of the study participants had normal range of body mass index (BMI). About 5% of the participants were smokers. The majority (87.5%) of the participants were intubated by anesthetists in charge, with 43% of them undergoing abdominal surgery (Table 1).
Table 1: Socio-demographic characteristics of the study participants, anesthetist experience, position and type of surgery (n=336). View Table 1
The commonly used muscle relaxant for intubation was succinylcholine (69.9%), and the majority (85.4%) of the participants were given fentanyl as analgesics. Almost half (50.6%) of the participants were intubated using Glide Scope video laryngoscope, and around 12% of the participants were observed to have multiple intubation trials (Table 2).
Table 2: Procedures related to intraoperative anesthetic techniques: analgesics, relaxants, type of laryngoscope and ETT used (n=336). View Table 2
Around eleven percent of the participants who underwent surgery had nasogastric tube insertion. The majority (89.6%) of the participants were intubated using cuffed PVC, with a tube size of 6.5 mm being used in the majority (40%) of the participants. The period from intubation to extubation for the majority (61%) of the participants was between 40-69 minutes with a median time of 60 minutes. During extubation, blood on ETT was observed in 11% of the participants (Table 3).
Table 3: Procedures related to intubation and extubation techniques (n=336). View Table 3
The Incidence of Post-Operative Sore Throat (POST) was found to be 30.7% and its duration of stay was ≤ 4 hours for 70.9% of the study participants, followed by 5 - 9 hours for 27.2% and ≥ 10 hours for 1.9% (Figure 2).
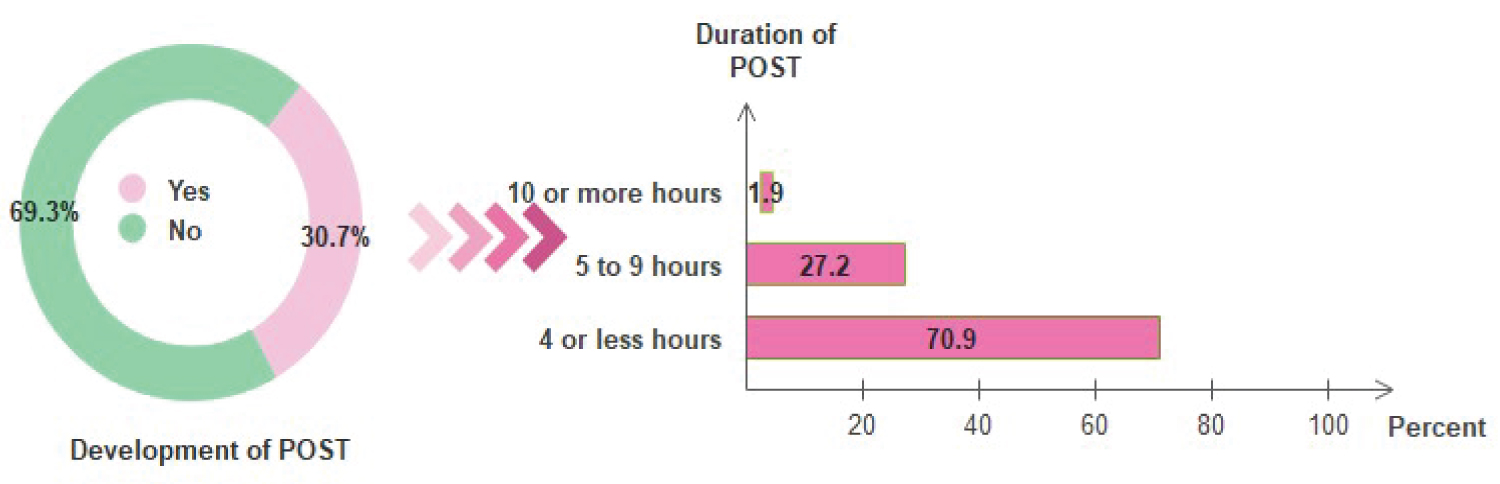 Figure 2: Percentage distribution of the participants who developed POST with the duration for which POST stayed, Asmara, Eritrea, 2018 (n=336).
View Figure 2
Figure 2: Percentage distribution of the participants who developed POST with the duration for which POST stayed, Asmara, Eritrea, 2018 (n=336).
View Figure 2
Patient-related factors: The risk of POST was compared across different categories of demographic characteristics. The risk of developing POST was not significant across age groups, sex, height, and BMI However, the incidence among overweight (42%) patients was relatively higher than those in normal (29%) range of BMI.
Participants with more than 70 kg were almost three times more likely to develop POST (RR=2.78, 95% CI: 2.05-3.76). Likewise, smokers were 2.15 times more at risk for developing POST than non-smokers (RR=2.15, 95%CI: 1.42-3.26). Patients undergoing Thyroid (45.5%) and ENT (34.6%) surgeries had the highest incidence of POST though no significant association was found between types of surgeries. The results revealed no significant risk of POST with respect to the person in charge of intubation or the years of experience of the anesthetist (Table 4).
Table 4: Bivariate analysis of socio-demographic characteristics of the patients, person in charge of intubation, anesthetist experience and POST (n=336). View Table 4
Factors related to intraoperative anesthetic techniques and procedures: The study found a statistically significant association between the development of POST and intubation trial of two or more (RR=2.30, 95% CI: 1.69-3.14). No significant occurrence of POST was shown across muscle relaxants used, types of analgesics, type of laryngoscope and blade of different sizes, NGT use, size and type of Endotracheal tube, lubricant or gel use and oral airway insertion. The incidence of POST was observed to be significantly higher (55.6 %) for those patients who have been stayed for more than 100 minutes of intubation (RR: 2.22, 95% CI: 1.08-4.59, p-value of < 0.05). The presence of blood on ETT during intubation was observed in (62.2%) of the patients who developed POST, and a statistically significant association was found at a p-value < 0.001 (RR=2.32, 95% CI: 1.70 - 3.18). Table 5 illustrates the remaining variables.
Table 5: Bivariate analysis of intraoperative anesthetic techniques and procedures and POST (n=336). View Table 5
Variables that were significantly associated with the incidence of POST at the bivariate level were analyzed further using multivariate analysis to find the adjusted relative risk. The risk of POST occurrence was found to have a statistically significant association with body weight (p=0.025) and a number of intubation trials (p=0.011). However, the remaining variables which have shown significance at the bivariate level had no more significant association after adjusting the confounding factors (Table 6).
Table 6: Multivariate results of relative risk adjusted for confounding effect (n=336). View Table 6
In the current study, the incidence of postoperative sore throat (POST) was found to be 30.7%. The incidence was lower than studies conducted in low-middle income countries [1,15,20]. On the other hand, the incidence was found to be higher compared to studies from developed countries [21,22]. Most of the studies compared showed that the incidence of POST was a common problem in patients who undergo surgery using tracheal intubation [5,21,22]. Yet, the incidence was found to be significantly low with the practice of LMA compared to ETI. Nevertheless, ETI is the commonly practiced procedure for intubation in the study setting. Given the results of the existing studies, the institution of LMA practice in the study area is highly recommended.
The majority of the participants were in the age range of 18 to 60 years. Though statistical significance was not found between age and sex as risk factors for POST, as the age of the participants' increases the incidence was observed to increase and it was higher in females than males. Similar studies reported a higher incidence of POST among females [1,6-12]. A higher incidence of POST was documented among older age groups in a study conducted in Pakistan [5]. The higher incidence among females might be due to the narrowness of the female tracheal tract. Likewise, the increased incidence of POST in older patients could possibly be due to the narrowing and kinking of the trachea related to geriatric physiologic changes. About three-fourths of the participants had a BMI within the normal range, nevertheless, the incidence of POST was observed to increase from those with severe malnutrition to those with overweight. Those participants who had a bodyweight of more than 70 kg had a significantly higher incidence. Studies conducted in other countries also revealed a positive correlation between POST and body weight [11,22,23]. The higher incidence of POST among patients with higher body weight might be due to the possibility of difficult intubation related to the limited head tilting during intubation resulting in multiple intubation attempts.
Smoking increased the likelihood of POST studies conducted elsewhere [6,13]. Similarly, our findings indicate a higher incidence of POST among smokers compared to non-smokers. The possible reason for this could be the fact that smoking and tobacco sniffing have the tendency to irritate of the oral cavity, organs of the respiratory and cardiac system. The majority of the study participants were anaesthetized by the anesthetist in charge. Among the study participants who were identified to be intubated by students, two-fifth of them developed POST. The findings of our study is inconsistent with another study that reported a similar incidence of POST in those patients who were intubated by trainees and consultant anesthetists [24]. The findings in our study can be attributed to the minor complications that can happen during the training time.
Though significant association was not observed, the incidence of POST was observed to be higher for those participants where vecuronium was used as a muscle relaxant during intubation. The difference in using analgesics didn't show any association with POST development. Type of laryngoscope and size of blade was found to have no significant association with the development of POST; however, the incidence of POST was higher in those participants who were intubated using GVL compared to Macintosh. Participants intubated with laryngoscope blade number 4 had a higher incidence than those intubated with blade size no 3. Inconsistently, studies conducted in Saudi Arabia, Iran and Ethiopia indicated a higher incidence of POST among patients intubated with Macintosh compared to GVL [1,14,16].
A significant association was seen between multiple intubation trials and POST development. Similar studies conducted in other countries reported a significantly higher incidence of POST among those patients intubated more than two times [1,8]. The reason can be defined due to the repeated trauma affecting the oro-laryngeal area related to multiple manipulations. In this study, the use of a nasogastric tube (NG), type and size of ETT, use of lubricant, and oral airway insertion were found to have no significant association with POST, however, some studies documented a significant association between NG and the occurrence of POST [1].
Post-operative sore throat has been found to develop in participants who underwent surgery using ETT with excessive cuff pressure [4,17]. In the setting where the study was conducted, there were only two types of cuffed ETT (Poly vinyl chloride and spiral), and the air was inflated to the balloon until air leakage was not heard or by checking the filling of an external balloon (pilot balloon); therefore, the comparability between the pressure on the tracheal wall created due to the amount of air in the balloon was very difficult as it was done manually instead of using the standard manometer (due to unavailability). Using such a method, a third of those with cuffed polyvinylchloride (PVC) and a fifth with cuffed spiral was found to develop POST, indicating the difference between the spiral and PVC ETT. This difference might be due to either the flexibility of the cuffed spiral or the hardness of the cuffed polyvinylchloride. The study findings indicated that the presence of blood on ETT or suction tube, and prolonged intubation time were found to have marginal significance in the development of POST. These results have consistency with other studies that reported bloodstain on the endotracheal tube as a risk factor for POST [6]. Patients with surgical procedures with a longer duration of time were found to develop POST more likely than those with short duration surgeries [1,14,15]. If a patient stays intubated for a long time, the risk of irritation and trauma of the oro-laryngeal and tracheal area is high; this might be the main cause of the development of POST.
This study had several limitations. Firstly, cuff pressure was not measured (due to the unavailability of a manometer); for this reason, the impact of cuff pressure in the development of POST was not assessed. Secondly, various types of surgical procedures (like ENT surgery) were included; this might affect the study results. Thirdly, a binary scale of ‘yes' or ‘no' responses was used to assess POST. The utilization of four-point scale was difficult to be measured during the pilot study. Despite these limitations, the current study attempted to quantify the incidence of POST and the impact of possible socio-demographic and clinical variables. The study also adds the following: POST studies in Eritrea are limited; thus, the current study will be used as a reference for future studies. The findings open room for developing a prevention strategy as the possible predicting factors are identified.
The incidence of postoperative sore throat was high at the national referral hospitals of Asmara that provided surgery services. The number of intubation attempts and the body weight of the participants were identified as the main risk factors. Reduction of multiple trials during tracheal intubation might help reduce postoperative sore throat.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
An official letter of support from Asmara College of Health Sciences was sent to the Ministry of Health Research and Ethical Committee and Health Facility Management Division, for obtaining a formal research study approval paper that was submitted to the medical directors of the selected hospitals and departments for conducting data collection at the selected National Referral Hospitals. Ethical issue for the study participants was highly respected. A thorough explanation of the study aim and potential benefits of patients in the study were stated, written consent paper was obtained for every participant who underwent surgery, in case he/she didn't agree, the participant was free to resign from the study at any part of the questionnaire. Anonymity and confidentiality were ensured in that the participant name will not appear on the questionnaire, and information will not be shared. During the study period, those patients who developed POST were given the appropriate treatment for relieving their complaint.
Not applicable.
The authors declare that they have no conflicts of interest.
No funding.
YMG, was responsible for study conception; data acquisition, and manuscript drafting. GGB, was advising, supervising and critically reviewed the study. EHT, was the study statistician conducted data analysis and interpretation. IMI, was responsible for data interpretation, manuscript drafting and critical revision. All authors revised and approved the manuscript for publication.
The authors thank all data collectors, encoders and study participants for their invaluable cooperation.