Background: The prevalence of geriatric surgery is rapidly increasing and, concomitantly, the procedure of anesthesia in the aging population. As a result, the goal of this research was to compare the efficacy of various anesthetic methods used in an ambulatory elderly population.
Methods: Retrospect chart study of 150 patients scheduled for procedures in a day surgical center using various anesthetic techniques. The cases were classified into three groups, and each anesthesia method had a total of 50 patients, that is, general anesthesia with endotracheal intubation (ETT) and general anesthesia with laryngeal mask airway (LMA), and spinal anesthesia (SA). The primary outcome was the discharge time from the post-anesthesia care unit (PACU), the secondary outcomes included perioperative hemodynamics, analgesia usage, the Aldrete Score, the incidence of postoperative nausea and vomiting (PONV), and other complications.
Results: The maximum fluctuation rate of the three groups' heart, systolic and diastolic blood pressures differed significantly. LMA < ETT < SA: P < 0.001. The mean duration of anesthesia among groups was significantly shorter, medium to long in SA (98.16 min) < LMA (106.78 min) < ETT (165.92 min): P < 0.001. Analgesic usage differed significantly from 24% in SA < 30% in LMA < 74% in ETT: P < 0.001. In the Aldrete scoring system among groups, the mean value differed significantly from 8 in SA > 6 in LMA > 5 in ETT: P < 0.001. SA (23.52 min), LMA (24.80 min), and ETT (54.60 min) had significantly shorter, medium, and longer mean times to discharge from PACU: P < 0.001, and no other complications were recorded except four, 8% cases of PONV only in SA: P = 0.016.
Conclusions: In the absence of contraindications, this research recommends using general anesthesia with a laryngeal mask airway for elderly patients having surgery in a day surgery facility.
Day surgery center, Elderly patients, Endotracheal intubation, Geriatric anesthesia, Laryngeal mask airway, Spinal anesthesia
The rate of population aging in many countries is much greater than has been the case in the past. For example, the population older than 60 years will double by 2050 in China and some other regions, as reported by the WHO [1]. Today, more than half of all in-patients undergoing surgery are above 60 years of age in most western countries. This trend will likely increase significantly within the following decades [2]. Surgical services increase as a country's population ages; anesthesia for elderly patients requires more excellent specific knowledge and skills.
Patients and society will benefit greatly from strategies to optimize anesthetic care, reduce complications and enhance outcomes in elderly surgical patients [3].
Patients always expect a low risk of anesthesia, minimum discomfort, and quick recovery and discharge; in this context, it is essential to consider optimal anesthesiologic care for elderly patients.
The decision to use spinal or general anesthetic is based on the surgical method, the anesthetist's and surgeon's ability, the patient's medical status (age, comorbidities, etc.), and other variables such as anxiety and the dread of not waking up, etc. [4,5].
The number of surgeries performed each year grows, with most of them being outpatient procedures. As anesthesiologists, we are continually looking for innovative ways to deliver effective anesthetic care, which is safe, pain-controlling permits patients to be released home promptly according to post-anesthesia care unit policy, and is easily repeatable. The usage of spinal anesthesia in the outpatient surgical approach has been proposed [6].
As we know, the choice of anesthetic methods is made between general and regional anesthesia. However, it is unidentified which one has the advantage over the other for geriatric patients in a day surgery center.
Only careful selection of patients and operations, adequate intra- and postoperative anesthetic management, and early discharge of patients without affecting the quality of patient care can ensure the safe and timely delivery of ambulatory surgical care [7].
Our monocentric retrospective study aimed to clarify and remove the confusion about which anesthesia method is to be used in a daycare center. Comparing outcomes of procedures performed in a geriatric population under general anesthesia represented by general anesthesia with laryngeal mask airways and general anesthesia with endotracheal intubation versus regional anesthesia represented by spinal anesthesia in a day surgery center.
The study was approved by the ethical committee of the institution: LDYYLL-2022-356.
The sample size represented by n was calculated using the following formula where z is a score for a 95% confidence level, p̂ is the population proportion 10.1, and ε is the margin of error of 5%.
From April 2021 to January 2022, 159 elderly patients underwent surgeries in the day surgery center of the first hospital of Lanzhou University. Among all patients who underwent procedures, 10.1% represented the aged population over 70-years-old and above. The type of surgical procedures was various 55% of them were urologic surgeries, 38% were orthopedics, and 7% represented other diagnostics. One hundred and fifty patients were analyzed in this retrospective cohort study.
We included men and women with the grade ASA (American Society of Anesthesiologists) ranging from I to III, aged 70 years or older, and ≥ 6 hours of preoperative fasting before surgery.
Patients with the conditions listed below were excluded from the study: emergency case, cognitive impairment, operation time > 4h, and patients who bypassed the PACU (Figure 1).
 Figure 1: Flowchart illustrating the assessed population.
View Figure 1
Figure 1: Flowchart illustrating the assessed population.
View Figure 1
The patients were paired by age, gender, weight, and ASA, then received general anesthesia with ETT (n = 50), general anesthesia with LMA (n = 50), and spinal anesthesia (n = 50). All of the patients fasted for at least 6 hours before surgery. Anesthesiologists with considerable experience from the same center performed all anesthetic protocols.
Monitoring was placed to control and identify the changes between baseline and perioperative hemodynamics; during the process, the patient's heartbeat, blood pressure, and oxygen saturation in the blood were all checked. In some cases, invasive monitoring was placed. A large functioning intravenous line was placed for infusion and drugs.
During preoxygenation, dexmedetomidine and penehyclidine were injected, followed by dexamethasone. Sufentanil 10-25 μg/kg and propofol 1.5-2 mg/kg or etomidate 0.1-0.3 mg/kg were used for induction. Cisatracurium 0.15-0.2 mg/kg was used before the management of the airway; whether an endotracheal tube or laryngeal mask was inserted, the fresh gas total flow of 2-3 l/min of air-oxygen mixture with a varying inspired fraction of oxygen between 45 to 60%, then anesthesia syringe pump with remifentanil 0.1 μg/kg.min and propofol 1-3 mg/kg.h on it, was used in association or not with sevoflurane 0.5-1% the inhaled anesthetic to maintain the anesthesia. Controlled mechanical ventilation was stopped, then the extubation followed if the patient was fully awaked; otherwise, patients were discharged to PACU before the extubation. Postoperative analgesics were used when skin closure began.
The patient was lying in lateral decubitus during the spinal anesthetic puncture. An intradermic infiltration of local anesthesia using 2% lidocaine was injected at the proposed puncture site. 0.5% or 0.75% of bupivacaine in 10% dextrose solution was released into the subarachnoid area across the intervertebral space L2-L3. Atropine, dopamine and norepinephrine, and dexmedetomidine were preferred to control the variation of hemodynamic parameters; oxygen 2l to 3l per minute was open to supply respiration and enhance blood saturation. Plus, as the duration of anesthesia was prolonged and an opioid was administered, more dezocine was used.
Patient information was obtained from a hospital database, where intraoperative heart rate and systolic and diastolic blood pressures were recorded. The maximum variation rate, obtained using the calculation: Maximum variation rate = (maximum-minimum)/pre-anesthesia value, was used to evaluate hemodynamic changes.
The anesthetic duration was measured from the time of induction of anesthesia until the time of discharge of a patient in the PACU, and it was recorded whether the patient was under general or spinal anesthesia.
Postoperative pain was evaluated. Therefore, the number of patients that required analgesia was recorded.
Aldrete score was evaluated when patients were admitted in and before discharging a patient from PACU. The five critical parameters considered were physical activity, degree of wakefulness, oxygen saturation, breathing, and circulation. A score of eight and above indicates that a patient is fit and can be discharged.
The duration time of patients in PACU was recorded as the time to discharge. It was evaluated when the patient was admitted to the PACU, whether awakened or unconscious, under respiratory assistance until the patient was discharged from PACU.
Complications that occur before the discharge of patients from PACU, such as postoperative nausea and vomiting, were recorded.
To present continuous data, both mean and standard deviation were employed, as percentages or frequencies for categorical data. The one-way ANOVA was used to make comparisons, followed by post hoc analysis or the chi-square test. The Kruskal-Wallis test was used to compare ordinal data. The SPSS 25.0 program was used for all statistical analyses. Statistical significance was defined as a P-value less than 0.05.
For the study, a total of 159 patients were collected, and 9 patients were ruled out. 114 men (76%) and 36 women (24%) mean age 76 years, mean weight 66.8 kg, ASA I n = 7 (5%) ASA II n = 106 (70%) ASA III n = 37 (25%) population information among groups was comparable (Table 1).
Table 1: General information on the study population. View Table 1
Heart rate and systolic and diastolic blood pressure fluctuations were statistically significant among the three groups: high, medium, and low in spinal anesthesia, general anesthesia with intubation, and general anesthesia with LMA; all had P < 0.001. (Table 2). Within each group, the heart rate was found to be statistically significant in comparison to all groups. However, only the statistical significance of systolic and diastolic blood pressures was observed in comparing general anesthesia with laryngeal mask airways, GA with intubation, and SA. However, in comparison between GA with laryngeal mask airways and GA with intubation, there was no significance, P > 0.05.
Table 2: Perioperative hemodynamic. View Table 2
The total number of patients that required analgesia was 64 (42.67%). The use of analgesics differed significantly in the three groups. The number of analgesic usages among the groups was statistically high in GA with intubation 37 (74%), followed by GA with laryngeal mask airways 15 (30%) and SA 12 (24%), all P < 0.001 (Figure 2). The group comparison showed statistical significance between GA with intubation, GA with laryngeal mask airways, and SA. P < 0.001, unlike GA with laryngeal mask airways and SA showed no statistical significance, P > 0.05. On the other hand, 86 (57.33%) patients did not require analgesia.
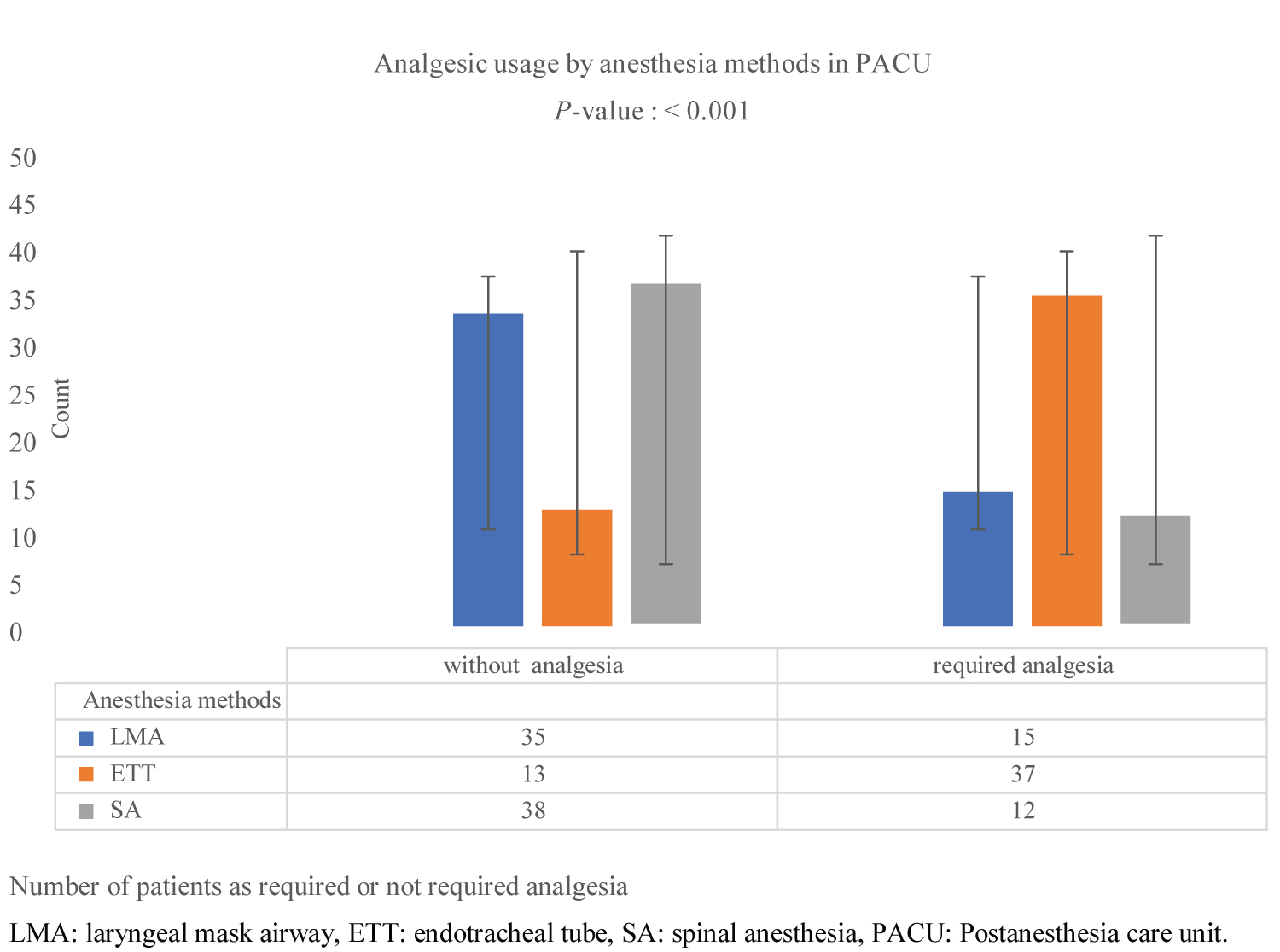 Figure 2: Comparison of analgesic usage.
View Figure 2
Figure 2: Comparison of analgesic usage.
View Figure 2
The Aldrete scoring system by the time of admission in PACU patients between the three groups was as follows 8, 6, and 5 mean values for SA, GA with laryngeal mask, and GA with intubation, respectively, with P < 0.001 (Figure 3). However, the comparison within the groups showed statistical significance between them GA with a laryngeal mask GA with intubation and spinal anesthesia.
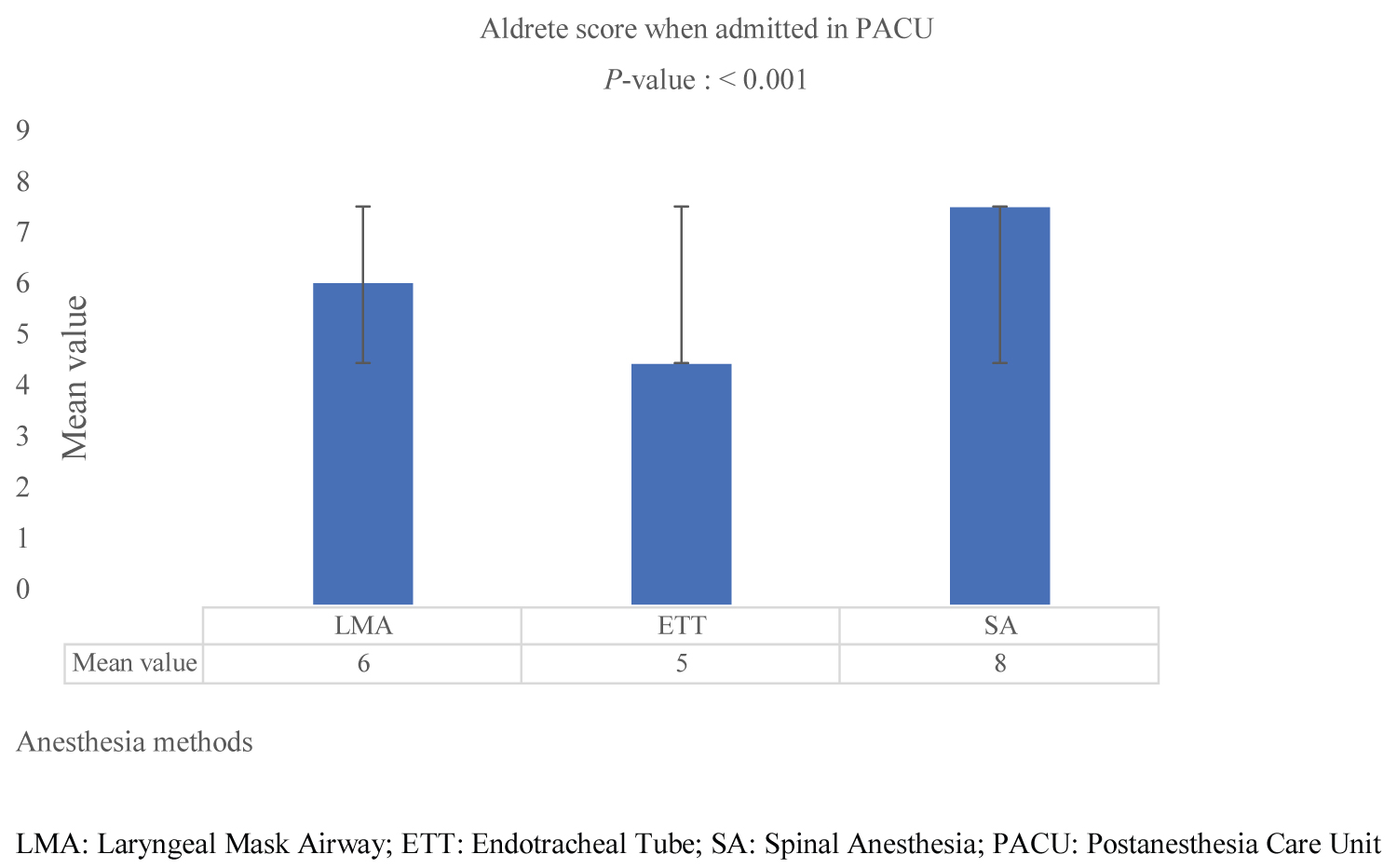 Figure 3: Comparison of the Aldrete scoring system.
View Figure 3
Figure 3: Comparison of the Aldrete scoring system.
View Figure 3
In the Postanesthesia care unit, the mean duration from admission to discharge was statistically significant, and it differed between the groups from longer, medium to shorter in GA with intubation (54.60 min), GA with laryngeal mask airways (24.80 min), and SA (23.52 min) respectively, with P < 0.001 (Table 3). Within the groups, the comparison between the mean duration of GA with intubation, GA with laryngeal mask airways, and SA was statistically significant. Unlike the comparison of mean duration between GA with laryngeal mask airways and SA, which showed no statistical significance, P > 0.05.
Table 3. Duration and complications. View Table 3
The mean duration from the induction of GA or puncture of SA to the time when patients were discharged to PACU was statistically significant. Compared to GA with laryngeal mask airways (106.78 min) and SA (98.16 min), the mean duration of GA with intubation (165.92 min) was more prolonged, P < 0.001 (Table 3). Within the groups, the comparison between GA with intubation, GA laryngeal mask airways, and SA was significant statistically, with P < 0.05. However, the comparison among GA with laryngeal mask airways and SA was insignificant, P > 0.05.
Postoperative nausea and vomiting were recorded only in SA 4 (8%); therefore, the comparison between the group showed a statistical significance, P = 0.016 (Table 3). Within the groups, the comparison between SA, GA with intubation, and GA with laryngeal mask airways was significant, unlike the comparison between GA with intubation and GA with laryngeal mask airways was not significant, P > 0.05.
Apart from nausea and vomiting, no other complications were recorded among the three groups.
This study showed that using the laryngeal mask is profitable for endotracheal intubation overall outcomes of the two general anesthesia. Several reviews discovered that the incidence of airway complications and time management were better in a laryngeal mask [8-10].
It was found in this study that compared to general anesthesia with ETT and spinal anesthesia, general anesthesia with LMA was associated with less significant hemodynamic changes, which was comparable to the study others [11]. Supraglottic airway mechanisms are associated with the fewest hemodynamic changes during general anesthesia [12]. Particularly in aging patients, the intubation and extubation led to hemodynamic instabilities in pulse rate and blood pressure, augmenting the possibility of cardiovascular attack [13]. However, in this study, the hemodynamic variation of the two general anesthesia techniques was statistically the same. Furthermore, spinal anesthesia showed significantly more variations than other methods due to vagus nerve dominance, which led to peripheral vascular dilation and a sluggish heartbeat during spinal anesthesia [14].
In this study, we discovered that statistically, the GA with laryngeal mask airways and spinal anesthesia were equally profitable in terms of the anesthesia duration, the analgesic usage inside the post-anesthesia care unit, as well as the time to discharge from PACU, which is consistent with other studies [15,16]. Unlike general anesthesia, intubation was associated with a longer duration of anesthesia which may influence the high number of analgesia usage and the prolongation of the time to discharge from PACU. Another study showed that intraoperative factors like general anesthesia, long duration of surgery, and postoperative pain contributed to a delay in discharge [17].
This study demonstrated that the Aldrete scoring system was better in the spinal anesthesia method; this might be because the five key parameters evaluated to ensure the safe discharge of patients postoperatively were maintained during spinal anesthesia. In their research, Doss NW, et al. came up with a similar conclusion [18].
Apart from nausea and vomiting in the spinal anesthesia group, our study found no other complications contradicted research conducted by others. In their study, Obrink E, et al., more PONV was observed in general anesthesia groups [19]. However, the SA itself may be a risk to PONV [6]. In addition, this could be a result of the population's aging factor. Furthermore, in our study, as the duration of anesthesia was also prolonged, it was reasonable to use an analgesic that could lead to PONV. As a risk factor, aging and the use of aanalgesics may lead to PONV [20,21].
The main limitation of our study came from the data collection, which is from a single center affiliated with a clinical school of medicine. Data from many centers would have been statistically useful. Moreover, nursing staff in the PACU were blinded to the study, which might have interfered with a decision to discharge a patient.
General anesthesia through using a laryngeal mask airway and spinal anesthesia has many advantages. However, general anesthesia using a laryngeal mask airway is profitable intraoperatively and postoperatively, which is not the case for spinal anesthesia, which shows many hemodynamic instabilities, presenting a high risk to patients' life especially in the aging population during operations.
Future research focusing on comparison specifically between general anesthesia through the use of a laryngeal mask airway and spinal anesthesia needs to be conducted, including outcomes that were not reported in this study, such as the cost, well-being, and appreciation of patients.
We acknowledge that the assistance of the members of the staff of a day surgery center of the first affiliated hospital of clinical medicine of Lanzhou University was important, and we appreciate their contribution to the success of our study. There were no grants for this study.
No potential conflict of interest relevant to this article was reported.
Not applicable.