Background: The risk of thrombosis due to idiopathic nephrotic syndrome (INS) appears to be proportional to massive protein leakage. This massive leak could be linked to the overexpression of the c-mip gene. The objective of the current study was to investigate the involvement of the c-mip gene in the risk of occurrence of thrombosis in children with INS in Abidjan.
Methodology: A cross-sectional study was carried out at the pediatric nephrology unit of University Hospital of Yopougon from January 2021 to April 2022. Children with INS aged 24 to 144 months were recruited. Blood samples were taken in tubes without or with an anticoagulant such as citrate, and EDTA. Albuminemia was assessed using Cobas C311. Fibrinogen, D-dimers and antithrombin III (ATIII) were assayed on the Sysmex CS1600. Expression levels of the c-mip gene were determined using the ddCt relative quantification method with the housekeeping gene GAPDH as the normalization standard. The risk of thrombosis was defined in front of an albuminemia < 20 g/L, a fibrinemia > 6 g/L, an ATIII < 70% or D-Dimers > 1000 ng/ml.
Results: Out of the 33 patients with INS, the risk of thrombosis was found in 18 (54.5%) children. Some children had a single risk factor and others had a combination of several risk factors. The link between the expression of the c-mip gene and the various thrombotic risk factors could not be established. Therefore, the expression of the c-mip was not correlated to the risk of occurrence of thrombosis in children with INS.
Conclusions: There is a risk of occurrence of thrombosis in children with INS. However, that risk was not related to the levels of expression of the c-mip.
Thrombosis, c-mip, Idiopathic nephrotic syndrome, Child, Abidjan
The idiopathic nephrotic syndrome (INS) or nephrosis is a kidney disease originating from the glomeruli. It is the most common glomerular nephropathy in pediatrics although, its epidemiology is still poorly understood [1, 2]. It is characterized by an alteration of the podocytes by various mechanisms favoring an increase in the permeability of the glomerular membrane which will let through the proteins. The podocyte alteration was previously reported to be linked to the overexpression of the c-mip gene. This gene, which is not expressed in healthy individuals, is expressed conversely in immune cells and in podocytes during INS [3]. The overexpression of the c-mip gene would be the cause of the massive loss of proteins in the urine and the ensuing hypoprotidemia. The hypoproteidemia drives most of the clinical consequences of the nephrotic syndrome such as infections, dyslipidemia and thromboses. The thromboses are due to the loss of anti-coagulant proteins such as Antithrombin III (ATIII) [4] and the overproduction of procoagulant factors [5]. So far, no study was conducted in Cote d'Ivoire to assess the biological markers of thrombotic risk in children's INS and the involvement of the c-mip gene in that risk. The present study aims to find the existence of a link between the expression of the c-mip gene and the risk of occurrence of thrombosis in children with INS in Abidjan.
This study recruited children aged 24 to 144 months with idiopathic nephrotic syndrome (INS) that consulted at the pediatric nephrology unit of the University Hospital of Yopougon. The parents of these children gave their informed and signed consent. The study was approved by the National Ethical Committee for Life Sciences and Health of Cote d'Ivoire. The parents of these children gave their informed and signed consent. The idiopathic nature of the nephrotic syndrome (NS) was ascertained for all children aged 24 to 144 months at the time of diagnosis and whose etiological assessment (HIV serology, malaria serology, Hepatitis B and C serology, schistosomiasis serology) had returned negative. A pool of control patients was constituted for the measurement of the expression levels of the c-mip gene and they were children aged 24-144 months healthy for the INS. Children with non-compliant samples (coagulated, insufficient quantity) were not included in the study. Any child with a urinary tract infection was excluded from the study.
A cross-sectional study was conducted from January 2021 to April 2022. The recruitment of patients and the samples collection took place at the pediatric nephrology unit of the University Hospital of Yopougon. The control subjects were recruited at the pediatric unit of the National Institute of Public Health (INSP) of Adjame. Storage at -80 °C of the biological specimens took place at the INSP Malaria Research and Control Center. Fibrinogen, D-dimers and ATIII were assayed at the Longchamp Laboratory in Abidjan. The albumin assays were carried out at the biology and medical research laboratory of the INSP. The expression levels of the c-mip gene was measured at the Molecular Biology Unit of the Center for Diagnosis and Research on AIDS and other infectious diseases (CeDReS).
The socio-demographic data was collected with a survey sheet. The venous blood samples from INS subjects were drawn on tubes with citrate or EDTA as anticoagulant, or on dry tube. Whole blood from the control subjects were sampled on an EDTA containing tube. The samples collected in a citrate containing tube underwent a double centrifugation at 3000 revolutions/min for 15 min to obtain plasma aliquots. Those aliquots were used for the assessment of fibrin, ATIII and D-Dimers levels. The sera were obtained after centrifugation at 1500 rpm for 5 min of blood samples collected on dry tubes. Aliquots of sera were made and used to assay albumin levels. Aliquots of whole blood collected in EDTA containing tubes was aliquoted for the measurement of the expression levels of the c-mip gene. All the aliquots were stored at -80 °C before further processing.
The aliquots of serum were first thawed in a water bath at 37 °C for 10 min and homogenized. From them, albumin levels were assessed using the ALB2 reagent from Cobas, a colorimetric test performed on the Cobas C311 automaton. The aliquots of plasma were also thawed and used for the coagulation tests on the CS1600 automaton. The reagents for the fibrinogen were the Dade Thrombin and Dade Owrens’ veronal buffer reagents based on a chronometric test. The reagent for the ATIII was the Berichrom antithrombin III kit based on a colorimetric test. The reagent for the D-dimers was the Innovance D-Dimers reagent used in an immunoassay. The tests were carried out according to the manufacturer's instructions. The risk of thrombosis was defined at least one of the following, a serum albumin level < 20 g/L, a serum fibrin level > 6 g/L, an ATIII level < 70% and a D-Dimers levels > 1000 ng/ml [6]. For molecular testing, the whole blood was thawed and subjected to an automated RNA extraction with the GXT NA kit on Hain's GenoXtract machine. The quality and quantity of the extracts were evaluated with the UV/visible spectrophotometer Biophotometer of Eppendorf. The extracts were amplified by a real-time RT-qPCR technique with SYBR Green detection chemistry using the RNA to Ct reagent and the Quant Studio Dx5 real-time thermal cycler from Invitrogen. The conditions of the RT-qPCR were a reverse transcription step at 50 °C for 30 minutes followed by the activation of the Taq polymerase at 95 °C for 3 minutes. Once the Taq polymerase is activated, 40 cycles of PCR were run with each cycle consisting in a denaturation phase at 95 °C for 15 seconds followed by a hybridization coupled with an elongation phase at 63 °C for 45 seconds. The ddCt relative quantification method was used in the presence of the housekeeping gene, glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as normalization standard. Expression of the c-mip gene in controls ranged from 55 to 150%. Below 55%, gene expression was considered low and above 150, gene expression was considered high.
The data was computerized and analyzed on the Excel 2013 software. The results made it possible to determine the main statistical parameters, which are the average (m) and the standard deviations (s) for Gaussian distributions or the median (Med), the first quartile (Q1), and the third quartile (Q3) for non-Gaussian distribution. Fischer's exact statistical test was used and considered significant if p < 0.05.
Over the study period, 33 children with INS and 10 control subjects were recruited.
A male predominance was noted with a sex ratio of 1.2 among INS affected subjects. The average age was 54.9 ± 30.2 months with the age group of 24-59 months being the most common (Table 1).
Table 1: Distribution of children by age and sex. View Table 1
The risk of thrombosis was present in 18 children (54.5%) of the children with INS. Hypoalbuminemia defined as an albumin level in the serum below 20 g/L was found in 66.7%. The same proportion of children with INS had D-dimers levels above 1000 ng/ml. The fibrinogen level was higher than 6 g/L in 50% of the INS affected children. And the level of ATIII was under 70% in 38.9% of the aforementioned children (Table 2).
Table 2: Thrombotic risk factors. View Table 2
Seven children had a single risk factor whereas in the other cases, several risk factors were combined (Table 3). Among these children, hypoalbuminemia was below 20 g/L in 12 children (66.7%), hyperfibrinemia was above 6 g/L in 9 children (50%), the D-dimers levels were over 1000 ng /ml in 12 children (66.7%), and ATIII was less than 70% in 7 children (38.9%).
Table 3: Distribution of children by the thrombotic risk factors. View Table 3
The measurement of c-mip gene expression levels showed significantly higher expression levels in children with INS compared to the control subjects (Figure 1).
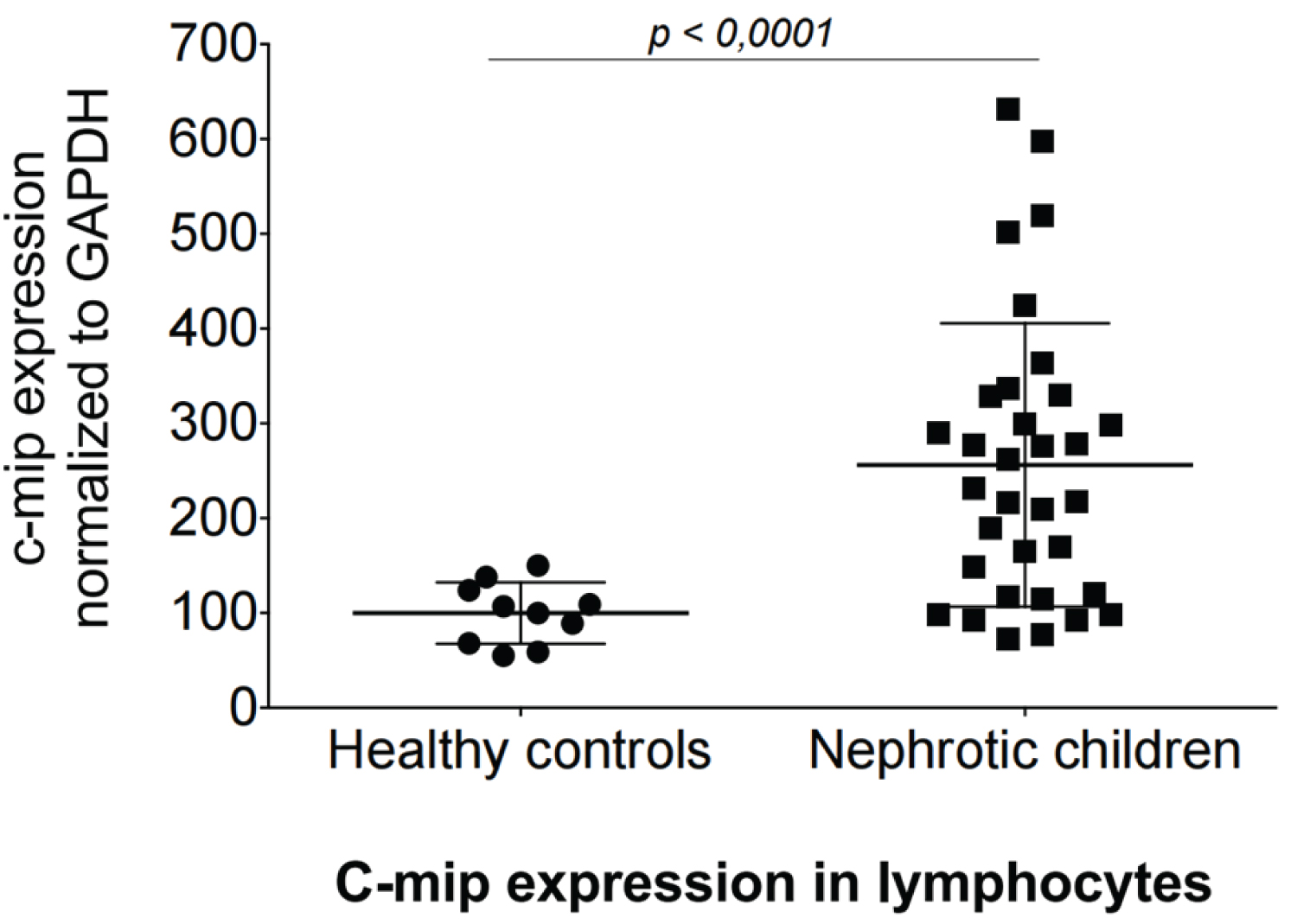 Figure 1: Expression levels of the c-mip gene normalized to GAPDH (ddCt analysis).
View Figure 1
Figure 1: Expression levels of the c-mip gene normalized to GAPDH (ddCt analysis).
View Figure 1
No link could be found between the expression of the c-mip gene and the various parameters for the assessment of the thrombotic risk such as albumin, D-dimers and ATIII levels (Table 4).
Table 4: Data on cross-analysis between c-mip expression and thrombotic risk factors. View Table 4
Statistical tests showed that there was no link between the level of expression of the c-mip gene and the risk of occurrence of thrombosis (Table 5).
Table 5: Relationship between c-mip expression and thrombotic risk. View Table 5
The INS is the most common glomerular nephropathy in pediatrics [7, 8]. A male predominance was noted with a sex ratio of 1.2 in the current study. This result is in agreement to that found in the study by Ernould, et al. in France [9]. The average age was 54.9 months ± 30.2, which is similar to the results found in Europe, Asia and America that reported an average age of 60 months [9]. However, Keita in a study conducted in Senegal found an average age of 85.3 months [10]. Niaudet described the nephrotic syndrome as the most frequent renal pathology in children between 24 and 72 months [11]. Moreover, the nephrotic syndrome is considered a disease with high thromboembolic risk in both children and adults [12]. However, the incidence of thromboembolic complications in patients with nephrotic syndrome is by far lower in the pediatric population with 1.9% compared to 4% in adults according to the study by Orth, et al. [13]. This incidence is certainly underestimated due to the fact that many thromboembolic events are without clinical manifestation [14]. High-risk patients are defined by serum albumin level below 20 g/L and/or fibrinogen above 6 g/L and/or D-dimers level above 1000 ng/ml and/or ATIII level under 70% [15]. These different biological disturbances are often found associated in the same patient, as was the case in the current study. The combination of hypoalbuminemia and hyperfibrinemia may justify the start of treatment with anticoagulants [16]. The risk of thrombosis was demonstrated in 18 children (54.5%) in this study. Tahar, et al. in Tunisia showed hypoalbuminemia in all children with a thromboembolic complication, while hyperfibrinemia and D-dimers were each found in 66.7% of these children [17]. Abnormalities of hemostasis, contributing to a state of thrombophilia during the nephrotic syndrome, are essentially linked to urinary leakage of coagulation-inhibiting factors and mainly ATIII. The plasma activity of ATIII is then found to be reduced, thus constituting a state of hyper-coagulation [18]. Jeanne, et al. report an ATIII level of less than 70% in 64% of patients at the time of the occurrence of a thromboembolic accident [19]. The c-mip gene has been described as being responsible, when expressed, for urinary protein leakage during INS. Oniszczuk, et al. showed that this gene, which is weakly or not expressed in the tissues of healthy individuals, is strongly expressed during relapses both in T lymphocytes (LT) as well as in the podocytes which are the target cells of the INS [20]. In the current study, the expression levels of this gene were higher in children with idiopathic nephrotic syndrome compared to the healthy control children. There was no link between the expression of the c-mip gene and hypoalbuminemia or any other thrombotic risk factors assessed. These results are in agreement with those obtained by Vermorel, et al. who did not demonstrate any link between the glomerular expression of c-mip and the degree of proteinuria [21].
Thrombosis remains a redoutable complication during INS in children. There is little to no data on the frequency of this complication in children with INS in Sub-Saharian Africa. Henceforth, no study in that context has ever looked into the involvement of the c-mip gene in the thrombosis risk in children with INS. Although the risk of thrombosis has been found in certain children, the level of expression of this gene was not associated with an increase in the occurrence of a thrombotic risk.
The authors would like to thank the managers and staff of the Pediatric Nephrology Unit and the central laboratory of the University Hospital of Yopougon, the Center for Research and Fight Against Malaria, as well as the Biology and Medical Research Laboratory and the Pediatrics Department of the National Institute of Public Health, the Longchamp laboratory, and the Center for Diagnosis and Research on AIDS and other infectious diseases of the University Hospital of Treichville for their availability and their help in carrying out this work. Our thanks also go to all the parents who accepted that their children be participants to the study, and the children themselves.
The authors state that they have no conflicts of interest.
This research did not receive any specific funding from any public, commercial, or non-profit organization.
All authors contributed equally in the study. They made substantial contributions to the design of the study, the collection of the data as well as the preparation and analysis of the data. They also drafted the manuscript and gave final approval for its submission to the journal for consideration of publication.