Iron deficiency anaemia (IDA) has been observed concomitantly with unexplained leukopenia. However, this association is limited in literature. We investigated the association between IDA and leukopenia and explored iron therapy as a novel approach to improving immune function in patients with leukopenia.
A retrospective cohort study was conducted in females undergoing gynaecological surgery. Females with IDA and without IDA were the test and control groups respectively.
Five-hundred and two females were included (214 IDA, 306 non-IDA). IDA compared to non-IDA patients had significantly lower white cells (5.6 (1.8 SD, 95% CI 5.4-5.9) × 109/L vs. 6.5 (2.1 SD, 95% CI 6.2-6.7) 109/L) and neutrophils (3.1 (1.4 SD, 95% CI 2.9-3.3) 109/L vs. 3.6 (1.7 SD, 95% CI 3.4-3.8) 109/L). Ethnicity was a confounder with Black females having a lower WCC and neutrophils than others. In the 214 patients who received intravenous iron, there was no effect on their WCC or neutrophil counts.
Our study reveals an association between IDA and leukopenia and neutropenia. The failure of iron to increase WCC and neutrophils demonstrates the complexity of the iron-leukopoiesis relationship, defying a simplistic dose-response explanation. Basic science research is warranted. Moreover, our findings underscore disparities in standard care for Black patients.
Haemoglobin (Hb) is an iron-containing protein in erythrocytes or red blood cells (RBC) that transports oxygen throughout the body. Anaemia is the state in which there is a lack of Hb, defined by the World Health Organization (WHO) as < 130 g/L in men and < 120 g/L in women [1]. Iron deficiency anaemia (IDA) is the cause of approximately half the global anaemia burden [1,2]. Women are particularly susceptible due to increased iron losses during menstrual blood loss. Iron plays an important role in various processes including erythropoiesis, oxygen transport, energy production, and cellular immunity. Thus, iron deficiency can lead to a reduced quality and quantity of these crucial processes, ultimately resulting in clinical manifestations such as fatigue, dyspnoea, heart failure, and susceptibility to infection [3].
At our institution, a pre-operative anaemia pathway exists to optimise patients before planned surgery. Patients listed for any planned major blood loss surgery with an estimated blood loss (EBL) of 500 mls or more, or a 10% or more risk of donor red cell blood transfusion, undergo laboratory tests: full blood count (FBC), ferritin and total iron-binding capacity (TIBC). Patients found to have a low Hb (< 130 g/L) with concomitant low ferritin level (< 30 mcg/L) and iron saturations (< 20%) are referred to the pre-operative anaemia service for Hb optimisation, which may include an intravenous (IV) iron infusion. A common cohort of patients receiving iron and Hb optimisation within the pre-operative anaemia service, are female patients awaiting planned gynaecology surgery.
Anecdotal experience from the pre-operative anaemia service has observed that patients with absolute IDA are commonly found to have concomitant unexplained leukopenia: Reduced levels of leukocytes or white blood cells (WBC). White blood cells are key in immune function. Consequently, leukopenia is an important clinical problem as it could indicate attenuated immune function, therefore lead to increased infection susceptibility. It has also been observed that leukocyte levels increase after receiving an iron infusion. A hypothesized mechanism for these observations is the role of iron in enzymatic function involved in leukopoiesis, as well as the role of iron in cellular immunity [4]. Current evidence of the association between IDA and leukocyte is however limited to only several case reports and observational studies from Asian populations who may have underlying differences to the population in the United Kingdom, possibly owing to diet and cultural variances [5,6]. To our best knowledge, there has been no previous cohort studies conducted in this specific patient population investigating the association between IDA and leukopenia, and the effect of iron therapy on leukocytes. Exploring this association is essential, as if indeed an association and causation exists, iron optimisation therapies could be considered as a novel indication for unexplained leukopenia to augment patients’ immune function.
Herein, we conducted an observational retrospective cohort study to investigate the association between IDA and leukopenia, as well as the effect of iron therapy on leukocytes in female patients undergoing gynaecological surgery.
We conducted a retrospective observational cohort study. This study was conducted and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies [7] (Supplementary Material S1).
Female patients aged between 18 and 50-years-old who underwent a gynaecological operation at our institution, between September 2019 and December 2022 were included in this study.
Patients with IDA (defined as Hb < 120 g/L and ferritin < 30 mcg/L) were included as the test group and attended the pre-operative anaemia clinic as per local protocol. These patients were given an intravenous iron infusion (ferric carboxymaltose, FERINJECT ® ) and were included for the secondary outcome of this study. For practical reasons, majority of patients received 1000 mg of Ferinject regardless of their initial Hb level and weight (no patients weighed below 35 kg) to optimise compliance, as administering more than 1000 mg requires two appointments at least one week apart. Post-infusion blood tests were performed 4 to 6 weeks after the infusion, or 1 week before their surgery, whichever was earliest. Treatment was deemed effective if their Hb and ferritin levels had increased to a range which allowed them to be ‘fit for surgery’ (IDA corrected).
Patients without IDA (defined as Hb 120 g/L and/or ferritin 30 mcg/L) were included in the control group for the primary outcome.
Patients without IDA who received an iron infusion, or patients with IDA who attended the clinic but did not receive an intravenous iron infusion were excluded. Patients with haemoglobinopathies, haematological malignancies, and pregnant patients were also excluded.
The primary endpoint of this study is the association between IDA and leukopenia. The secondary endpoint is the impact of subsequent iron optimisation on leukocyte count.
Exploratory outcomes include the effects of age, body mass index (BMI) and ethnicity on the association between IDA and leukopenia, and on the impact of iron therapy on leukocyte count.
Data collection was performed independently by JW, CZ, SM, and CT. Data was collected from Cerner, the electronic patient record system used by Homerton University Hospital. The following data items were collected: patient demographics (age, date of birth, weight, height, BMI, ethnicity, ASA grade), operation type, full blood count (FBC) and iron studies, dates of blood results. FBC variables collected were the Hb level and leukocyte count, including total white cell count (WCC), neutrophils, lymphocytes, monocytes, basophils, and eosinophils.
Patients in the test-group (intravenous iron optimisation) also had additional data collected: date of iron infusion and total dose, and post-optimisation blood test results (FBC, ferritin and iron studies).
Data was entered and anonymised onto a pre-designed proforma on Microsoft Excel and stored on a secure password-protected server. Access was granted only to team members (JW, CZ, SM, CT).
All data and statistical analyses were performed on IBM ® SPSS ® Statistics for Windows (version 28). FBC and iron studies data were dichotomized into categorical data (“normal” and “low”) based on pre-determined laboratory ranges (Supplementary Material S2). Age, weight, BMI, ethnicity, and ASA grade were evaluated as potential confounding variables.
The study includes both between-subject and within-subject designs for the data collection. For the between-subject data the statistics used for analysis included Chi-square and Independent Samples t-tests, with Mann-Whitney U tests used for any continuous data that failed the Levene Test for homogeneity of Variances. To evaluate the effect of the possible confounding variables, a series of Univariate Analysis of Covariance (ANCOVA) were used (Univariate General Linear Modelling). From the results of the ANCOVAs it was decided to further investigate the effect of Ethnicity as a main effect, rather than as a confounding variable, so a series of One-way Analysis of Variance (ANOVA) were performed. Post hoc tests were used to investigate any differences between categories.
For the within-subject data which compares pre- and post-therapy blood results from the same individual, the statistics used included the Wilcoxon Signed-Rank Test and Paired Samples t-tests. To evaluate the effect of the possible confounding variables, a series of Repeated-Measures Analysis of Covariance were used (Repeated Measures General Linear Modelling).
A p-value of < 0.05 was taken as the threshold of significance. A power calculation was performed during our pilot study. It was estimated that 15% of patients with IDA will have leukopenia, and 5% of patients without IDA (the control group) will have leukopenia. Power calculations based on an alpha level 0.05 and 80% power, determined that a sample size of at least 160 was required in each group.
Five-hundred and twenty patients were included in the study from September 2019 to November 2022, with 214 patients in the IDA (test) group and 306 in the non-IDA (control) group. Patient demographics are found in Table 1. There was no difference in weight and BMI between the IDA and non-IDA groups. Statistically significant differences were found in age, ethnicity, and ASA grade between both groups. Overall, there were significantly more Black patients who underwent gynaecological surgery compared to other ethnicities. There were also significantly more Black patients who had IDA compared to those without IDA, compared to other ethnicities.
Table 1: Patient demographics for the IDA and Non-IDA groups. View Table 1
Leukopenia was significantly associated with IDA when compared to non-IDA: 14.5% vs. 5.9% respectively, p < 0.001 (Table 2). A similar relationship was seen when leukocyte count was treated as a continuous variable, where the mean WCC for patients with IDA and non-IDA was 5.6 ± 1.8, 95% CI 5.4-5.9 and 6.5 ± 2.1, 95% CI 6.2-6.7 respectively, p < 0.001 (Table 3).
Table 2: Association between iron deficiency anaemia and Leukopenia. View Table 2
Table 3: Difference in leukocyte count between IDA and non-IDA groups. View Table 3
Similarly, neutropenia was associated with IDA when compared to non-IDA: 22.0% v. 14.1% respectively, p = 0.019 (Table 2). A similar relationship was observed when the neutrophil count was treated as a continuous variable with IDA and non-IDA groups: 3.1 ± 1.4, 95% CI 2.9-3.3 and 3.6 ± 1.7, 95% CI 3.4-3.8 respectively, p < 0.001 (Table 3).
For the lymphocyte count, a significant statistical difference between IDA and non-IDA groups was found when treated as a categorical variable (1.4% vs. 8.2% respectively, p < 0.001), although no difference was seen when lymphocyte count was treated as a continuous variable. Conversely, for the monocyte count, no difference was observed when treated as a categorical variable, however there was a significant statistical difference seen when comparing as a continuous variable with lower monocyte levels in the IDA group (Table 2 and Table 3). It should be noted that the number of cases of low lymphocyte and monocyte count was small and the absolute difference between groups also small, which may negate the findings of statistical difference.
We investigated the influence of potential confounding factors including age, BMI, ASA, and ethnicity, on the association between IDA and leukopenia. Age and BMI were not confounders to the association between IDA and leukocytes. There existed an interaction relationship between ASA and IDA, which can be attributed to the notion that patients with IDA by default have a higher ASA grade as IDA is a systemic disease.
Ethnicity was a confounding factor of the association between IDA with WCC, and IDA with neutrophils (Figure 1). Particularly, the Black ethnicity was significantly associated with both leukopenia and neutropenia (both p < 0.05), and IDA. Even after controlling for ethnicity, IDA was still associated with leukopenia (p < 0.018), although the significant association found between IDA and neutropenia was lost (p = 0.138). Overall, Black patients were found to have a significantly lower WCC (5.4 ± 1.5, 95% CI 5.2-5.6) and neutrophil count (2.8 ± 1.2, 95% CI 2.7-3.0) than other ethnicities (Supplementary Material S3).
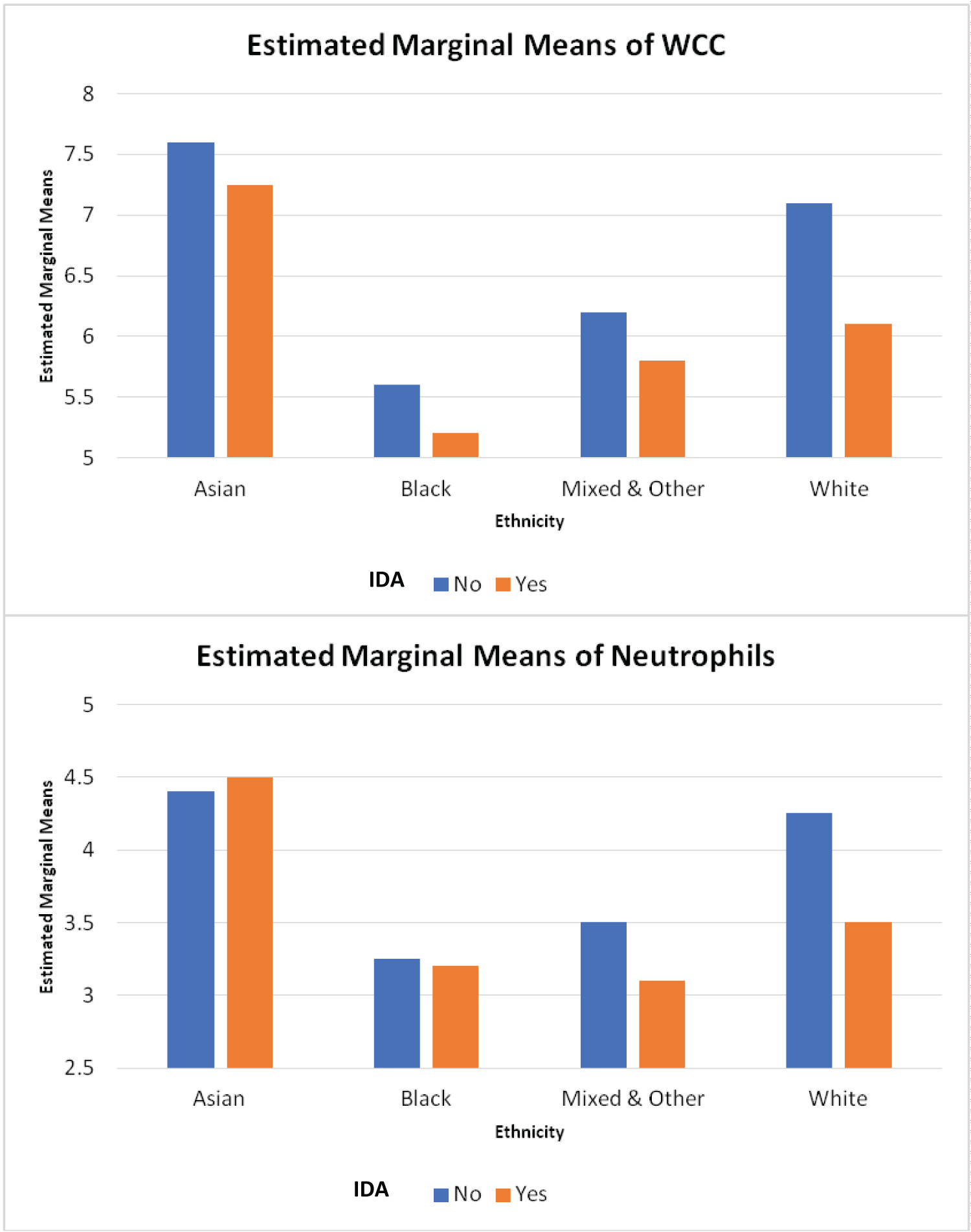 Figure 1: Relationship between ethnicity with IDA status (A) white cell count and (B) neutrophil count.
View Figure 1
Figure 1: Relationship between ethnicity with IDA status (A) white cell count and (B) neutrophil count.
View Figure 1
For the secondary outcome investigating the impact of intravenous iron optimisation on leukocyte count, 214 patients who received an iron infusion were included. Patient characteristics are shown in Table 4.
Table 4: Patient demographics for women who received an intravenous iron infusion. View Table 4
Receiving intravenous iron optimisation significantly increased the post-infusion Hb, iron saturations, and ferritin levels as expected (all p < 0.001). There was no significant difference found in WCC and neutrophil count post-iron infusion. There was a statistically significant difference in lymphocyte and monocyte count post-iron infusion, although the absolute difference was clinically small (Table 5).
Table 5: Change in iron studies and leukocyte counts pre- and post-infusion. View Table 5
Subgroup analyses were performed of patients who received the correct dosage and under-dosage of iron for their weight and initial Hb (Supplementary Material S4), to investigate if an under-dosage of iron impacted results. There was an equivalent number of patients who received the correct dosage and under-dosage of iron. There were no changes to the results whether or not patients received a dose corrected for their weight and baseline Hb. Another subgroup analysis was performed to examine only patients who had a low leukocyte level to begin with. There was no improvement in leukocyte count after an iron infusion in patients with an initial low leukocyte count (Supplementary Material S5). It should be noted that sample sizes were small.
Controlling for ethnicity did not change the within-subject results. However, there was a significant between-subject effect of ethnicity, similar to that seen in the prior section, where Black patients had a significantly lower leukocyte count than other ethnicities (p < 0.001) (Supplementary Material S6). Controlling for age and BMI made the significant differences seen in lymphocyte and monocytes statistically insignificant (both p > 0.05).
From the results of the Analyses of Covariance which found that ethnicity had a main effect on various dependent variables, it was decided to further investigate the effect of ethnicity as a main effect. The main results from these separate analyses for each dataset can be found in the Supplementary Material (Supplementary Material S7). In summary, it was found that ethnicity had a main effect on age, BMI, Hb, ferritin, WCC, neutrophils, and lymphocytes. Importantly, it was found that Black ethnicity patients had a lower mean age and a higher BMI when they presented for surgery. Black ethnicity patients also had a significantly lower Hb, WCC, and neutrophil count. Asian patients had a significantly higher ferritin and lymphocyte count.
Our observational study in female patients awaiting planned gynaecological surgery showed that IDA is associated with leukopenia and neutropenia. Although ethnicity was a confounding factor in this relationship, controlling for it still showed that IDA is associated with a low WCC. Intravenous iron optimisation significantly improved Hb, iron saturations, and ferritin levels, irrespective of the recommended dosage based on weight and initial Hb. However, it did not improve the leukocyte count in patients with IDA, even after accounting for potential confounders such as age, BMI, and ethnicity.
This study is the first to explore the association between leukopenia and IDA and the impact of intravenous iron therapy on leukocyte count. Our findings contrast with a previous study by Yassin, et al., who reported a lower prevalence of leukopenia (5.1%), neutropenia (4.0%), and lymphopenia (1.2%) in a cohort of patients with IDA [8]. Whereas, our population had higher prevalence rates. These disparities may be attributed to the homogeneity of Yassin, et al’s. cohort, comprising Arabic female patients, and the mixed-gender nature of Lim, et al’s. cohort, which included South Korean patients [9]. In contrast, our cohort was more diverse, representing East London’s multi-ethnic population with ethnicity playing an independent role in both IDA and leukocyte count.
What sets our study apart is the significant association found between IDA and low WCC and neutrophils, supported by the inclusion of a control group which was lacking in previous studies. This robust association suggests that iron may influence leukocyte production and cellular immunity [4,10]. Even after accounting for ethnicity, a substantial link between IDA and low WCC remained. Notably, Black patients displayed higher incidence rates of both IDA and leukopenia, a well-described phenomenon attributed to genetic and environmental factors [11-13]. Of note, the rs2814778-CC genotype is associated with low WCC in Black people [14,15].
To further substantiate this relationship, one might expect a dose-response effect where increasing iron levels with therapy would enhance leukocyte levels. However, this was not the case in our study. While the cohort of Arabic female patients demonstrated increased leukocyte levels after iron therapy [8], our results differed, possibly due to the smaller sample size (only 214 patients received intravenous iron replenishment) and the unique demographic of our predominantly Black population. This underscores the complexity of the relationship between iron and leukopoiesis, with genetics playing a confounding role, as our ethnicity-related findings suggest.
Taken together, our findings that associate IDA with low WCC and neutrophils, combined with failure of levels to increase with iron therapy, shows that an intricate interplay exists between iron and leukopoiesis. This suggests that a simple dose-response relationship does not explain the phenomenon. What remains clear is the disproportionate impact on Black patients.
The Homerton Hospital serves a diverse population in the London Borough of Hackney, with a substantial non-White representation (46.9%) with 21.1% Black/African, 10.4% Asian, 6.7% ‘Mixed’, and 8.7% identified as ‘Other’ [16]. Our demographic data reveals a particular disadvantage for Black females, who represent a high proportion of gynaecological surgery patients, presenting for surgery at a significantly younger age, higher BMI, and also exhibiting a higher incidence of IDA. This emphasises the need for tailored care for Black patients and raises questions about the applicability of standard haematologic reference ranges to this population. Driest, et al. found that a majority of Black patients being investigated for a low WCC were undergoing unnecessary bone marrow biopsies as a majority of them had the aforementioned rs2814778-CC genotype [15].
This study has limitations. It is a retrospective observational study, limiting causal inferences regarding the IDA-leukopenia relationship. Additionally, the inclusion of only female gynaecological surgery patients restricts the generalisability of our findings. These women are inherently different to patients not undergoing gynaecological surgery, as their cause of IDA is intrinsically related to the reason why they require surgery - menorrhagia. Another limitation is that in a majority of cases the intravenous iron dose administered were standardised irrespective of weight and initial Hb, due to clinic capacity. However, subgroup analyses found no significant differences between those who received the correct dose and those who were under-dosed, and post-replenishment laboratory tests indicated no further IDA. Finally, the number of cases of low count for monocytes and lymphocytes were small, which limit the reliability of statistical p-values found when the variables were treated as a categorical variable.’
In conclusion, our study has elucidated a significant association between IDA and leukopenia and neutropenia. The observation that iron therapy failed to increase WCC and neutrophil counts underscores the complexity of the relationship between iron and leukopoiesis, defying a simplistic dose-response explanation. This highlights the pressing need for further exploration of this intricate relationship through basic science research before embarking on clinical trials. Moreover, our findings emphasise the alarming disadvantage experienced by Black patients, highlighting the inadequacy of conventional medical care for this ethnic group.
CT conceptualised the study; CT and JWKL designed the methodology; JWKL, SM, CT, and CZ performed data collection; JWKL performed the data analysis; JWKL, CZ, SM, and CT drafted and reviewed the manuscript.
The authors thank Kate Grayson for undertaking the statistical analyses in this study, and the Homerton Research and Innovation Department for their advice and support in conducting this study.
This work was supported by CSL Vifor in form of funding for an independent statistician.
The authors declare no conflict of interests. CT declares conference travel expenses from Pharmacosmos and honorarium from Vifor Pharma.