Background: Inherited hemoglobinopathies led by Sickle Cell Disease (SCD) are key contributors to the anaemia burden in Sub-Saharan Africa (SSA). In Tanzania, an estimated six out of one thousand newborns are born with SCD, making Tanzania the fourth country with the highest burden of SCD patients in the world and the third in Africa after Nigeria and the Democratic Republic of Congo (DRC) (Nigeria 85,000, Democratic Republic of Congo 42,000 and Tanzania 11,000). At present, curative options for sickle cell anaemia are limited and not readily available, especially in SSA where the burden is huge. Severe disease in SCD is defined as occurrences of either frequent painful vaso-occlusive crises, recurrent Acute Chest Syndrome (ACS), stroke or death as observed and defined in the infant cohort by the Cooperative Study of SCD (CSSCD) group. Low haemoglobin F, Infections, low haemoglobin levels, hemolysis, and high white blood cells have all been implicated as predictors of morbidity and mortality. This study aimed to assess the clinical presentations, laboratory features and factors associated with the severe disease among admitted SCA patients to use as indicators that could predict the disease outcome.
Methods: A retrospective study was carried out in Dar-es-salaam-Tanzania at Muhimbili National Hospital among SCA (HbSS) patients admitted in the past five years (June 2016-July 2021). demographic data, clinical presentations, laboratory indexes, treatment and clinical outcomes of admitted patients were all captured from the medical records retrospectively. The risk factors of SCA were analyzed by binary Logistic regression model, and the ability of different risk factors to predict SCA was evaluated using Receiver Operating Curve (ROC) curve analysis based on the data extracted.
Results: Duration of disease (OR = 1.310; 95% CI: 1.174-1.477, respiratory rate (odd ratio) (OR = 1.047; 95% CI: 1.016-1.081) and white blood cell count (OR = 1.026; 95% CI: 1.002-1.052) were independent risk factors for SCD. The Area under the Curve (AUC) of duration for predicting severe SCD was 0.705, the cutoff was 4.5, the sensitivity was 73.0%, and the specificity was 59.1%. The AUC of respiratory rate is 0.630, the cutoff was 37.5, the sensitivity was 29.9%, and the specificity was 92.4%. The AUC of White Blood Cells (WBC) for predicting severe SCD was 0.582, with a cutoff of 11.25, a sensitivity of 88.5%, and a specificity of 28.0%.
Conclusion: Duration of disease attack, Respiratory rate, and WBC were independent risk factors for severe SCD.
Sickle Cell Disease (SCD) is a genetic disorder caused by a point mutation. The sixth amino acid, glutamic acid, in the b-globin chain, is replaced by valine acid, which results in the formation of mutant Haemoglobin S (HbSS). Under hypoxic conditions, acidosis or dehydration conditions, HbSS polymerizes and forms linear elongated fibres that distort ("sickle") red blood cells [1]. SCD is characterized by chronic hemolytic anaemia, recurrent debilitating pain and an array of clinical sequelae, including increased risk of infection, stroke, lung disease, splenic dysfunction and bone infarction [2].
Severe SCD is defined as frequent pain, recurrent Acute Chest Syndrome (ACS), stroke and death [2]. SCA is one of the most common causes of stroke in children. Most cases are related to the lesion of the distal internal carotid artery and middle cerebral artery. Acute chest syndrome is the second most common cause of hospitalization and is a leading cause of morbidity and mortality in SCD patients [3,4].
It is estimated that more than 80% of the global annual births with SCA are born in Sub-Saharan Africa [1,3,4]. While the mortality rate of children under 5 years is 50%-90% [5] it is estimated to increase in the coming few decades [4]. Tanzania is among the five countries with the highest number of children born with SCD in the world (Nigeria 85,000, Democratic Republic of Congo 42,000, India 38,000, Tanzania 11,000 and Uganda 10,000) with an estimated 11000 births per year [5]. Despite progress to optimize the available clinical treatment like the use of transfusions, hydroxycarbamide, transplantation and gene therapy, many patients die of severe SCD every year [6].
Low haemoglobin F [7], Infections, haemoglobin levels, hemolysis, and high white blood cells have all been implicated as predictors of morbidity and mortality in the majority of cohort studies conducted in high and middle-income countries [8].
Though all sickle cell disease patients have similar genetic alterations, patients have variable clinical phenotypes with some having an extremely severe disease course while others have a milder course. This makes it difficult to predict the clinical outcome of the patient with this genetic disorder, while there are still difficulties in obtaining the existing curative option i.e. (HSCT) or the available treatment options especially in low-income countries, predicting the clinical outcome and disease severity is therefore crucial. This will help in enriching and strategizing the treatment offered consequently improving the standard of life. Predicting the severity of the disease early on would've therefore helped in initiating the disease-modifying treatment regimens including hydroxyurea or gene therapy timely before the onset of the organ damage which is often irreversible, while those with the milder course would have not been subjected to the lifetime of adverse events and toxicities from the therapeutic options provided [9]. Therefore, it became necessary to find out some indicators that are related to the severity of the disease to help in the early detection and prevention of severe SCD.
This was a five years retrospective study conducted in Dar-es-salaam at Muhimbili National Hospital. 310 patients were involved in this research. We used the logistic regression model to explore the risk factors for severe SCD. And we found that the duration of a sickle related attack, respiratory rate and leukocyte count are independent risk factors for severe SCD.
This was a retrospective cohort study designed for the evaluation of clinical presentation, laboratory features and factors associated with severe disease (ACS, stroke, frequent pain) and patients requiring blood transfusion among SCA patients admitted to Muhimbili National Hospital.
All patients with laboratory-confirmed HbSS who were admitted in the past five years (June 2016-July 2021) were studied. Informed written consent was not necessary as the study was conducted retrospectively. The data were retrospectively extracted including clinical presentations, laboratory findings, the treatment offered and the outcome of the disease. Ethical approval for the study was obtained from the ethics committee of Muhimbili University of Health and Allied Sciences as well as the Institutional Review Board (IRB) of Muhimbili National Hospital (MNH).
SPSS 13.0 was used for the statistical analysis of clinical data. Kolmogorov-Smirnov method was used to test the normality of data. The data conforming to normal distribution were expressed as X ± SEM and analyzed by an independent-sample T-test. The cases of categorical variables were represented as a percentage and analyzed by Fisher's exact test. A binary Logistic regression model was used to analyze independent risk factors of severe SCD. The Receiver Operating Characteristic (ROC) curve was used to predict the diagnostic efficacy of the indicators, and the best truncation value was selected according to the Youden index. The P < 0.05 was considered to be statistically significant.
Among 310 participants, 189 were male and 121 were female among the patients with severe disease, 62.41% (106) were male while 37.59% (71) were female patients. For the non-severe disease group, 59.89% (83) were male while 40.11% (50) were female patients, and the median age was 7 years (see Table 1).
Univariate analysis of the Severe SCD group and the Non-Severe SCD group suggested that age < 7 (P = 0.016), white blood cell count (P = 0.016), respiratory rate (P < 0.001) and duration (P < 0.001) were statistically related to severe SCD (Table 1).
Table 1: Clinical and laboratory factors in SCD patients. View Table 1
Then, the variables with the statistical difference between the Severe SCD group and the Non-Severe SCD group in univariate analysis were included in the binary logistic regression model for multivariate analysis. As seen in Figure 1, the analysis results show the duration of the attack (OR = 1.310; 95% CI: 1.174-1.477), respiratory rate (OR = 1.047; 95% CI: 1.016-1.081) and white blood cell count (OR = 1.026; 95% CI: 1.002-1.052) are independent risk factors for severe SCD.
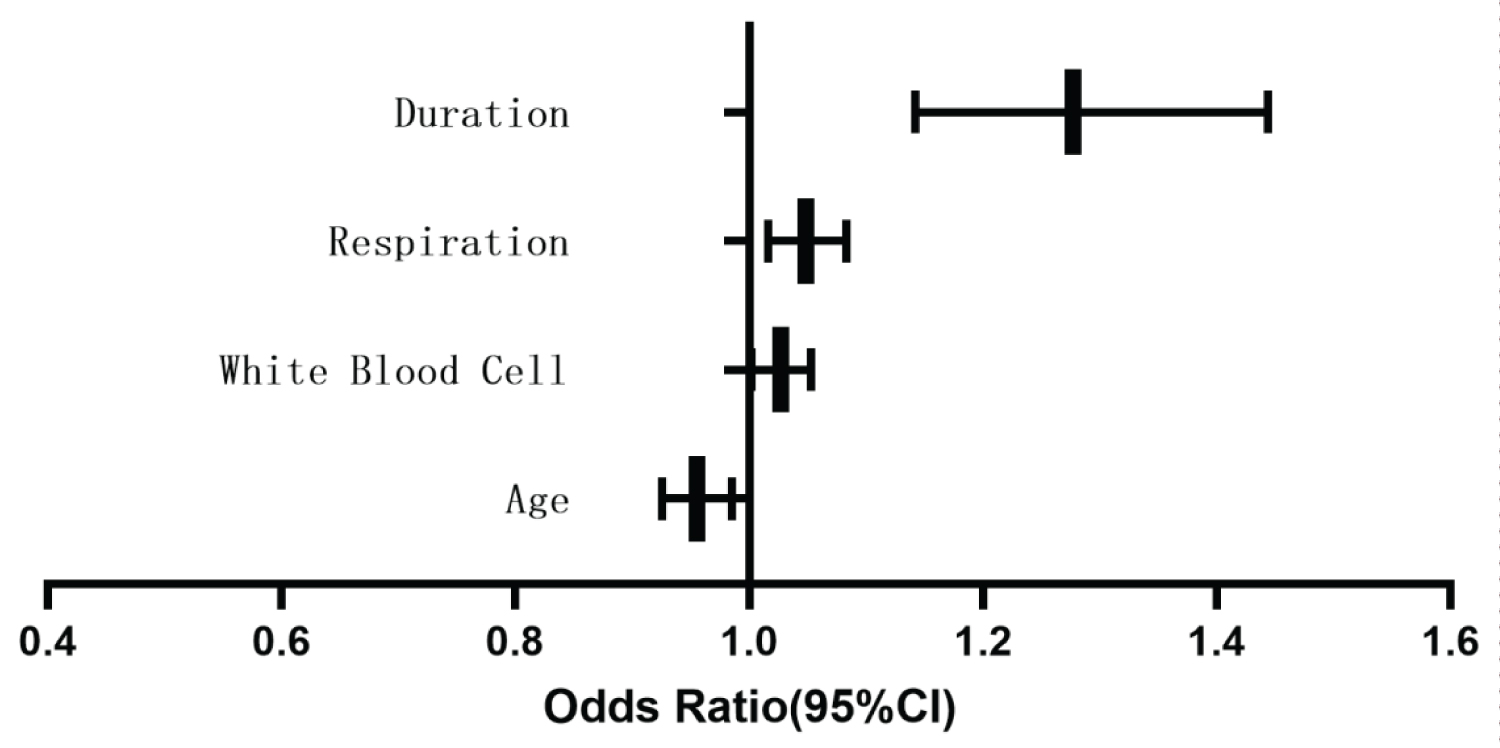 Figure 1: Forest map of binary logistic multifactor regression analysis.
View Figure 1
Figure 1: Forest map of binary logistic multifactor regression analysis.
View Figure 1
As seen in Figure 2, ROC curve analysis showed that the Area Under the Curve (AUC) of the duration of the attack for predicting severe SCD was 0.705, the cutoff was 4.5, the sensitivity was 73.0%, and the specificity was 59.1%. Respiration predicted an acute attack of SCD with an AUC of 0.630, the cutoff was 37.5, the sensitivity was 29.9%, and the specificity was 92.4%. The AUC of White blood cells for predicting severe SCD was 0.582, with a cutoff of 11.25, a sensitivity of 88.5%, and a specificity of 28.0%.
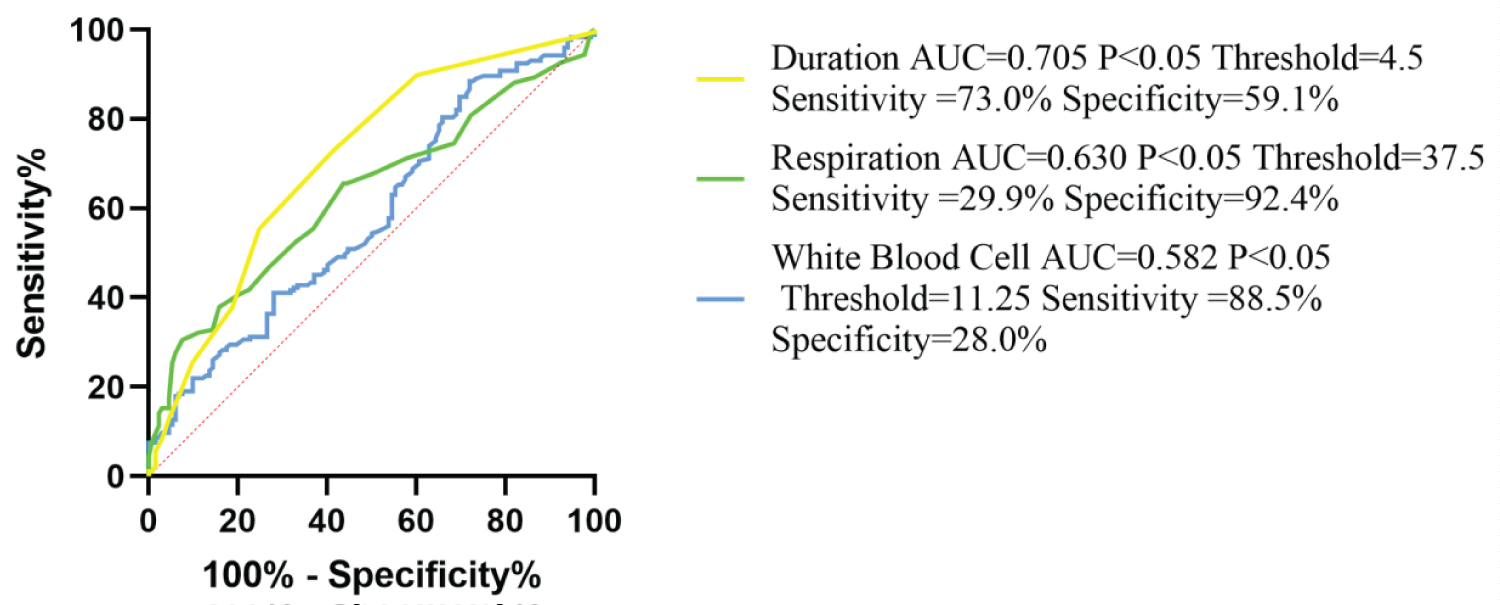 Figure 2: Analysis of ROC curve of duration, respiration and white blood cell.
View Figure 2
Figure 2: Analysis of ROC curve of duration, respiration and white blood cell.
View Figure 2
SCD is characterized by sickled red blood cells with poor deformability. From a clinical point of view, the progression of the disease can be attributed to two phenomena: hemolysis and vascular occlusion [7]. Sickled cells, activated endothelial cells, neutrophils, leukocytes and monocytes create a pro-inflammatory and pro-aggregation environment that can easily induce vascular obstruction. Moreover, ischemia-reperfusion injury secondary to microvascular occlusion promotes chronic inflammation by increasing oxidant production and leukocyte adhesion, which further leads to Vascular Occlusion (VOC) and tissue injury [10]. In the brain, vascular occlusion of cerebral blood vessels can lead to stroke. Acute chest syndrome is the second cause of SCD aggravation, which is a painful complication of vascular occlusion.
Severe disease in SCD is defined as occurrences of either frequent painful vaso-occlusive crises, recurrent Acute Chest Syndrome (ACS), stroke or death as observed and defined in the infant cohort by the Cooperative Study of SCD (CSSCD) group [11] and later by Miller, et al. in later childhood [12]. Recurrent pain and ACS are the most common complications and reasons for hospitalization in SCA patients, with ACS being the major cause of increased mortality. Prediction of severe disease is therefore crucial and will help to significantly lower the development of the severe disease among SCD patients.
In this study, we found that age < 7, white blood cell count, respiration and duration of the attack were statistically related to severe SCD. And the results of the binary logistic regression model for multivariate analysis showed that the duration of attack, respiration and white blood cell count are independent risk factors that may contribute to acute SCD attack of SCD.
The results of the ROC curve showed that the cutoff duration of sickle related attacks was 4.5 days, the Area Under the Curve (AUC) of duration for predicting severe SCD was 0.705, the sensitivity was 73.0%, suggesting that the duration of sickle related attacks is a diagnostic index for severe SCD with high predictive value. With the extension of the disease course, sickle red blood cells continue to accumulate and vascular occlusion gradually aggravates, stroke and ACS are more likely to occur, which explains the correlation between the duration of the sickle related attack and the severity of SCD. This may be the underlying mechanism by which the duration of the attack predicts disease progression. The predictive value of the duration of attack may be significantly affected by different treatment approaches. The advancement in the treatment offered has significantly shortened the duration of the sickle related crisis, especially with the use of hydroxyurea, a potent inducer of fetal haemoglobin [9]. Previous research carried out on hydroxyurea using a murine model showed that short-term administration of hydroxyurea ameliorated VOC in SCD, thus showing that hydroxyurea may have immediate benefit in the setting of VOC [13]. In addition, treatment with Hydroxyurea has shown to reduce the number of reticular cells and young low-density sickled red blood cells, that may adhere to the vascular endothelium. Hydroxyurea is relatively safe and can effectively reduce the incidence of ACS [14]. Hence, reduced the sensitivity and accuracy of the duration of attacks as a predictor of severe SCD. In summary, the ROC curve analysis showed that the duration of sickle related crisis is related to the prognosis of SCD and could be a useful screening tool, subject to the limitations of the study.
We also found that WBC is associated with severe SCD. The severity of SCD increases with leukocyte count. Leukocytes contribute to SCD by adhering to blood vessel walls and obstructing the lumen, aggregating with other blood cells with more effective blockage of the lumen, stimulating the vascular endothelium to increase its expression of ligands for adhesion molecules on blood cells, and causing tissue damage and inflammatory reaction which predispose to vaso-occlusion [15]. Studies have shown that leukocytosis was a risk factor for hemorrhagic stroke and ACS [16], this agrees with the findings from our study. The ROC curve analysis showed that the Area under the Curve of white blood cell count for predicting severe SCD was 0.585, the cutoff was 11.25, Michail, et al. found that white blood cell count is a predictor of the severity of SCD during pregnancy, however, the cutoff in their research was 6.5*109 L [17]. The mean WBC for the SCD population during pregnancy was 10.1*109 L, while the mean WBC for the SCD population in Tanzania was 15.6*109 L [8]. The differences observed in the outcomes of these researches may be due to the study population. We also found that the positive predictive value of white blood cell count was as high as 88.5%. In summary, the ROC curve analysis showed that WBC is related to the prognosis of SCD and could be a useful screening tool, subject to the limitations of the study. A long duration indicates that subsequent severe SCD complications are very likely and should increase vigilance. As a diagnostic indicator to predict SCD, WBC has a high sensitivity of 88.5%, but the AUC indicated that its accuracy is not high, which may be caused by the population restriction in this study.
ACS is defined as a new pulmonary infiltrate, presence of chest pain, fever and signs and symptoms of pulmonary illnesses including cough, tachypnoea and dyspnoea [18]. It is the second leading cause of increased hospitalization in SCD patients [19]. In our study we found that respiratory rate was an independent risk factor for severe SCD. This was also observed in several other studies, that increased respiratory rate can be used as a predictor of disease severity [3]. ACS Results from a chaotic interplay between vaso-occlusive ischemia and inflammatory cytokines. The lung undergoes a process of pathologic alveolar collapse leading to ventilation-perfusion mismatching, hypoxemia, and raised pulmonary pressures [19,20].
The results of the ROC curve analysis showed that the cutoff of respiratory rate was 37.5/min and respiratory rate predicted severe SCD with an Area under the Curve (AUC) of 0.630, suggesting that respiratory rate can predict the prognosis of the disease to some extent. However, the sensitivity of respiratory rate as a predictor of severe SCD was only 29.9%, which indicated that the rate of missed diagnosis may be higher. This may be related to sample size limitations and the presence or absence of cardiogenic complications of SCD.
Our study found that respiratory rate, duration of the attack of the disease and WBC count were independent risk factors for severe SCD. Duration of sickle related attack can be a predictor of severe SCD. A long duration of attack indicates that subsequent severe SCD complications are very likely and should increase awareness.
None.
The authors declare that they have no competing interests.