The restrictions imposed to control the COVID-19 pandemic had significant negative effects on the mental health of the general population, and particularly in nurses as frontline healthcare workers. The main goal of the present study was to analyze the direct and indirect effects, via social connectedness, of centrality of the COVID-19 outbreak on depressive symptoms. Furthermore, it is explored whether this association varied by group (nurses versus general population). The global sample included 326 individuals from the community and 316 nurses, who were administered self-reported questionnaires. Results revealed that event centrality of COVID-19 outbreak was linked to depressive symptoms, both directly and through the deterioration of social connectedness; moreover, this indirect effect was significant for both subsamples. Interventions aimed at preventing the deterioration of social connectedness may facilitate the decrease of depressive symptoms in the aftermath of the pandemic, particularly for nurses.
COVID-19, Event centrality, Depressive symptoms, Social connectedness, Nurses, General population
The coronavirus disease 2019 (COVID-19) reached pandemic proportions by March 2020, threatening healthcare systems and the well-being of the general population. The COVID-19 outbreak played a critical role in everyone's life, constituting a highly stressful, unexpected event [1,2]. Around the world, states of emergency were declared with many restrictions, such as closure of all except essential activity, and lockdowns with variable degrees. Given that humans are wired to deeply connect with others [3], public health measures (such as isolations, quarantines, and lockdowns) had a huge impact, both short and long-term, on mental and physical health of the general population and healthcare professionals in particular [4,5]. Social motives and mentalities, such as care providing and care seeking, can be vital to prevent psychological symptoms and regulate threat processing [6]. However, little is known about the role of COVID-19-related experiences on the development of depressive symptomatology.
Since the onset of the COVID-19 pandemic, a growing number of studies has shown the psychosocial impact of the coronavirus outbreak and the related social restrictions, reporting increased levels of post-traumatic stress, anxiety and depressive symptoms, insomnia, and the heightened experience of negative emotions (e.g., denial, anger, and fear) for the general population [2,7,8]. In the initial stage of the outbreak, a study on Chinese population showed moderate-to-severe depressive symptoms in 16.5% of the participants [9]. As we know from previous studies, pandemics are not gender neutral, worsening pre-existing social inequalities. Women have been affected more profoundly than men, both at workplace (constituting most of the health and social workforce) and at home, due to the increased workload following lockdown and quarantine measures. Therefore, they have been reported as more likely to develop depressive symptomatology [10].
The magnitude of the pandemic threat (e.g., work overload, fear of infecting significant others, isolation/loneliness, long COVID) enhanced the physical and mental burden of healthcare workers, but the risk of developing psychological and/or psychosomatic symptoms is particularly high among nurses [11-13]. A recent meta-analysis found that over one-fifth of nurses in professional practice during COVID-19 suffered from depression [14]. Another systematic review analyzing the psychological impact of the COVID-19 outbreak among nurses stated that 35% of the participants reported depressive symptoms [15]. Studies also demonstrate that those who are women experienced more severe symptomatology during this global health crisis, facing a higher risk of exposure to the virus, more occupational stress, family-work conflict, and unequal domestic labor [16]. Being on the frontline of healthcare services, nurses have a closer contact with patients, which exacerbates the consequences of the pandemic on their mental and physical health, as well as on the quality of their work. Fear of infecting significant others, long hour shifts, physical fatigue, lack of material and human resources, and separation from family and friends are the most important cited factors affecting these professionals' well-being. Another problem that has been reported all over the world, and enhanced by the pandemic, is staff shortage and redeployment, since many professionals had to isolate themselves because of the infection [17]. Given the fact that groups affected by the pandemic may assess the risk differently, it is crucial to document the detrimental effects of the pandemic on the mental health of nurses and the general population to inform and develop effective psychological interventions aimed at fostering adaptation. Nonetheless, the majority of studies focused on those groups separately, excluding the opportunity to evaluate the differences and similarities between them. Therefore, the invariance of adaptation patterns between both groups remains an understudied topic.
Research has demonstrated that perceiving a negative event as central to identity and life story might be associated with adverse psychological outcomes, including depressive symptoms [18]. As such, memories of highly stressful events become central by forming: 1) A reference point for the attribution of meaning to other experiences; 2) A turning point in one's own life story, and 3) A core component of the personal identity. The centrality of highly negative, unpredictable, rare events can influence their use to structure life, to give meaning to other mundane events, and to generate expectations for the future [19]. Due to the broad spectrum of impacts (e.g., social, economic, psychological, physical) caused by the COVID-19 pandemic on everyone's life, the perception of its outbreak seems to be important enough to play a pivotal role on autobiographical knowledge and the development of one's self narrative [20]. The extent to which the COVID-19 pandemic is seen as a salient personal memory for individuals may be related to their ability to cope with the adversity, as well as to the development of depressive symptoms, but this association remains unclear and needs further investigation.
Integrated in the disaster research, conservation of resources theory [21-23] suggests that people actively seek to save, defend, and develop resources. Thus, psychological distress occurs as a reaction to the environment in which there is a potential or actual loss of those key, valued resources (i.e., objects, personal characteristics, conditions, or energies). According to this perspective, individual's behaviors and reactions to environmental changes are socially framed as they act to protect and preserve the self and the attachments that establish self in social context relationship [24]. Within the specific context of large-scale trauma events, which are universally perceived as stressful, individuals' coping abilities may be threaten due to resource deterioration. Even if they tend to mobilize support immediately after the impact, its pervasive and long-lasting nature may lead to deterioration of resources. This rapid transformation from availability of support to depletion can produce a substantial negative effect on individuals' well-being [25,26].
Whether individuals experience mental health problems in the face of traumatic events may depend on the quantity and quality of their social ties. Social support, defined here as the perception of the availability of others to provide help and emotional support when needed [27], appears to be an evolutionary adaptation with survival value for humans [28]. In fact, perceived social support has been associated with the enhancement of internal resources, the reduction of the negative impact of stress on mental and physical health, and the development of resilience and personal growth [29,30]. Evidence has been showing that social support in general can act through different pathways to influence adaptation outcomes of stress, depending on the temporal and contextual factors [31]. To explain these mechanisms, literature has largely focused on two models. The "direct or main effects" model proposes that social support can have a positive impact on physical and psychological well-being, regardless of the stress levels. On the other hand, the "buffer" model posits that social support interact with stress and might inhibit, decrease, or regulate the detrimental effects of stressful events [29]. This perspective conceptualizes social support as a moderator and identifies the conditions under which the effects occur.
However, when stressful events become large-scale and prolonged in time, a mediating effect of social ties has been found [31]. According to the "support deterioration model" [25,32], disasters and catastrophic events can have an impact on mental health, both direct and indirectly. In the context of chronic, traumatizing and/or stigmatizing events, the availability of support doesn't always correspond to the need for assistance, which means social resources (e.g., social connectedness) suffer erosion and disruption along the process of coping. Negative perceptions of support might, in turn, increase symptoms of depression and anxiety. During the COVID-19 pandemic, there are many factors contributing to social connectedness deterioration, including effective losses (e.g., job loss, death of significant others, displacement), disruption of routines, successive restrictive measures (isolations, quarantines, and lockdowns), stigma, violated expectations of help [8]. However, using the support deterioration model as the theoretical framework to examine the link between pandemic-related stress and depressive symptoms remains understudied.
Even though literature consistently shows beneficial effects of social ties, it is important to clarify the facets that make those interactions a critical resource. The simple aspect of receiving adequate support from others is certainly part of it, but receiving social support is only one dimension of what it means to feel deeply connected to others. More than perceiving that help is available, the way one experiences the social world is crucial to influence physical and psychological well-being. Accordingly, individuals who perceive more support from others tend to feel their relationships as safer and warmer [33]. The concept of social connectedness captures the feelings of warmth, reassurance, and safeness elicited by soothing, threat-regulating others [1]. While social support broadly defines the relationships that individuals have, social connectedness refers to the emotional tone of that bond, illustrating the subjective affective experience. In other words, the sense of belonging narrows the focus of social ties [35].
Humans are wired to seek for connection to protect themselves from threats, to acquire resources necessary for reproduction and survival, and to work together in coping with the environment [3]. The presence or perception of a soothing, warming, and reassuring social world mitigates the impact of stressful events that lie beneath many forms of psychopathology. Feelings of social connectedness and safeness appear to be linked with the soothing-affiliation system, which plays a vital role in affect regulation, having the highest negative correlations with depression, anxiety, and stress [6,34]. This social perception of safeness activates psychological (e.g., compassionate mentalities and caring motives) and physiological (e.g., increased activity of vagus nerve, heightened heart rate variability, higher levels of oxytocin) mechanisms that are linked with soothing emotions [36,37].
Within the specific context of disasters and mass traumas, people have a greater propensity to affiliate and turn to others [38]. There is consistent evidence that social isolation and loneliness are linked to physical and mental health problems [39]. Findings from a cross-sectional study within a racially diverse and lower income population, during the COVID-19 pandemic peak, highlighted the importance of individual-and community-level of social support to development of depressive and anxiety symptoms [40]. Another multi-national study across 21 countries in the context of the pandemic threat showed that social connection predicted, not only post-traumatic growth, but also traumatic stress [41]. Recent research has also demonstrated that support deterioration, social rejection or isolation, and stigmatization against healthcare workers were risk factors for depression during and after the outbreak of a viral epidemic [42]. Another study found that higher levels of family and friends' support predicted fewer depressive symptoms during the COVID-19 pandemic [43]. As members of a group that has been stigmatized, the positive aspects of nurse's interactions with others are important to understand, so that factors contributing to improved functioning can be nurtured in these individuals. The documentation of potentially modifiable factors within disaster research is important to foster positive adaptation outcomes and reduce the adverse psychosocial effects of the pandemic. Additionally, the analysis of adaptation patterns in nurses and general population will enhance the clinical understanding of commonalities and specificities underlying the psychosocial interventions. Thus, the main goal of the present study is to investigate the mediating role of social connectedness on the association between COVID-19-related experiences and depressive symptomology, and to examine whether this indirect effect was conditional upon group (i.e., nurses and general population).
The present study targeted a sample of nurses and individuals from the general population, in order to compare adaptation outcomes and processes between these two groups. This research endorses the notion that global health crises may have psychosocial effects across the general population [7,9], but specially on nurses, who are directly exposed to and involved in the care of patients, working in healthcare settings that tend to face additional challenges during pandemic crises [15]. Additionally, evidence has been suggesting that social support and social connectedness play a critical role on well-being during disasters, since events that elicit chronic and/or stigmatizing stress are often followed by a depletion of support and increased levels of depressive symptoms [25,32].
Therefore, the aims for this study were defined as follows: First, to assess event centrality, social connectedness, and depressive symptoms of nurses, in comparison with the general population; and second, to examine a potential mechanism through which event centrality of COVID-19 outbreak may influence the levels of depressive symptoms, by testing social connectedness as a mediator of that relationship. Additionally, the study sought to investigate whether the indirect effect of event centrality (via social connectedness) on depressive symptoms varied by group (i.e., nurses and community subsamples).
According to these objectives, three theoretically-driven hypotheses were outlined: 1) Nurses would report higher levels of event centrality and depressive symptoms than the general population group; 2) Decreased levels of social connectedness would be observed for nurses, than for the community sample; 3) Social connectedness would mediate the association between event centrality and depressive symptoms. No predictions were made for the assessment of conditional (in)direct effects, given the absence of previous literature to devise such hypotheses.
The conceptual model of the study is presented in Figure 1.
 Figure 1: Group (Nurses vs. General population) as moderator of the mediated pathway from event centrality to depressive symptoms, via social connectedness.
View Figure 1
Figure 1: Group (Nurses vs. General population) as moderator of the mediated pathway from event centrality to depressive symptoms, via social connectedness.
View Figure 1
This study is part of a larger research project exploring the impact of COVID-19 outbreak on the mental health and wellbeing of Portuguese nurses, in comparison with the general population. For the community sample, there were two inclusion criteria to participate in this study: Age over 18 years; and being able to understand Portuguese. For nurses, a single inclusion criterion was considered: To be a nurse working in Portuguese hospitals or any other healthcare institution (e.g., primary and tertiary care). The global sample comprised 642 participants, mean age 38.1 (SD = 12.03), with 88% (n = 565) women, 11.5% (n = 74) men, and 0.5% (n = 3) non-binaries. The general population group included 326 participants and the group of nurses was composed by 316 participants. Sociodemographic and clinical information per group is available in the Results section.
All procedures were in accordance with the ethical standards of the institutional research committee, and with the Declaration of Helsinki and its later amendments for research involving human participants [44]. The study was approved by The Ethics Committee of the BLIND_FOR_REVIEW.
The research sample was recruited online, between September and December 2021, using a web-based survey (LimeSurvey®) that was shared through social and traditional media platforms and institutional emailing lists, using the non-probabilistic snowball sampling method. A protocol has been established with the Order of Nurses (and other unions), which also approved and facilitated the dissemination of this project.
The survey's first page contained the study aims, procedures and the voluntary, anonymous, and confidential nature of the participation. After reading this information, participants gave their informed consent to participate in the study (by clicking on the option "I understand and accept the conditions of the study"). No compensation was given to participants.
Sociodemographic and clinical questionnaire: This questionnaire was developed within this research project and includes questions about sociodemographic (e.g., age, gender, marital status, residence) and clinical data (e.g., psychological/psychiatric treatment history), as well as the level of exposure to COVID-19 (e.g., "Do you integrate a risk group for COVID-19?", "Were you infected with the coronavirus?", "Were you isolated from your family due to infection by the coronavirus disease?"). Nurses also answered questions about whether they treated COVID-19 patients in their professional practice and if they worked at a COVID-19 unit.
The centrality of event scale: This measure assesses the extent to which a memory of a stressful or traumatic event (in this case, participants were asked to: "Think about the COVID-19 outbreak") becomes: a) A reference point for one's personal identity (e.g., "I feel that this event has become part of my identity"); b) A turning point in one's life story (e.g., "I feel that this event has become a central part of my life story"); c) A central component for inferences and attributions in everyday life's experiences (e.g., "This event has colored the way I think and feel about other experiences"). This self-report questionnaire consists of 20 items, rated on 5-point Likert scale, ranging from 1 (totally disagree) to 5 (totally agree). The total score of the scale is calculated through the sum of its items, with higher scores indicating a higher centrality of the pandemic for individual's personal identity, life story and everyday life's experiences. In the present research, the scale revealed a high internal consistency (α = 0.95), [19,41,45].
Social safeness and pleasure scale: This instrument measures social connectedness and the extent to which individuals usually experience their social world as safe, warm, and soothing. The instrument includes 11 items, related to feelings of belonging, acceptance, and warmth from others (e.g., "I feel connected to others", "I feel a sense of belonging, "I feel a sense of warmth in my relationships with people"). Participants rate how often they feel as described in each sentence on a 5-point Likert scale from 1 (almost never) to 5 (almost all the time). Higher scores represent higher perceived social safeness and connectedness to others. In the present study, internal consistency was very good (α = 0.94), [46,47].
Overall depression severity and impairment scale: This scale evaluates the frequency and intensity of depressive symptoms and their interference with individual's life. This self-report questionnaire contains 5 questions rated on a 5-point Likert scale, ranging from 0 to 4 ("How often have you felt depressed?", "How much has depression interfered with your social life and relationships?"). It refers to an "in the past week" time frame, with higher scores indicating more frequent and severe depressive symptoms. Reliability of the scale was high within the current study (α = 0.95), [48,49].
Data analyses were conducted using Statistical Package for the Social Sciences (SPSS, version 25.0; IBM SPSS, Chicago, IL, USA) and the PROCESS computation tool (version 3.5 for SPSS; [50]). Internal consistency of questionnaires integrating the assessment protocol was measured through the calculation of their Cronbach's alphas, considering α ≥ 0.80 as optimal [51]. Descriptive statistics were obtained for all variables under study, and differences in sociodemographic and clinical variables were tested through mean differences tests (Student's t tests) or frequency differences for categorical variables (chi-square tests). To compare study variables between groups, univariate analysis of covariance (ANCOVA) was performed. Given previous reports on gender differences in the psychosocial impact of the COVID-19 pandemic [10,16], and the observed discrepancy in gender frequencies between general population and nurses (x2 = 8.36; p = 0.02), this variable was entered as covariate in univariate analyses, with only two categories (female vs. male) for these statistical analyses. Effect-size measures (partial Eta squared) were presented for the comparison analyses, considering n2p ≥ 0.01 as a small effect, n2p ≥ 0.06 as a medium effect and n2p ≥ 0.14 as a large effect [52].
Pearson's bivariate correlation coefficients were computed to assess associations between event centrality, social connectedness, and depressive symptoms, while adopting the following guidelines to classify their strength: ± 0.10- ± 0.29 (weak); ± 0.30- ± 0.49 (moderate); ± 0.50- ± 1.0 (strong) [52].
To identify potential variables that should be introduced as covariates in mediation and moderated mediation models, Pearson correlations were calculated between the dependent variable (depressive symptoms) and relevant sociodemographic variables. Psychologic/psychiatric treatment history was significantly associated with depressive symptoms (r = -0.24, p < 0.01). The association between isolation from significant others and depressive symptoms was also statistically significant (r = -0.14, p < 0.01). Regarding the core grouping variable, the correlation was statistically significant with depressive symptoms (r = 0.16, p < 0.01). Therefore, psychologic/psychiatric treatment, isolation from significant others, and group (nurses vs. general population) were controlled in the subsequent tested models.
A simple mediation model (Model 4) was performed to examine the mediating effect of social connectedness between event centrality of Covid-19 outbreak and depressive symptoms. Then, a moderated mediation model (Model 59) was tested to explore the moderating effect of group in the direct and indirect relationship between event centrality and depressive symptoms, through social connectedness [53]. The moderated mediation index was used as an indicator of the significance of the indirect effect moderation [54,55]. The statistical significance of the indirect effects was tested using a bootstrapping procedure with 5000 samples, which generated 95% bias-corrected and accelerated confidence intervals (95% BCaCIs) [56]. The indirect effect was significant when the value of zero was not contained in the confidence intervals. In addition, a standard simple slops analysis was conducted to ascertain the associations between variables for both groups separately (using Model 1 for simple moderation analyses), based on bootstrapping procedures (using 5000 bootstrap samples). Effect sizes of main, indirect and interaction effects were based on the values of R2, which were then classified as small (R2 ≥ 0.02), medium (R2 ≥ 0.13) and large (R2 ≥ 0.26) [57]. For all the analyses performed in this study, results were considered statistically significant at a p-value lower than 0.05.
The socio-demographic and clinical characteristics of the global sample and its subsamples are presented in Table 1. The total sample involved 642 participants. The general population group was composed by 326 individuals (age: M = 37.53; SD = 13.91), while the nurses group included 316 participants (age: M = 38.68; SD = 9.71). Except for age, residential area, and psychological/psychiatric treatment history, all the other variables showed statistically significant differences between both groups.
Regarding the group of nurses, the majority treated COVID-19 patients (76.9%) and 52.5% worked at a COVID-19 unit during the pandemic outbreak (Table 1).
Table 1: Socio-demographic and clinical characteristics. View Table 1
As shown in Table 2, when controlling for gender, a small, though statistically significant difference was found for event centrality (F(1.635) = 7.42, p < 0.05, n2p = 0.01), with nurses reporting the COVID-19 outbreak as a stronger reference point to their identity, when compared to the general population. Results on social connectedness and depressive symptoms indicated the absence of statistically significant differences between both groups.
Table 2: Comparison of event centrality, social connectedness, and depressive symptoms between groups. View Table 2
As presented in Table 3, all correlations were significant. For the global sample, a negative correlation was found between event centrality and social connectedness; the strength of this association was weak. For the relationship between event centrality and depressive symptoms, the correlation was positive and moderate. Finally, social connectedness correlated negatively with depressive symptoms (moderate to strong associations). The inter-correlations between study variables for each group and the global sample can be seen in Table 3.
Table 3: Descriptive statistics and matrix of inter-correlations among study variables. View Table 3
As shown in Figure 2, event centrality was negatively associated with social connectedness (b = -0.10, SE = 0.02, 95% CI = [-0.1423, -.0637]), and social connectedness was negatively related to depressive symptoms (b = -0.22, SE = 0.02, 95% CI = [-0.2506, -0.1860]). The direct effect of event centrality on depressive symptoms was significant (b = 0.07, SE = 0.01, 95% CI = [0.0509, 0.0843]). Finally, the indirect effect of event centrality on depressive symptoms was significant (b = 0.02, SE = 0.00, 95% CI = [0.0131, 0.0324]), which means that social connectedness was found to mediate the association between event centrality and depressive symptoms (Figure 2).
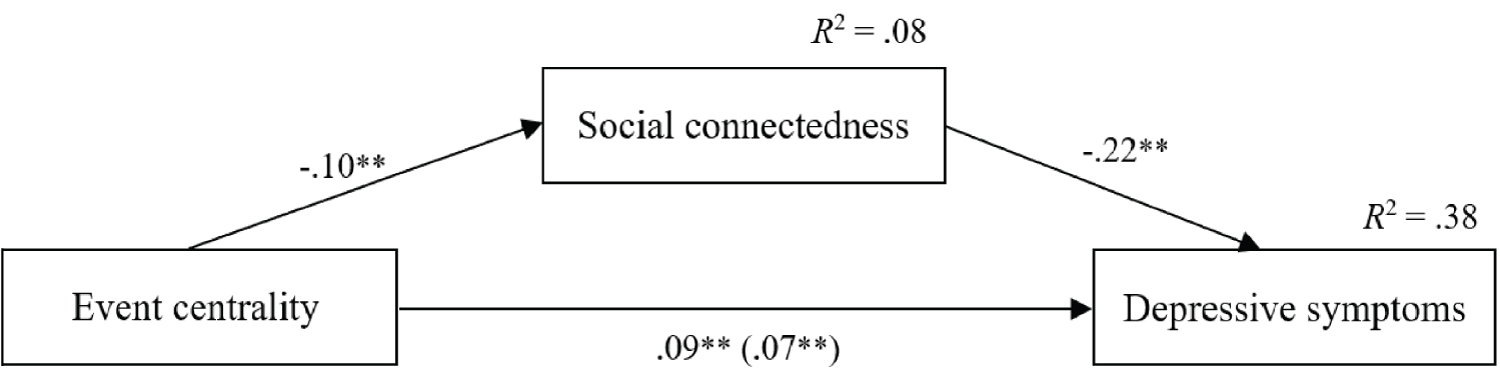 Figure 2: Simple mediation model analyzing the associations between event centrality and depressive symptomology, through social connectedness. The values shown in the arrows represent the unstandardized regression coefficients. In the paths, the value outside the parenthesis represents the total effect of event centrality on depressive symptoms. The value inside the parenthesis refers to the direct effect after the inclusion of the mediating variable. Measurement errors and covariates were omitted to facilitate reading, **p < 0.01.
View Figure 2
Figure 2: Simple mediation model analyzing the associations between event centrality and depressive symptomology, through social connectedness. The values shown in the arrows represent the unstandardized regression coefficients. In the paths, the value outside the parenthesis represents the total effect of event centrality on depressive symptoms. The value inside the parenthesis refers to the direct effect after the inclusion of the mediating variable. Measurement errors and covariates were omitted to facilitate reading, **p < 0.01.
View Figure 2
Following the examination of a moderated mediation model (Figure 1), the obtained results showed that group (nurses vs. general population) moderated the relationship between event centrality and depressive symptoms, as well as the association between social connectedness and depressive symptoms. The interaction between event centrality and group did not have a significant predictive effect on social connectedness (b = 0.02, SE = 0.04, 95% CI = [-0.0598, 0.0967]). However, it had a marginally significant effect on depressive symptoms (b = -0.03, SE = 0.02, 95% CI = [-0.0664, 0.0003]). The interaction between social connectedness and group had a significant predictive effect on depressive symptoms (b = -0.07, SE = 0.03, 95% CI = [-0.1384, -0.0103]).
Post-hoc analyses were conducted to ascertain the moderating effects of group (Nurses vs. General population) described above. Firstly, the simple effects of event centrality on depressive symptoms were examined; and secondly, it was investigated the association between social connectedness and depressive symptoms. As shown in Figure 3, simple slope analysis showed that the association between event centrality and depressive symptoms was positive for both groups, but stronger for the general population (b = 0.08, t = 0.01, p < 0.001) than for nurses (b = 0.05, t = 0.01, p < 0.001). According to Figure 4, depressive symptoms decreased as social connectedness increased for both groups, although the association was stronger for nurses (b = -0.25, t = 0.02, p < 0.001) than for the general population (b = -0.18, t = 0.02, p < 0.001).
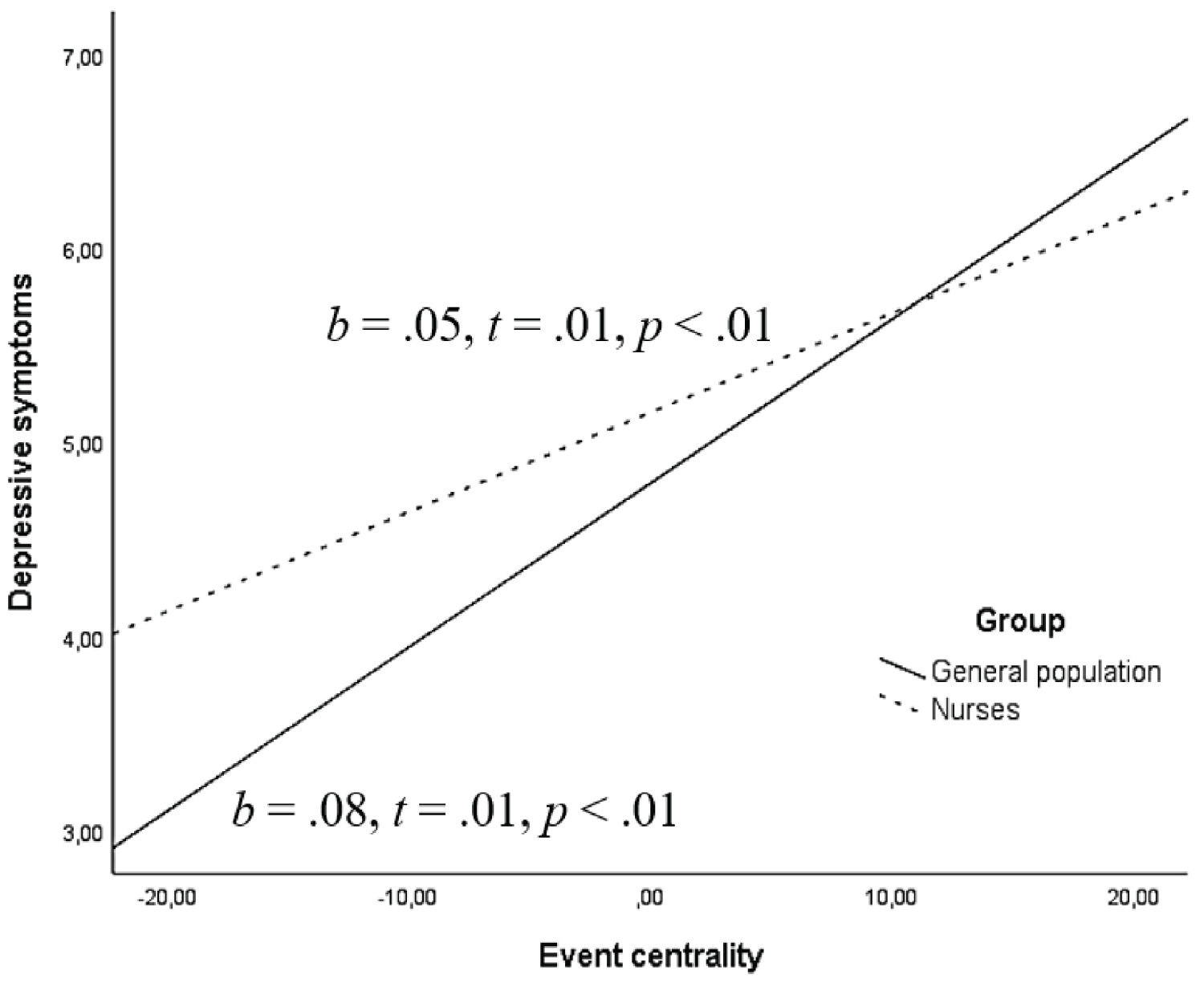 Figure 3: The moderating effect of group on the association between event centrality and depressive symptoms.
View Figure 3
Figure 3: The moderating effect of group on the association between event centrality and depressive symptoms.
View Figure 3
When analyzing the indirect effect of event centrality on depressive symptoms, as presented in Table 4, results indicated that social connectedness was a significant mediator for nurses (b = 0.02, SE = 0.01, 95% CI: [0.0086, 0.0396]), as well as for the general population(b = 0.02, SE = 0.01, 95% CI: [0.0093, 0.0330]). Finally, the index of moderated mediation was not statistically significant (b = 0.00, SE = 0.01, 95% CI: [-0.0162, 0.0227]), suggesting at the indirect effect of event centrality on depressive symptoms through social connectedness was not conditional upon group (Figure 3, Figure 4 and Table 4).
 Figure 4: The moderating effect of group in the association between social connectedness and depressive symptoms.
View Figure 4
Figure 4: The moderating effect of group in the association between social connectedness and depressive symptoms.
View Figure 4
Table 4: Conditional indirect effects of event centrality, via social connectedness, on depressive symptoms. View Table 4
To the best of our knowledge, this is the first study to investigate the role of social connectedness on the association between centrality of COVID-19 outbreak and depressive symptomatology, and whether this effect was invariant across groups (i.e., nurses and general population). The present research gathered evidence for a potential mechanism linking event centrality to depressive symptoms within the context of the COVID-19 pandemic outbreak.
Main findings may be summarized as follows: First, nurses perceived the COVID-19 outbreak as a stronger reference point to their identity than the general population; second, there were no significant differences in the levels of social connectedness and depressive symptoms between those two groups; third, social connectedness was found to mediate the association between event centrality and depressive symptoms; and finally, the in direct effect of the event centrality on depressive symptoms, through social connectedness, was not conditional upon group.
When compared to the general population, nurses reported higher levels of event centrality. Although this difference was small, these results confirm our first hypothesis and demonstrate that those who were directly and repeatedly exposed to the coronavirus appraised the pandemic as more central to their identity and life story. Despite the restrictive measures imposed to control the spread of the virus, nurses had to continue to perform their jobs uninterruptedly, coping with the additional challenges of a world-wide health emergency besides the usual workplace stressors [17]. Their daily routines were severely disrupted, and self-identity was narrowed to their occupational role, thus making the pandemic a well-remembered, vivid, intense, and easily accessible personal memory. This finding suggests that addressing the importance of this global crisis to one's identity and life story can be a salient target in preventive and therapeutic interventions for nurses, during and in the aftermath of the COVID-19 pandemic.
Contrary to our second hypothesis, and challenging previous reports [11-13], there were no significant differences in social connectedness and depressive symptoms between nurses and the general population. This unexpected result emphasizes the substantial and enduring effects of the COVID-19 on mental health and well-being of the whole population, regardless of the group under study. A key factor available to nurses that might justify the reports of social connectedness was interpersonal support among colleagues, which is associated with a sense of belonging, shared identity, and affiliation with the group [58]. On the other hand, physical distancing was the most recommended measure to reduce transmission rates of the virus, in addition to routine hygiene practices (e.g., hands washing, mask use) [4]. General population was confined to their houses and universally recommended to restrict social interactions, thus experiencing deterioration of a sense of social embeddedness [59].
Regarding depressive symptoms, we found similar prevalence of depressive symptoms among nurses and the general population. Previous studies on the context of COVID-19 have shown some inconsistency on the comparison of the mental health status of both groups, remaining unclear which one presents higher rates of depressive symptoms [5,17]. In fact, the whole world has been facing an unprecedented situation. People of all ages and social status were confronted with critical life changes, being compelled to adopt pandemic-control measures (e.g., stay-at-home orders, conditioned exits even for physical exercise, working from home) that emphasized isolation and inactivity. Accordingly, feelings of despair, boredom, frustration, and states of hopelessness and helplessness-which are typical of depressive reactions and disorders-have been frequently reported during the COVID-19 [4]. Noteworthy, many people were exposed to repetitive and dramatic information about the pandemic through media coverage of events, which could have contributed to negative psychological outcomes [60]. In contrast, despite their unique experience of healthcare-related stress, nurses were required to keep on the "doing" mode, with all the workload to manage, and less time to additional sources of exposure to stress, such as media consumption. Also, nurses are more knowledgeable about the disease than the general population, and thus less permeable to misinformation and fake news [61]. Finally, nurses may be better prepared to face extreme stressful situations and to cope with adversity, being able to integrate their experience more efficiently. The consistency between their behavioral pattern and their own intrinsic vocational motivations, values, and goals might protect their own psychological health [62].
As for the third hypothesis, we found support for a mediation model in which the association between event centrality and depressive symptoms was mediated by social connectedness. First, there was a direct positive association between event centrality and depressive symptoms, corroborating that the degree to which the pandemic outbreak was perceived as an anchor point to personal narratives plays an important role in the development of depression symptoms [16]. In fact, the outbreak of COVID-19 may shape one's sense of self, mold meaning attribution to past, present, and future events, and structure life narrative. The event centrality may block access to new information unrelated to the pandemic, which might create a vicious cycle, thus explaining the development of depressive symptoms [63].
Moreover, event centrality was indirectly linked to depressive symptoms through social connectedness. When the COVID-19 outbreak became integrated as key to how one understands oneself and the world, it formed a highly accessible and interconnected reference point that could be related to the deterioration of social ties (e.g., isolation, heightened social anxiety, social unskillfulness), thus exacerbating depressive symptoms. Altogether, the present results offer additional support for the mediating effect of social connectedness between chronic, traumatizing and/or stigmatizing stressful events and depressive symptomatology [64]. The enduring manifestation of the stressful event tends to deplete emotional and tangible resources (e.g., social ties), impairing feelings of closeness, safeness, and affection to others and influencing psychosocial adaptation process. As we know from previous literature [6,34], individuals who experience their social world as less warm, kind, and supportive tend to be more prone to develop psychopathological symptoms, namely depression.
When analyzing the conditional effects within the mediation model under examination, centrality of the pandemic outbreak was positively correlated with depressive symptomatology for the global sample, but this association was stronger for the general population. The diminished strength of the association for nurses may be related to the potential desensitization to the virus-related fears, due to the constant exposure to those who are seriously ill and/or dying. Social connectedness was negatively correlated with depressive symptoms in both groups, although the strength of this association was higher for nursing professionals. Given the extreme pressure, work-family conflict, and emotional issues that nurses have been facing since the beginning of the COVID-19 outbreak, relying on supportive and caring relationships maybe particularly significant for them to mitigate the deleterious effect of the pandemic on mental health, through the activation of the soothing-affiliation system in affect regulation processes [6,34].
Finally, the indirect effect of event centrality, via social connectedness, on depressive symptoms was not conditional upon group, thus suggesting the applicability of the mediation model to nurses and the general population. This result suggests that greater event centrality of the COVID-19 outbreak may induce deterioration of social connectedness, which in turn leads to higher levels of depressive symptoms. Despite the specific challenges faced by both groups due to the pandemic, our findings indicate that event centrality may have a significant impact on the depressive symptoms of nurses and the general population through a common potential mechanism. In fact, mobilizing emotional and practical support and fostering safe interactions seem to play an important role in affect regulation, especially in the context of a life-threatening situation, promoting affiliative and prosocial processing and toning down threat focus [6].
The current study has important implications for clinical practice and health policy. First, it would be valuable to implement interventions aimed at determining the centrality of the COVID-19 outbreak and encouraging new perspectives, particularly in the general population. Examining the impact of this global health crisis to identity and life story is of paramount importance to prevent and reduce depressive symptoms. Besides, creating a coherent narrative about the experience can be crucial to highlight memories that are congruent with one's own values and goals [65].
Second, findings from this research suggest that cultivating feelings of social safeness and connectedness, especially in nurses, may improve mental health outcomes, namely depressive symptoms. Since health care workers are frequently reluctant to ask for support [58], it would be very important that organizations cultivate a safe work environment, creating the structural conditions for nurturing peer support. Additionally, team leaders should be mindful of specific pandemic-related fears, difficulties and needs of healthcare workers, to facilitate the nursing team's adjustment processes.
Third, training people to develop compassionate mentalities and caring motives can mitigate the effects of event centrality and thus reduce depressive symptoms, for both the general population and nurses. This is to say that the cultivation of a sense of social connectedness and safeness may attenuate the deleterious effects of traumatic appraisals on the development and maintenance of depressive symptoms. Accordingly, compassion-based interventions (e.g., compassionate mind training, mindful self-compassion) have been found to reduce depression and anxiety, and increase well-being [66].
Despite the contributions of the present study, a few limitations should be noted. First, its cross-sectional design constitutes one of its main shortcomings, preventing the establishment of causal relationships between variables. Second, data were collected during a specific period of the pandemic, which may not be generalizable to other times of this ever-changing health crisis. Third, the sampling frame relied exclusively on online procedures, thus excluding those individuals with the lowest levels of digital literacy, and those who, through lack of interest or opportunity, do not use social media at all. Fourth, our study's sample was embedded in the Western European cultural context, which may impair its external validity by limiting the generalizability of findings. Furthermore, the retrospective assessment of the experience may be subject to recall bias. Given the profound effects of the COVID-19 pandemic on the entire population, individual's perceptions of the event are more likely to have been influenced by many factors (e.g., social interactions, media exposure, infection), thus reducing the accuracy of collected data. Another limitation relates to the fact that data were exclusively collected through self-report measures, as some individuals may not have complete awareness of their emotional responses, thus reducing the accuracy of such reports; moreover, self-reports may be easily affected by social desirability factors and not fully reflect what participants actually feel, think or do.
Future studies should longitudinally analyze the proposed mediational model, not only to substantiate the findings from cross-sectional research, but also to elucidate (mal)adjustment trajectories across time. Second, it would be valuable to assess the effects of compassion-based interventions on decreasing depressive symptoms and mitigating the impact of the centrality of a traumatic event, especially in nurses. In addition, future research could address other outcomes frequently co-occurring with depression (e.g., anxiety, PTSD symptoms), as well as other cognitive-interpersonal mediators (e.g., specific social support provisions, family environment/functioning), seeking to refine a model linking health pandemics appraisals to individual's mental health outcomes. Finally, the overall applicability of the proposed model could be ascertained across different at-risk populations (e.g., healthcare workers in general, COVID-19 patients, socially marginalized groups).
The current study sheds light on the urgency of advocating for a culture of interdependence, through the cultivation of a sense of social safeness and connection to others. Given that human beings are not islands, but peninsulas instead, it is crucial to foster warm, kind relationships, to counteract the harmful effects of the COVID-19 pandemic on mental health, especially for nurses, who experienced traumatic levels of event centrality related to the COVID-19 outbreak.
This study was supported by the Center for Research in Neuropsychology and Cognitive-Behavioral Intervention (CINEICC)-University of Coimbra (UIDB/PSI/00730/2020), and by a doctoral grant (2020.07981.BD) awarded to the first author (Portuguese Foundation for Science and Technology/MCTES). The authors thank all the participants in this study for their contribution, and are especially grateful to the Portuguese Order of Nurses and to the Nursing Schools of Coimbra and Lisbon, for their assistance in the collection of the sample of nurses.
None.
The data that support the findings of this study are available from the corresponding author, upon reasonable request. We have no known conflict of interest to disclosure.
Catarina Vitorino and Carlos Carona: Conceptualization and drafting of the article, data collection and data analysis; Maria Cristina Canavarro: Formulation of research goals and aims, critical review of the manuscript.