To determine the psychosocial impact of Rosacea on Women QOL (Quality of life) and female self-esteem.
We conducted a cross-sectional paper based survey at New Cross Hospital, Wolverhampton, United Kingdom from January to June 2019.
42% of the female patients used makeup "all the time" to cover the rosacea. Correlation Coefficient (r) between the two variables (Rosenberg Self Esteem Score (RSES) and Function score) was noted to be -0.78. 53% of the patients were noted to experience frustration "all the time" as a result of rosacea.
Results from this study highlight the psychosocial burden of Rosacea on female population and the need to recognize the importance of cosmetic camouflage and psychological intervention as part of treatment for rosacea in women.
Rosacea, Female, Psychosocial
RosaQOL: Rosacea specific Quality of Life; RSES: Rosenberg Self Esteem Score
Rosacea is a common, chronic, relapsing inflammatory skin condition that affects blood vessels and pilosebaceous units [1]. The main features of rosacea are persistent central facial erythema, flushing, telangiectasia, inflammatory papules and pustules, skin thickening and ocular symptoms [2]. Based on these complex characteristics, National Rosacea Society Expert Committee [3] has classified rosacea into four different subtypes: Papulopustular erythematotelangiectatic, phymatous and ocular. The etiology of rosacea is still poorly understood. However, familial history and genetics [4] are found to have been a potential causative factor of rosacea. Rosacea is also known to have a profound impact on patients' psychosocial wellbeing.
Psychosocial distress, in patients with rosacea, stems from stigma of self-perception as well as public perception. Patients often scrutinize on visible skin changes and identify it as a cosmetic disfigurement, which in turn affects their self-esteem [5]. This leads to depression, anxiety and severe emotional distress [6]. The embarrassment and dissatisfaction caused by their facial appearance leads to social isolation [7]. This in turn has a detrimental impact on patients' quality of life as they become deprived of social opportunities. This significant psychosocial burden produced by rosacea also plays a role in triggering flare-up of the disease, causing a vicious cycle [8].
Rosacea is found in approximately 10% of the general population and is known to mainly affect people from 30 to 60 years of age. It is more prevalent in female population as opposed to male population (with the exception of phymatous rosacea where majority of affected patients are adult male). A 2012 study consisting of 60,042 patients in the United Kingdom identified that 61.5% of patients with rosacea was female [9]. Further studies suggest that rosacea has a greater impact on quality of life of female population compared to male, as female are more prone to distorted perceptions of their body image [8]. Despite the higher prevalence of rosacea in women, there is a paucity of studies that focus on the psychosocial stressors on women as a result of this condition.
Educating female patients and creating awareness that rosacea is a controllable disease would help mitigate the negative psychological effect of the disease. The lack of patient awareness is mainly due to the fact that the psychosocial impact of this condition has been underestimated and overlooked by dermatologists [10]. It is important for dermatologists to recognize that rosacea is not just a cosmetic affliction but could also psychologically affect patients. Understanding the psychosocial domains of rosacea can help in formulating a more holistically therapeutic treatment plan that can be tailored to each patient. This study aims to highlight the importance of treating rosacea in women not just from a medical, but also from a psychosocial perspective.
This is a cross-sectional paper-based survey conducted with female patients who have experienced rosacea for at least five years at the dermatology outpatient department at New Cross Hospital in Wolverhampton, United Kingdom from January to June 2019. This survey screened for psychosocial effect of rosacea on female adults and captured data on clinical features as well psychosocial effects of rosacea in women. Clinical experts have contributed to this RosaQoL, which is 5-point, 21-item likert scale questionnaire that targets the various psychosocial domains of Rosacea. Rosenberg Self Esteem Scale (RSES) Questionnaire has also been adapted for use in this research.
The potential for ethical issues for this questionnaire was taken into consideration. Patients were provided with an information leaflet before participation and the authors identified no concerns.
A total of 19 female patients voluntarily participated in this survey. Out of the 19 patients who responded to the questionnaire, 13 patients were between 41-50, making up the majority of the sample population. 5 of the patients were under the category of 51-60 and one patient was more than 61.
Rosenberg 1965 Self Esteem Scale (RSES) Questionnaire was used to assess the self-esteem of the female patients affected by rosacea. Responses were scaled on a 4-point likert scale (Strongly Disagree, Disagree, Agree, Strongly Agree). It is a 10-item uni-dimensional scale that measures global self-worth by measuring both positive, negative thoughts and self-perception. We had to take into consideration that certain items on the Rosenberg questionnaire (Questions 2, 5, 6, 8, 9) were reverse scored [11]. Score were kept on a continuous scale and ranged from 0-40, 40 indicating the highest possible score.
Rosacea related quality of life was assessed using the Rosacea specific Quality of Life (RosaQOL) questionnaire [10]. It is a 21-item likert scale that evaluated the impact of rosacea on the quality of life of patients across three main domains-Emotion, symptom and function. The score of each RosaQoL questionnaire was the average of the responses to the 21 items. The answers to the items were "never", "rarely", "sometimes", "often" and "always". Responses were recorded on the scale of 1 (never) to 5 (always). It is important to note that the RosaQoL score is inversely related to the quality of life. The higher the score, the worse one's quality of life and lower score indicates a better quality of life.
1. Age range: Divided into three groups- 41-50, 51-60, > 61.
2. Female patients who have had rosacea > 5 years.
1. Patients who did not complete the entire questionnaire.
2. Patients who have been diagnosed and treated for rosacea for < 5 years.
Descriptive statistics have been used to describe survey data with Microsoft Excel. The data was then collated and entered into a spreadsheet ready for analysis. RosaQOL and Rosenberg 1965 Self-Esteem questionnaire were scored based on the guidelines set by the instrument developing committee. For categorical variables, frequencies, mean, mode and median have been reported. Descriptive statistics were reported for scale scores in the sample population.
A total of 19 patients were involved in this study. The final sample obtained fulfilled the criteria of age and duration the patient has been experiencing rosacea for. These are patients who are under the care of dermatologists at the New Cross Hospital and obtaining medical treatment. Results of the pooled survey are described in the results section in this paper.
Out of the 19 patients who responded to the questionnaire, 13 patients were between 41-50, making up the majority of the sample population. 5 of the sample fell into the category of 51-60 and one patient was more than 61 (Table 1).
Table 1: Table illustrating age range, Rosenberg self-esteem score and function score of patients. View Table 1
Cosmetic camouflage was noted to be one of the popular coping mechanisms amongst female patients. 42% of the female patients used makeup "all the time" to cover the rosacea. 26% reported to have used it "often" while the remaining 32% of the sample population used cosmetic products to cover up their rosacea "sometimes" as illustrated by Figure 1. None of the patients (n = 0) reported to have never or rarely used any form of cosmetic camouflage.
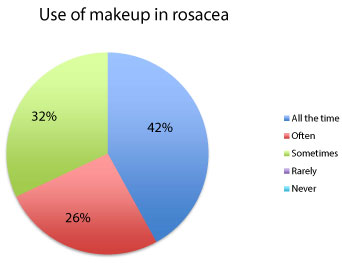 Figure 1: Pie chart illustrating percentage of patients using makeup. View Figure 1
Figure 1: Pie chart illustrating percentage of patients using makeup. View Figure 1
Furthermore, 11% of the sample population was noted to avoid certain environment and food products all the time as part of coping mechanism to deal with rosacea.
Pearson's Correlation Coefficient (r) between the two variables (Rosenberg Score and Function score) was noted to be -0.78. This was calculated on Microsoft Excel. A correlation of -0.78 indicates a strong negative linear relationship between the two sets of data (Figure 2). In other words, there is a strong association between self-esteem score and the function domain score. A negative linear relationship indicates that the higher the self-esteem of the patient, the less likely to use coping mechanisms such as makeup and avoiding triggers of rosacea.
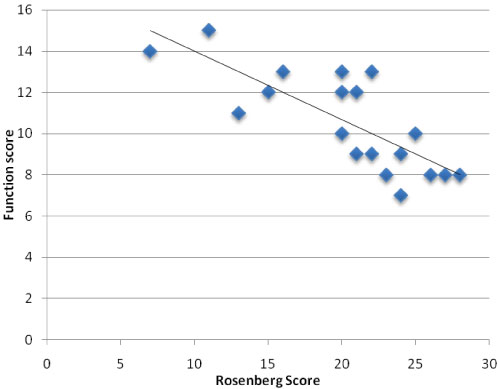 Figure 2: Pie chart illustrating percentage of patients using makeup. View Figure 2
Figure 2: Pie chart illustrating percentage of patients using makeup. View Figure 2
Standard deviation of 2.32 in the function domain of the RosaQOL indicates that the individual scores tend to be close to the mean score (10.58). The maximum score of the function domain is 15. The median was noted to be 10. Higher score in this domain indicates increased use of coping mechanisms such as makeup, avoiding food or certain environment. On the other hand, Rosenberg self-esteem scale had a higher standard deviation (5.42), which indicates the wider range of self-esteem scores in the population (Table 2).
Table 2: Function Domain score of RosaQOL and Rosenberg Self-Esteem Scale score. View Table 2
Clinical characteristics are described in Table 3. More than half of the sample population (53%) report that they often experience discomfort as a result of stinging or burning of skin from rosacea at the point of survey completion (Table 3). Mode and median is noted to be "often", which indicates that burning and stinging of skin in rosacea is noted to be the most prominent symptom experienced by the female patients.
Table 3: Clinical characteristics of rosacea (Symptom Domain). View Table 3
21% of the patients report that they experience skin flushing all the time. In terms of ocular symptoms, a very small proportion of the female patients (5%) experienced it all the time. 42% of the survey population reported to have not had ocular symptoms at all. A smaller proportion of patients noted to have rarely experienced ocular symptoms (Blepharitis, conjunctivitis, dryness, itching, light sensitivity, blurred vision and telangiectasia of the conjunctiva or eyelids).
A huge proportion of participants (53%) were noted to experience frustration all the time as a result of rosacea. 32% of the sample reported to feel frustrated "often". A smaller proportion of the sample (15%) experienced this "sometimes". 37% of the population reported to be embarrassed of their skin condition "all the time". Similar proportion (37%) of the population noted to be embarrassed of their rosacea "often". It is also important to note that none of the participants reported to have "rarely" or "never" experienced both frustration and embarrassment (Figure 3).
 Figure 3: Bar chart showing the percentage of rosacea that experienced embarrassment and frustration. View Figure 3
Figure 3: Bar chart showing the percentage of rosacea that experienced embarrassment and frustration. View Figure 3
53% of the female patients reported to be mentally pre-occupied by rosacea "all the time". 32% of the patients "often" thought about their condition. 37% of the sample was bothered "all the time" by the reoccurrence of their rosacea. 53% of the population was "often" bothered by the reoccurrence of rosacea (Table 4). None of the sample population noted to be "rarely" or never" bothered by the reoccurrence of rosacea. This indicates that female patients are constantly mentally occupied with thoughts of their rosacea and also worry about the relapse of the condition.
Table 4: Table illustration of Emotional Domain of RosaQOL (Emotional Domain). View Table 4
Currently, there is no specific literature focused on the psychosocial impact of rosacea in female population. This is the first cross-sectional survey based study on the psychosocial effect of rosacea on women, mainly focused on self esteem and the three main domains of RosaQOL (Symptom, Function and Emotional Domain). This study serves as a good foundation to explore the link between the self-esteem of the female patients affected by rosacea and their coping mechanisms to deal with the symptoms as well as the consequences of the disease.
This current study highlights that rosacea has a huge psychosocial effect on women and is also found to hugely affect self-esteem as proven by the Rosenberg scale scores. Moustafa, et al. noted in a 2014 review that patients with rosacea have higher incidences of embarrassment, social anxiety and reduced quality of life compared to the general population [12]. Another study done by National Rosacea Society involving more than 400 patients with rosacea concluded that 75% of respondents reported that their rosacea had an adverse impact on their self-esteem [9] .It was also reported that the patients were embarrassed (70%) and frustrated (69%) of their skin condition [9]. This is consistent with the findings from this current study in which all the patients experienced embarrassment and frustration to a certain degree.
Data from this current survey corroborated that the use of cosmetic camouflage is a commonly used coping mechanism and technique to cover up rosacea. This is highly relevant in the female population, given that women are the main consumers of cosmetic industry. These findings are supported by previous literature. Seite S, et al. suggest that dermatologists should encourage patients with disfiguring lesions to utilize appropriate and safe makeup to improve their appearance and their quality of life [13]. It suggests that corrective makeup can also complement the treatment of face dermatological diseases in order to improve patient's adherence. A 2018 German study suggests that green-tinted skin care creams or make up is suitable to conceal erythematous patches of rosacea and this will improve quality of life [14]. Furthermore, Kent noted in a study that cosmetic camouflage worked in boosting confidence, but did not play any role in changing the underlying negative cognitive processes or beliefs [15]. Thompson, et al. also noted in a 2017 qualitative study that patients were unable to interact confidently in social situations without any cosmetic camouflage, as it played a huge role in boosting self-esteem [16]. This is in line with the findings of the current study in which use of cosmetic camouflage did not help eliminate the negative feelings such as embarrassment and frustration.
The female participants in this study had consistently high scores in RosaQoL across all three domains- Emotion, Function and Symptoms. This highlights the overall negative impact rosacea has on female patients' quality of life. University of Sheffield, United Kingdom conducted a 2017 qualitative study that focused predominantly on female population with rosacea [16]. This study noted that emotion focused and avoidant focused strategies helped to boost confidence in social situations but failed to address the underlying negative cognitive factors that contributed to psychological distress in patients. It emphasizes the need to identify patients who will benefit from being referred for psychological support [16].
This current study has been uniquely designed to focus only on female population affected by rosacea given that psychosocial impact on women has not been extensively studied. This unique feature of the study allows the clinical symptoms, emotional and psychological burden of rosacea to be evaluated further, giving way for future research as well as management tailored to women.
However, there are certain limitations identified in this study. Given the small sample size, it may affect the reliability of a survey's results because it leads to a higher variability that causes biasness. Furthermore, a small sample size is noted to be decreasingly representative of the wider population. Therefore, there is a need to purposively seek male respondents as well in the future study.
Conclusively, the psychosocial impact of rosacea on women is a topic that has been understudied in literature. The findings from this current study highlights the impact rosacea has on female population. This will help dermatologists identify and gain a better understanding on the psychosocial burden imposed by rosacea on women.
These results from the study also shed greater light on the various coping mechanisms used amongst female patients affected by rosacea. Given that cosmetic camouflage has been noted to be one of the most commonly used coping method, it will be worth doing further research on the specific cosmetic products for female patients. This highlights the need for dermatologists and patients to understand the type of cosmetic products available in the industry which best suits the skin of patients affected by rosacea. Furthermore, makeup professionals in collaboration with dermatologists could run training workshops and distribute handouts focused on use of cosmetics in rosacea-affected skin. This could be targeted at female patients with a view of improving psychosocial outcomes.
Given that female patients affected by rosacea are vulnerable to the multifaceted impact of rosacea despite cosmetic measures, it is important that dermatologists collaborate with mental health professionals so as to identify the specific psychological needs of the female patient and tailor their treatment accordingly.
This study is an initial step in identifying the psychosocial burden specifically in the female population. Research focused on male population affected by rosacea is currently ongoing. Future research on rosacea should instead focus on the need for multi-disciplinary approach towards treating rosacea in both genders.
An informed consent was obtained from all the patients participating in the survey.
The authors declare that they have no conflict of interests.