Pemphigoid, Pemphigoid gestationis, Herpes gestationis
Pemphigoid gestationis is a rare autoimmune vesiculobullous disease that occurs during pregnancy or postpartum. It is caused by circulating IgG autoantibodies that target the extracellular non-collagenous domain of the hemidesmosomal protein BP180. Urticarial papules and plaques with posterior development of tense vesicles and bullae with an erythematous background are the hallmark of the disease. It affects both primigravidas and multigravidas and can occur in any trimester or postpartum but presents most often in the second or third trimester [1]. Sporadically it can occur as a paraneoplastic manifestation in women with trophoblastic tumors or molar pregnancies [2]. The diagnosis is based on compatible skin lesions, a positive direct immunofluorescence and compatible histopathological findings. Correct recognition and differentiation from similar diagnoses is critical due to potential risk for the fetus, which can be lowered with adequate treatment. Herein, we report a case of a third-trimester gestational pemphigoid in a multigravida.
A 29-year-old female presented to our clinic with a twenty-five-day history of skin lesions. Initially, she noticed erythema and highly-pruriginous bullous lesions in her abdomen with associated desquamation. Extension to her back, upper and lower extremities was noted sequentially. The patient was 30 weeks pregnant and had two other children. Her past pregnancies had been normal.
Skin examination revealed multiple, disseminated, symmetrical and sharply defined 0.5-1.5 cm urticarial plaques, erythematous erosions and clear fluid-containing tense vesicles and bullae (Figure 1). They coalesced in plaques and affected the abdomen, inguinal folds and upper and lower extremities. The umbilicus was relatively spared (Figures 2, Figure 3 and Figure 4). Hair and nails were unaffected.
 Figure 1: (a) Tense bullae; (b) Urticarial plaques apparent on upper extremities.
View Figure 1
Figure 1: (a) Tense bullae; (b) Urticarial plaques apparent on upper extremities.
View Figure 1
 Figure 2: (a) Multiple, disseminated, symmetrical and sharply defined 0.5-1.5 cm erythematous erosions and clear fluid-containing vesicles and bullae; (b) Post-treatment.
View Figure 2
Figure 2: (a) Multiple, disseminated, symmetrical and sharply defined 0.5-1.5 cm erythematous erosions and clear fluid-containing vesicles and bullae; (b) Post-treatment.
View Figure 2
 Figure 3: (a) Affection of the anterior thorax; (b) Post-treatment.
View Figure 3
Figure 3: (a) Affection of the anterior thorax; (b) Post-treatment.
View Figure 3
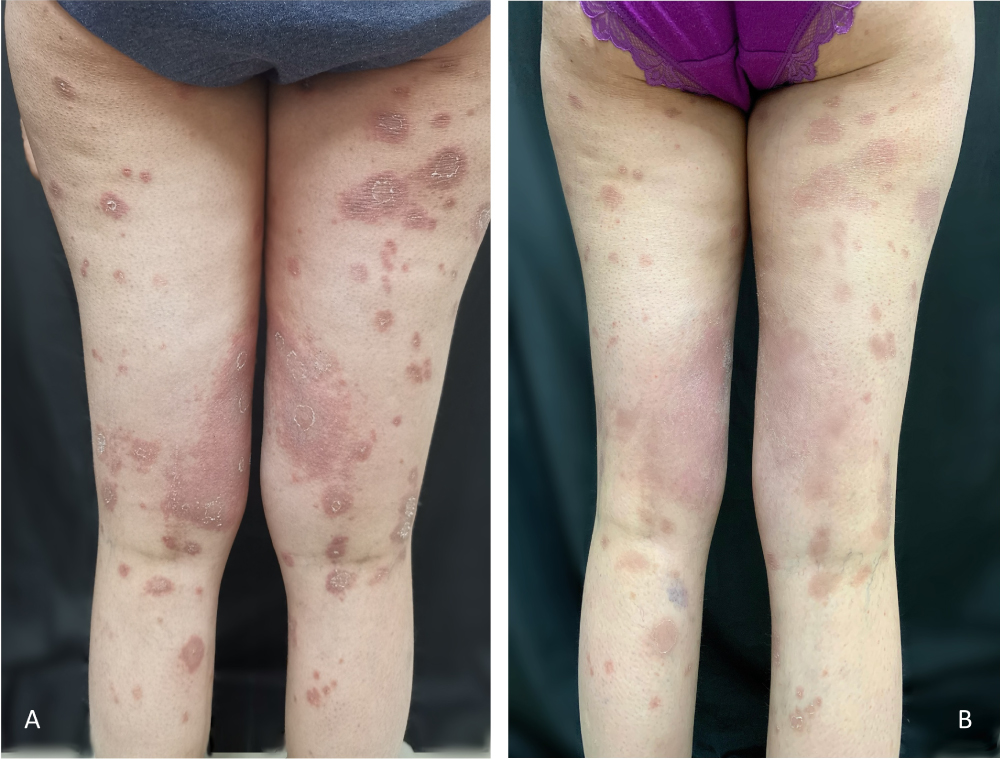 Figure 4: (a) Affection of the lower extremities; (b) Post-treatment.
View Figure 4
Figure 4: (a) Affection of the lower extremities; (b) Post-treatment.
View Figure 4
Work up included a complete blood count, serum electrolytes, renal and hepatic profile which demonstrated normal results. Two incisional biopsies were taken for histopathological and direct immunofluorescence analysis. The hematoxylin and eosin staining revealed a subepidermal bullae with abundant eosinofil-rich infiltrate, perivascular infiltrate and mild basal spongiosis (Figure 5). The direct immunofluorescence revealed linear and fibrillar C3 and IgG deposits along the basement membrane (Figure 6).
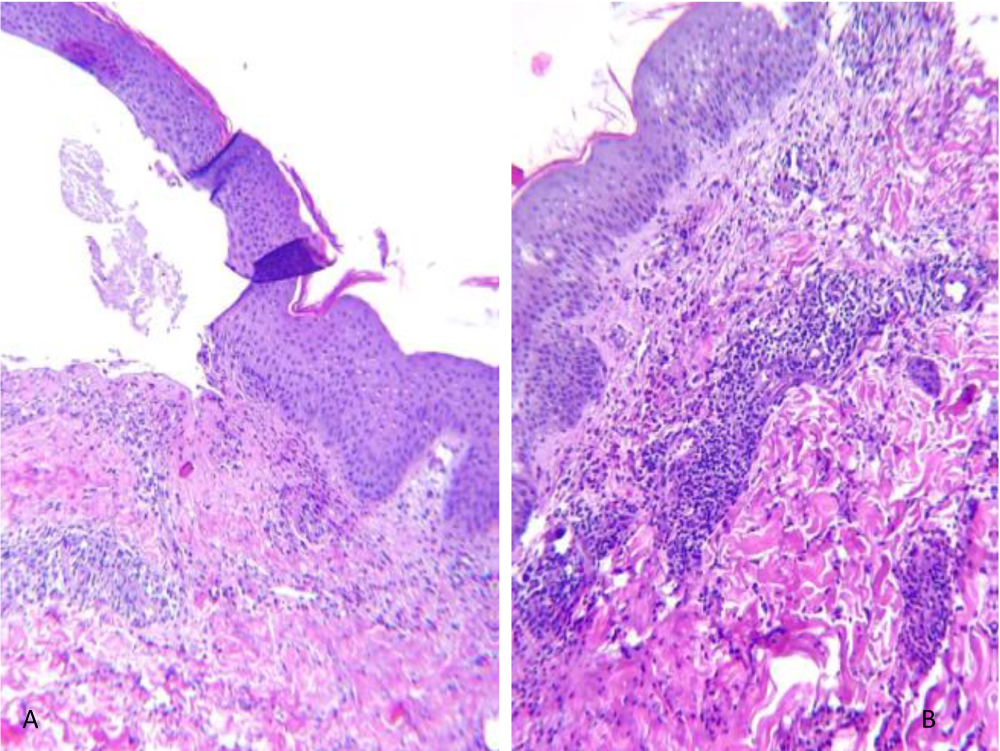 Figure 5: (a) Histopathological findings: Subepidermal bullae with abundant eosinophil-rich infiltrate; (b) Histopathological findings: Perivascular infiltrate and mild basal spongiosis.
View Figure 5
Figure 5: (a) Histopathological findings: Subepidermal bullae with abundant eosinophil-rich infiltrate; (b) Histopathological findings: Perivascular infiltrate and mild basal spongiosis.
View Figure 5
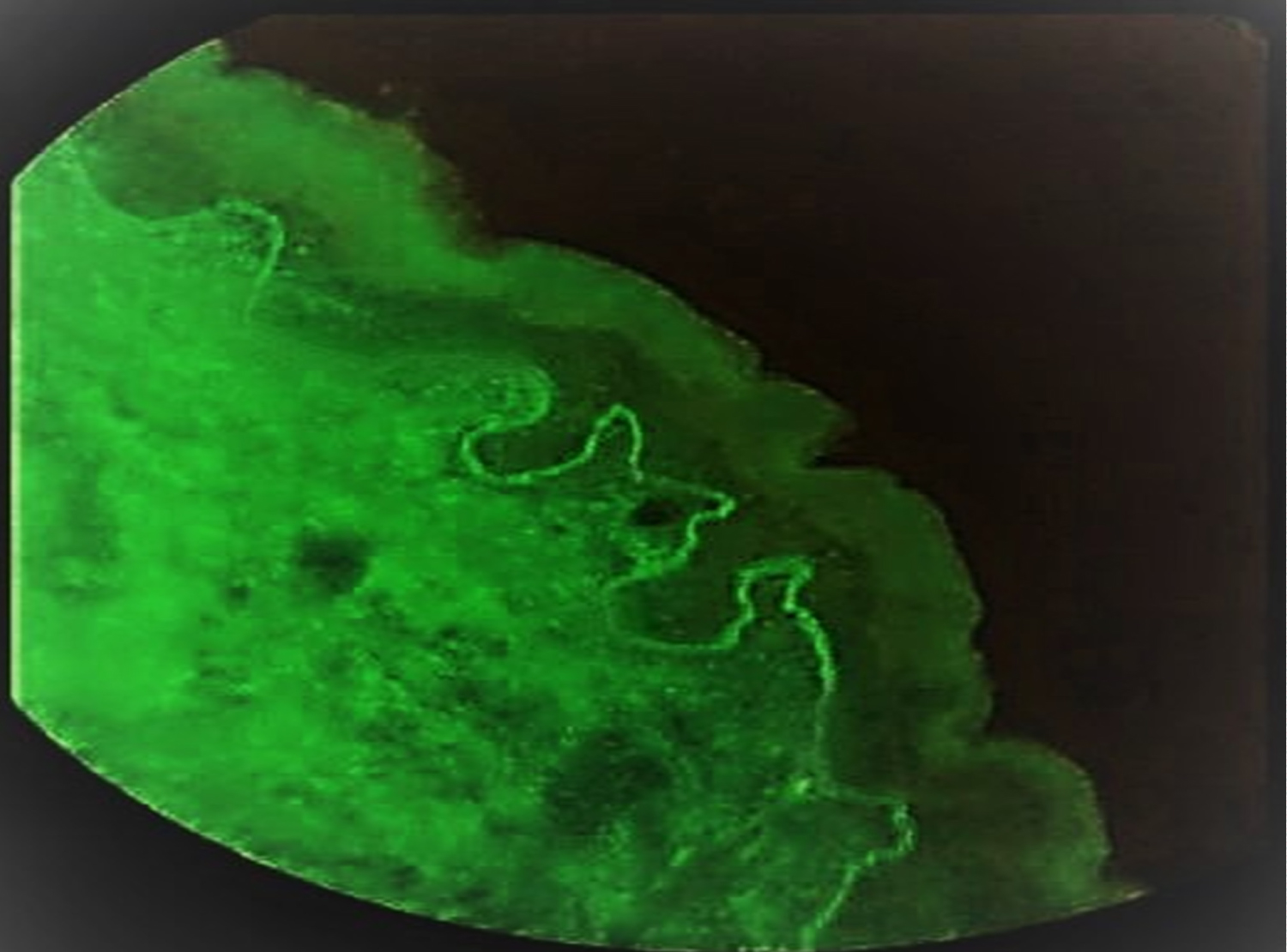 Figure 6: Direct immunofluorescence showing linear positivity of IgG in basement membrane.
View Figure 6
Figure 6: Direct immunofluorescence showing linear positivity of IgG in basement membrane.
View Figure 6
She was diagnosed with pemphigoid gestationis and treated with Prednisone (0.5 mg/kg/day with a subsequent reduction) and wound care. Significant improvement of the lesions (with desquamation and post-inflammatory macules) was observed on the two-week follow up (Figure 7). No skin involvement was present in her newborn at the two-month follow up visit.
 Figure 7: (a) Symmetric anterior thorax, upper and lower extremities involvement; (b) Post-treatment.
View Figure 7
Figure 7: (a) Symmetric anterior thorax, upper and lower extremities involvement; (b) Post-treatment.
View Figure 7
The dermatoses of pregnancy represent a heterogeneous group of skin diseases that occur only during pregnancy and/or the immediate postpartum period. Pemphigoid gestationis, formerly called herpes gestationis, is an autoimmune vesiculobullous acquired dermatosis of pregnancy and puerperium. Previous epidemiological studies had revealed PG frequencies of from 1 in 20,000 to 1 in 60,000 pregnancies. There are no differences in ethnicity, and it occurs worldwide [3].
PG shares a similar pathogenesis to that of bullous pemphigoid, with autoantibodies (IgG1 subclass) aimed against the NC16A (non-collagenous) domain of bullous pemphigoid antigen BP180 [4]. These autoantibodies stimulate an inflammatory response that causes a separation between dermis and epidermis [5]. Due to the fact that antibodies also bind to chorionic and amniotic epithelium, it has been hypothesized for the placenta to be the primary site of autoimmunity. As MHC class II molecules are aberrantly expressed on amniochorionic stromal cells and the trophoblast, it has been proposed that these molecules lead to a loss of the immune privilege of the trophoblast and amniochorion. BP180, which is expressed in the amniotic epithelium of the placenta and the umbilical cord [6], is presented to maternal MHC class II molecules in presence of paternal MHC class II. Subsequently, it is recognized as a foreign antigen, provoking the formation of IgG autoantibodies (predominantly of the IgG1 and IgG3 subclasses) [7-9]. Furthermore, PG shows a clear association with maternal HLA-DRs (HLA-DR3 and HLA-DR4) [8]. These human leukocyte antigens are present in 61-80% and 54% of PG patients, respectively. This relationship indicates a likely significant role of MHC class II in the pathogenesis of the disease [10].
Tani, et al. [11] described that the clinical features of PG in multigravidas are more severe than those in primigravidas, with an earlier onset of symptoms and demanding more extended courses of treatment. In multigravidas its onset is more common in the second trimester of gestation (38%), followed by the first trimester (38%) and finally in the third trimester (25%). It can also begin in the postpartum period. Our patient had a late onset (third trimester) but still had a severe course, likely due to previous antigen exposure on her 1st pregnancy.
Almost all patients have some degree of pruritus. Severe pruritus is frequently the initial clinical manifestation, followed by skin lesions [12]. Clinically, it is characterized by urticarial papules and plaques with posterior development of tense vesicles and bullae with an erythematous background [13]. According to Hallaji, et al. [14], the most frequently affected patient body sites are the extremities (100%) and the trunk (95.6%). Our patient had abdominal involvement, but her umbilicus was relatively spared. This is uncommon because the periumbilical area is frequently affected (65%) and it usually later spreads to the abdomen, upper and lower extremities. It can present with palmo-plantar lesions, but the mucous membranes are generally spared.
There appears to be a hormonal component affecting disease activity, with many patients experiencing improvements in late pregnancy and flares after delivery [15]. Recurrences in subsequent pregnancies are common, and are usually more severe and with an earlier onset [13]. Our patient had not presented any flares on the six-month follow up consult.
Diagnosis is made based on the presence of clinically-compatible lesions and positive histological and immunofluorescence findings. Classical histopathological findings consistent with PG include a subepidermal vesicle with perivascular lymphocytic and eosinophilic infiltrates and in some cases, basal cell necrosis with edema of dermal papillae [14]. As aforementioned, the patients' hematoxylin and eosin staining revealed a subepidermal bullae with abundant eosinofil-rich infiltrate, perivascular infiltrate and mild basal spongiosis, which was regarded as compatible with the PG diagnosis.
Direct immunofluorescence normally shows linear deposition of C3 along the basement membrane zone, along with IgG deposits in 30-40% of patients. The findings of the direct immunofluorescence of our patient (linear and fibrillar IgG deposits along the basement membrane) were also regarded as compatible with PG diagnosis. Anti-BP180 antibodies found in the patients' sera can aid the diagnosis because of their high sensitivity and specificity; however, the equipment necessary for their detection was not available in our institution [16].
Specific dermatoses of pregnancy lead to considerable morbidity for pregnant women and can pose a significant risk to the fetus, such as premature birth and birthweight below the 10th percentile for gestational age. Correct recognition and differentiation from similar diagnoses is critical, as appropriate pharmacotherapy helps mitigate symptoms and may reduce fetal risk [17].
Published guidelines regarding PG are scarce, but all of them concur with the same recommendations. First line of treatment for mild and localized PG are high-potency topical corticosteroids. If symptoms are not controlled by topical corticosteroids or if it is a severe form of the disease from the beginning, the recommendation is to start with a systemic corticosteroid (e.g. Prednisone 0.5 mg/kg/day). Once the symptoms start to recede, the dose may be tapered. For severe and persistent PG the aforementioned prednisone dose can be increased to reach 2 mg/kg/day. Other described therapies include azathioprine, high dose intravenous immunoglobulins, cyclosporine, cyclophosphamide, plasma exchange and rituximab [18].
None.
This article has no funding source.
No prior presentation of the case.