Hidradenoma or Eccrine acrospiromas are rare benign tumours that arise from the eccrine sweat gland. Eccrine acrospiromas are nonencapsulated, well-circumscribed, multilobular dermal nodules that may involve the epidermis and extend into the subcutaneous fat. A 30-year-old male patient presented with an asymptomatic progressive swelling on the scalp of 6 months duration. Cutaneous examination: A solitary, non-tender, firm to hard, mobile swelling over the scalp. Dermoscopic examination: Revealed white and red areas. Histopathological examination revealed tissue lined by epidermis with dermis showing tumor arranged in nodular configuration with proliferating cells with cells with clear cytoplasm with focal areas of squamous metaplasia. There was no evidence of necrosis or mitotic figures and diagnosis of nodular hidradenoma was made.
Nodular hidradenoma a rare appendageal tumour, is most often found in adults than children. It most commonly presents as a solitary, slow growing, well circumscribed, freely mobile, firm, non-tender, dermal lesion of varying sizes between 0.5 to 12 cm in diameter. Occasionally, the development of brown, blue or red discoloration with superficial ulceration and serous discharge may mimic malignancy. Nodular hidradenomas are most commonly seen on the scalp, neck, trunk and extremities. The diagnosis is usually confirmatory on histopathology [1,2].
A 30-year-old male patient presented with an asymptomatic progressive swelling on the scalp of 6 months duration which started as a 0.5 × 0.5 cm lesion and progressed to 3 × 3 cm size. There was no h/o discharge, pain or ulceration over the swelling. On examination: A solitary, non-tender, firm to hard, mobile swelling of size 3 × 3 cm present, over the left post-auricular region. The surface of the swelling was smooth with reddish discolouration, numerous dilated blood vessels with few areas of pus pointing (Figure 1). The surrounding area appeared normal with no regional lymphadenopathy.
 Figure 1: A solitary, non-tender, firm to hard, globular swelling mobile swelling of size 3 × 3 cm.
View Figure 1
Figure 1: A solitary, non-tender, firm to hard, globular swelling mobile swelling of size 3 × 3 cm.
View Figure 1
Excisional biopsy of the mass was done, where in it was removed in en masse with a 2 cm margin and was sent for histopathological examination which revealed tissue lined by epidermis with dermis showing tumour arranged in nodular configuration with proliferating cells with clear cytoplasm, focal areas of squamous metaplasia with no evidence of necrosis or mitotic figures (Figure 2 and Figure 3). The individual tumour cells appeared round with clear cytoplasm and diagnosis of nodular hidradenoma was made. The patient came back for follow up after 1 month but had no recurrence till date.
 Figure 2: HPE 10X-Proliferating tumor cells arranged in nodular configuration revealed on hematoxylin and eosin stain.
View Figure 2
Figure 2: HPE 10X-Proliferating tumor cells arranged in nodular configuration revealed on hematoxylin and eosin stain.
View Figure 2
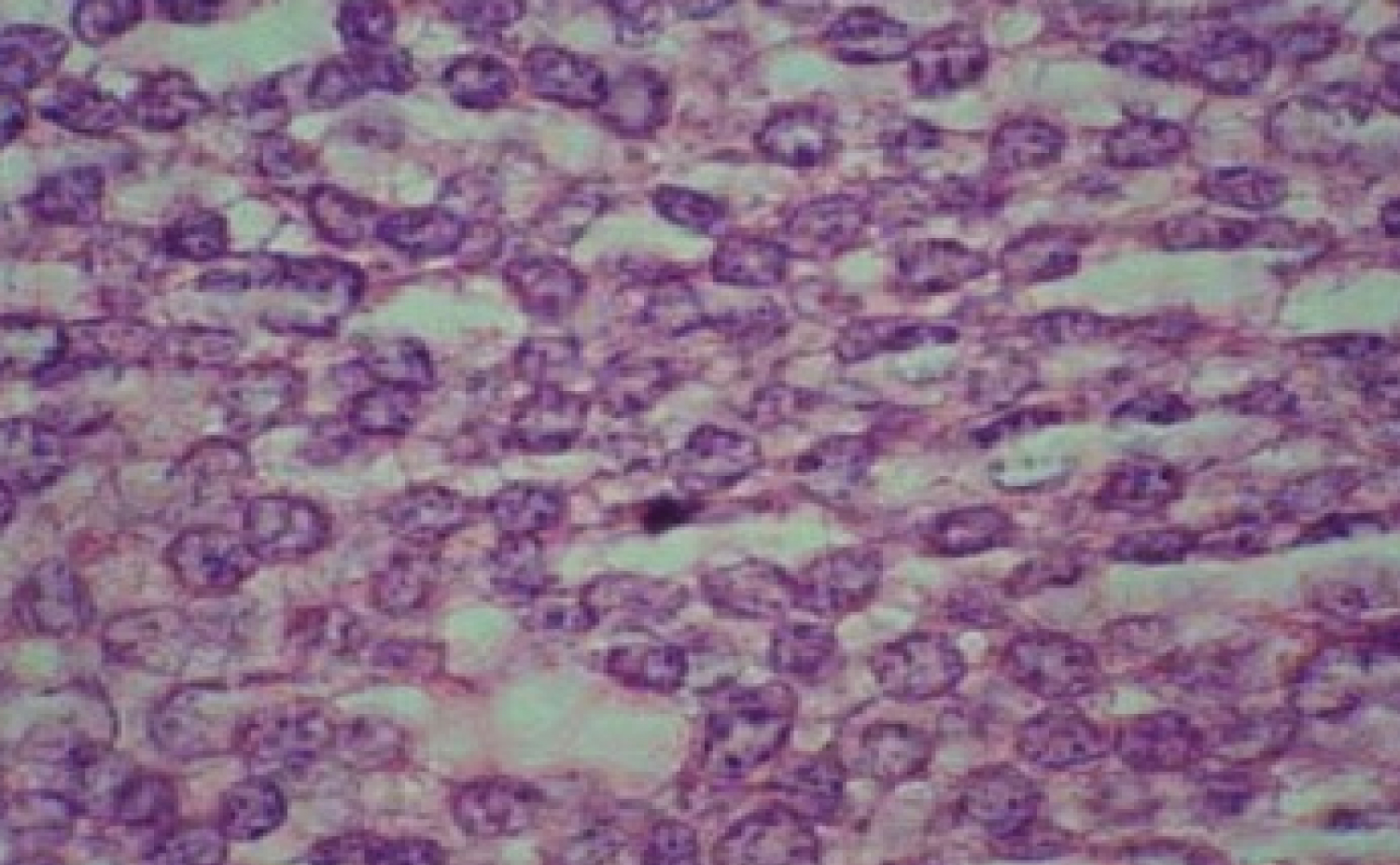 Figure 3: HPE 40 X- Round cells with clear cytoplasm on hematoxylin and eosin stain.
View Figure 3
Figure 3: HPE 40 X- Round cells with clear cytoplasm on hematoxylin and eosin stain.
View Figure 3
Dermoscopic examination revealed white pink areas, red lacuna like areas and hair pin dotted and linear irregular vessels (Figure 4).
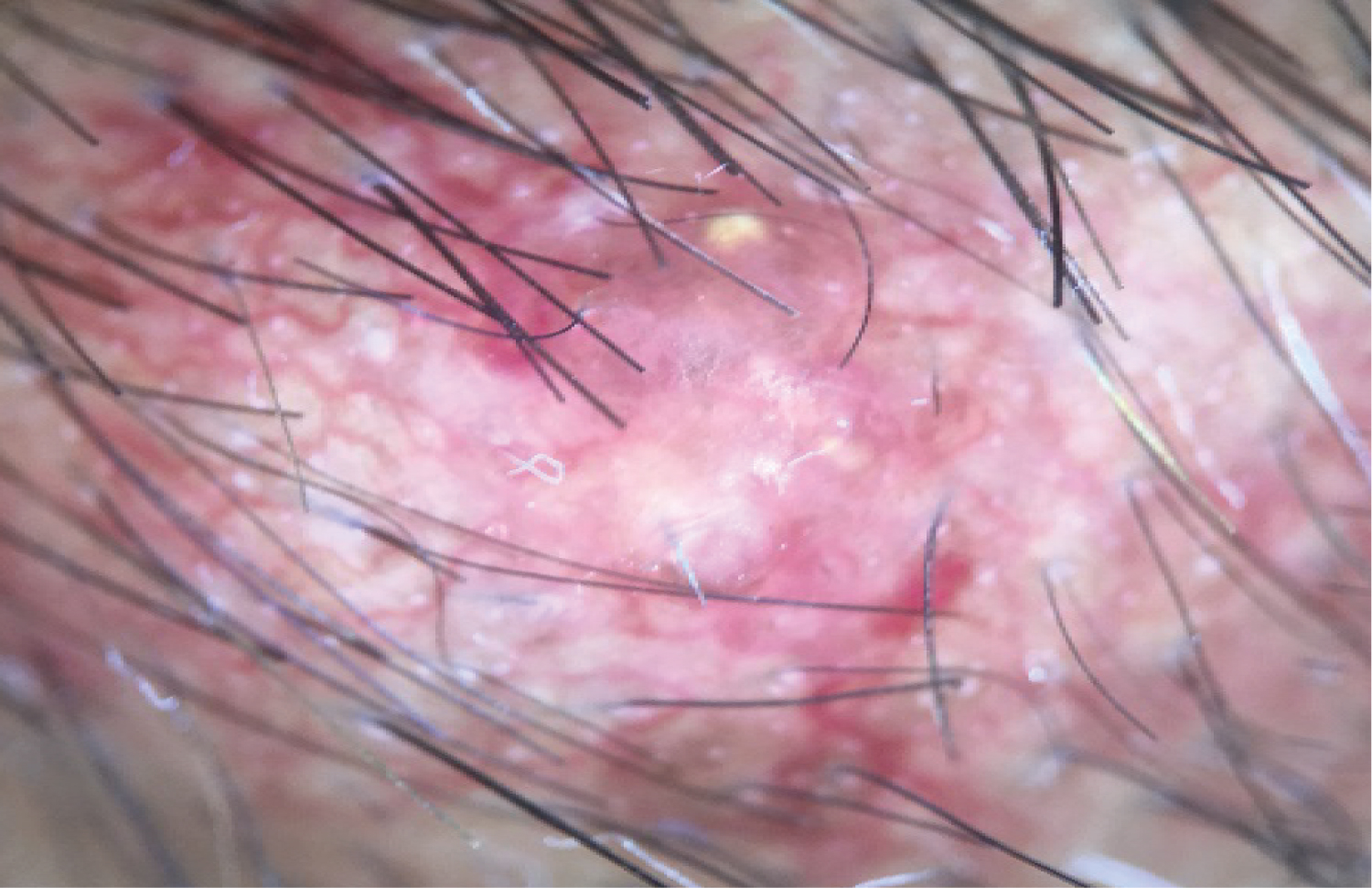 Figure 4: Dermoscopy Image with hair pin vessels and pinkish white background.
View Figure 4
Figure 4: Dermoscopy Image with hair pin vessels and pinkish white background.
View Figure 4
The patient was followed.
Nodular hidradenoma or Eccrine acrospiroma is a benign tumor originating from atrichial sweat glands and has several synonyms in literature. The term acrospiroma was first coined by Johnson and Helwig on the basis of histologic and histochemical studies. The tumor on histopathology resembled the cells and structure of ductal portion of sweat glands [1]. A series of cases studied by Hernandez-Perez and Cestoni-Parducci revealed a female predilection (1.7:1), with a mean age at presentation of 37.2 years. The most common sites of involvement as per their observation was head (30.3%) followed by the upper limb (25.8%) and then the trunk (20.2%). Histopathology depicted well circumscribed, sharply demarcated lesions from the epidermis by a clear cut Grenz zone [3].
This tumor usually presents between the fourth and the eighth decade of life, with a peak incidence in the sixth decade. There are two variants of nodular hidradenoma, the apocrine (clear cell hidradenoma) and eccrine (poroid) differentiation type. The most common among them is the Clear cell hidradenoma [4]. The aetiology of the lesions can spontaneous or traumatic. These individuals complain of pain on pressure to the tumor and pruritus or burning localized to the lesion. Most commonly these lesions present as slow growing, asymptomatic, solitary, freely mobile and firm dermal nodules. The skin surface of the swelling varies from pink-red to blue brown or purple with occasional ulceration. The local recurrences of these tumors are quite frequent but malignant transformation is very rare. Histopathologically they are characterised by well circumscribed, encapsulated nodular, solid, or solid-cystic lesions in the dermis. These may be connected to the epidermis and the dermal epithelial lobules extend into the underlying subcutaneous fat. The tumor consists of solid areas consisting of two types of epithelial cells. One of the cell types known as clear cell type has a small eccentrically placed nucleus, a well-demarcated cell border, and a clear cytoplasm. The second cell type has a round or oval nucleus, an indistinct cell boundary, and an eosinophilic solid or finely granular or vesicular cytoplasm. Also seen are transitional cells, keratinizing cells or horn pearls. Tubular lumina similar to eccrine sweat ducts and cystic cavities containing homogeneous eosinophilic material are present within the solid lobules. A structural connective tissue-stromal support surrounds the solid cell masses and cystic spaces [2]. The other cellular variants include oncocytic, epidermoid, pigmented type with melanocytes and melanin pigment in the cells and macrophages. Malignant Hidradenoma or hidradenocarcinoma histopathology reveals poor circumscription, large size, solid sheet-like growth pattern, necrosis, and vascular and lymphatic invasion, pleomorphism, and high mitotic rate. Dermoscopy reveals homogeneous area composed of the whole lesion with vascular and white structures, which is the most common presentation. The histopathological correlation of this homogeneous area is the presence of large lobulated masses of mainly polyhedral eosinophilic and clear cells with various-sized ductal structures and abundant cystic spaces located in the upper and mid dermis. The vascular patterns include arborising telangiectasias, linear-irregular vessels, dotted vessels, glomerular vessels, hairpin vessels, telangiectasias and polymorphous atypical vessels. These patterns are appreciated due to branching vascular pattern with a staghorn configuration [5]. Differential diagnosis of nodular hidradenoma includes dermatofibrosarcoma protuberans, leiomyoma, follicular cyst, and trichilemmoma [4].
Nodular hidradenoma is a rare slow growing tumor of the scalp with high malignant potential. This tumour is a simulator of malignant lesions, including basal cell carcinomas and melanomas on clinical and dermoscopic examination. This case report highlights the need to identify these tumors as a differential for painless soft tissue tumors on the scalp.