Scabies is a skin disease caused by infection with the mite Sarcoptes scabiei. The development of this disease is also influenced by low socioeconomic conditions, poor hygiene levels, lack of knowledge, and errors in diagnosis and management.
Internal and external examinations were carried out on patients related to personal hygiene behavior factors. Primary data were obtained through history taking (alloanamnesis), physical examination, and laboratory tests at Dr. Soetomo Hospital, Surabaya. A 3-year-old girl, has a habit of changing clothes and towels with his brother, and has a dirty home environment.
Based on the observation, cases of scabies with secondary infection are a problem in clean and healthy living behavior. Education to the family has an important role in the process of treating scabies with secondary infection and requires the role of parents to solve family problems and habits.
Scabies, Personal hygiene, Family medicine care, Human and medicine, Infection
Scabies is a skin disease caused by the infestation of the mite Sarcoptes scabiei. The disease that affects all types of races in the world is found in almost all countries around the world with varying prevalence rates. In some developing countries the prevalence is reported to be 6-27% of the general population and the highest incidence is in school-age children and adolescents. The development of this disease is also influenced by low socioeconomic conditions, poor hygiene levels, lack of knowledge about scabies disease, and errors in diagnosis and management.
Education for family members plays an important role in scabies disease in preventing disease and spreading the disease to the community, because this disease is easily transmitted, especially in dense settlements. Transmission or transfer between patients can take place through close direct skin contact from person to person. This can happen when living and sleeping together, for example, children who get mite infestations from their mothers, playmates, or other family members. In addition, the transfer of mites can also occur through indirect contact, namely through shared clothing or toiletries.
3-year-old girl accompanied by her mother came to the outpatient clinic of Dr. Soetomo Hospital, with complaints of small blisters which felt itchy and pus-like appearance between the fingers of hands, palms, abdomen, and chest for 6 days before the patient was treated. Lesions initially appeared small blisters filled with water and itching on the left palm, itching increased at night. The result of skin scraping is found mites. Initially by placing a drop of mineral oil directly over the burrow on the skin and then superficially scraping longitudinally and laterally across the skin with a scalpel blade. The result of gram staining from the pustule in the hand revealed gram-positive cocci and 30-40 leukocytes/field of view. Diagnosis of this patient was scabies with secondary infection. The patient was given oral cloxacillin 150 mg 4 times a day for 7 days. Wet dressings of 0.9% sodium chloride is given every 8 hours for 15 minutes on ulcer lesions on the hands. Permethrin 5% cream applied to the entire body at night and left for 8 hours, than wash it of completely with soaps. Salicylic acid 2% and sulfur praecipitatum 4% applied for 3 days to the entire body once a day in the morning after washing off permethrin (Figure 1, Figure 2 and Figure 3).
 Figure 1: Before Treatment (A,B,C,D,E,F). Multiple pustules over erythematous skin accompanied by erosions, exudates, and edema.
View Figure 1
Figure 1: Before Treatment (A,B,C,D,E,F). Multiple pustules over erythematous skin accompanied by erosions, exudates, and edema.
View Figure 1
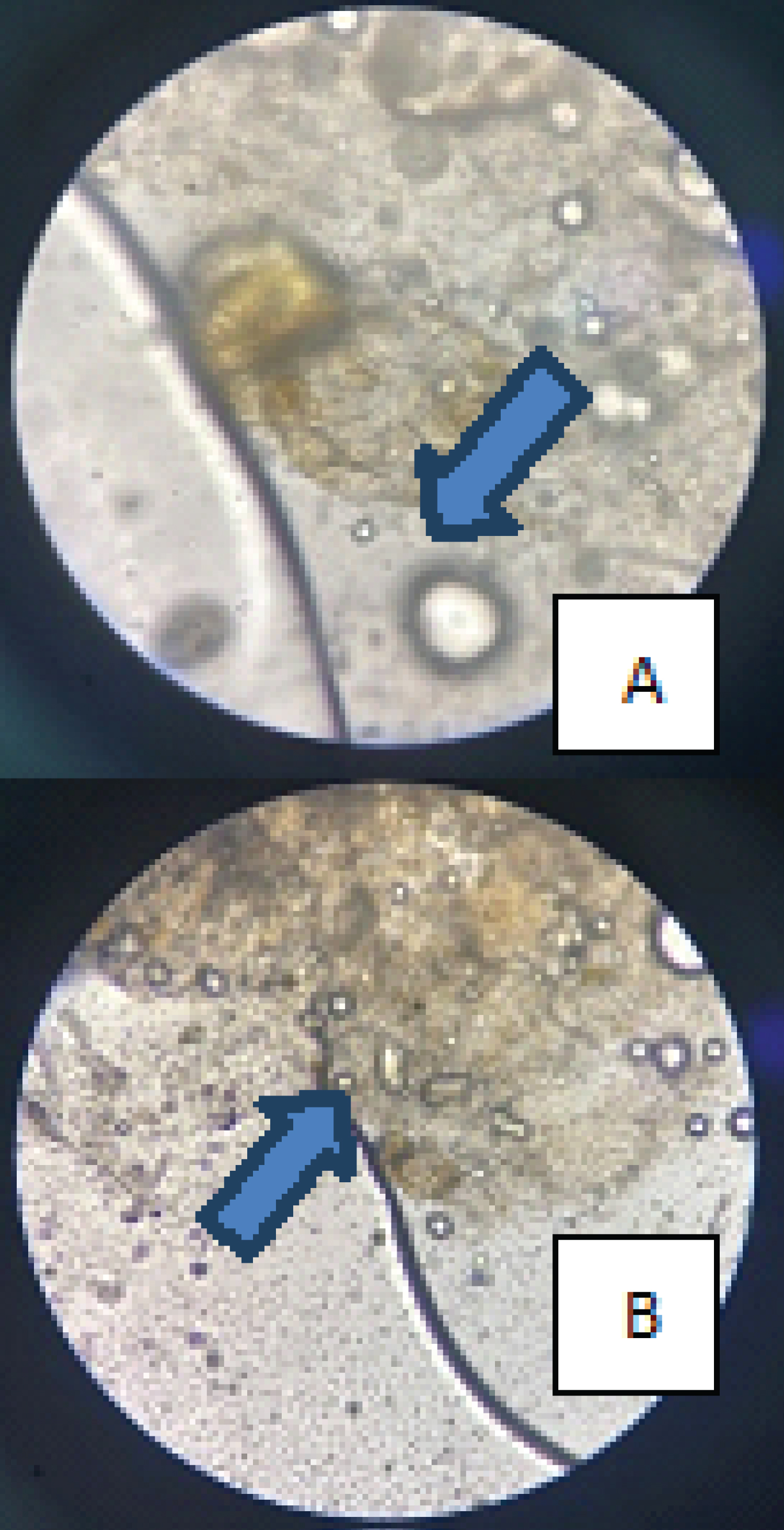 Figure 2: Microscopy showed adult mite.
View Figure 2
Figure 2: Microscopy showed adult mite.
View Figure 2
 Figure 3: After Treatment (A,B,C,D,E,F,G). Patient improved remarkably after oral antibiotic and topical treatment decrease.
View Figure 3
Figure 3: After Treatment (A,B,C,D,E,F,G). Patient improved remarkably after oral antibiotic and topical treatment decrease.
View Figure 3
Scabies is a zoonotic disease that affects the skin and is easily transmitted from human to human and from animal to human. The diagnosis is made from history, clinical manifestations and supporting examinations. The diagnosis found that there are 3 out of 4 criterias, including; itching at night, predilection and morphology that occur in a group of people, and it is found Sarcoptes scabiei mites [1-3]. The predilection is between the fingers, wrists, armpits, around the navel, inner thighs, male genitalia, and buttocks. Efflorescence of lesions due to scabies is a form of scabies infection's skin with the shape of papules and vesicles to lenticular that accompanied by excoriation [4,5]. If secondary infection occurs, lenticular pustules appear. Secondary infections in scabies are mostly caused by Group A Streptococci and Staphylococcus aureus, which are sensitive to a penicillin class. Topical agents to choose are permethrin 5% cream, salicylic acid 2%, crotamitone 10% cream, sulfur precipitum 2-10%, benzyl benzoate 10-25% emulsion and oral ivermectin 200 μg/kg/dose. Preventative efforts like improving personal and environmental hygiene are also important [6,7].
In addition to prevention efforts, treatment efforts were also carried out by providing pharmacotherapy in the form of oral cloxacillin 150 mg 4 times a day for 7 days. Wet dressings of 0.9% sodium chloride is given every 8 hours for 15 minutes on ulcerated lesions on the hands. Permethrin 5% cream applied to the entire body at night and left for 8 hours, then wash it off completely with soaps. Salicylic acid 2% and sulfur praecipitatum 4% applied for 3 days to the entire body once a day in the morning after washing off permethrin [8,9].
Based on the theory, cases of scabies with secondary infection are a problem in clean and healthy living behavior [8,9]. Education to the family has an important role in the process of treating scabies with secondary infection and requires the role of parents to solve family problems and habits [10-12].
The results of the interventions that have been carried out were evaluated, the general condition of the patient was good, the itching was reduced and the lesions had partially healed. To increase the regularity of patients using ointments, leaflets about the treatment of scabies were given. It is recommended to carry out treatment control so that it can be seen and re-evaluated. In addition, patients are also asked to invite the family of other patients who have not recovered [8,13-15].
Scabies with secondary infection has an excellent response to oral antibiotic and topical treatment. It is important to give information and education about scabies and its causes, the disease transmission, the treatment to family and people around and how to apply the medicine. Without behavior change of a clean lifestyle, the transmission of scabies will be difficult to stop and easy to recur.