Background: Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare and severe mucocutaneous reaction mainly due to drugs. Few studies have focused on this medical emergency. This study aims is to describe the epidemiologic, clinical, and treatment outcomes of the patients with SJS/TEN.
Materials and methods: A retrospective study was conducted on patients admitted to the Military Hospital of Instruction Mohamed V, Rabat Morocco, between September 2013 and June 2022. We included 34 patients. Data collected from medical records included: Age at admission, gender, diagnosis, causative drugs, comorbidities, treatment, and outcomes.
Results: A total of 34 patients including 18(52.9%) of SJS, 2(5.8%) SJS/TEN overlap, and 14(41.1%) of TEN were enrolled. A total of 55.8% were female, and the average age was 53.6 +/- 14.8 years. 88.2% of patients had concurrent medical conditions. Antibiotics were the most common causative drug followed by carbamazepine and allopurinol. All patients were admitted to the hospital, 5.8% of them had complications during hospitalization, 8.8% had long-term complication, and 14.5% were dead.
Conclusion: The most common causative drug was antibiotics followed by carbamazepine and allopurinol.
Stevens-Johnson syndrome, Toxic epidermal necrolysis, Culprit drugs, Comorbiditis, Mortality
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare, severe mucocutaneous adverse drug reaction affecting 2.6 to 13 cases per million persons per year [1]. SJS and TEN seem to have the same clinical and pathological spectrum, differing only by the percentage of body surface epidermal detachment. Whereas less than 10% of body surface area (BSA) involvement classified under SJS, SJS/TEN overlap falls under 10-30% BSA involvement, while more than 30% BSA involvement defines TEN [2].
Medications such as antibiotics, allopurinol, nonsteroidal anti-inflammatory drugs (NSAIDs), and aromatic anticonvulsants are the most frequently incriminated triggers with the highest risk of onset occurring within the initial weeks of treatment, ranging from 7 to 21 days [3]. Groups with higher risk of developing SJS/TEN include those with immunosuppression, especially those with human immunodeficiency virus (HIV) and mycoplasma, older age, slow acetylator genotypes, and individuals with specific HLA alleles [4,5].
The symptoms of SJS/TEN begin 1-4 weeks after drug exposure with the onset of prodromal symptoms - fever, cough, sore throat, and rhinorrhea - followed by a cutaneous eruption characterized by erythematous macules, atypical target lesions, blister formation, ocular, oral, or genital mucosal involvement, and progression to erosions [6]. The pathogenesis of SJS/TEN is incompletely understood, therefore the optimal treatment regimens for patients have yet to be fully elucidated.
This retrospective study aims to study the epidemiology, clinical, and treatment outcomes in patients with SJS/TEN within Moroccan population.
We retrospectively conducted a chart review of SJS/TEN patients that were treated in our Military hospital of instruction Mohamed V, Rabat, Morocco between September 2013 and June 2022. Data collected from medical records included: Age at admission, gender, diagnosis, causative drugs, comorbidities, and treatment. Initial diagnoses of SJS/TEN were made by dermatologists. Skin biopsies were performed in all patients and clinical pictures of skin lesions were available in order to validate SJS/TEN cases. We included in this study all patients with confirmed diagnoses of SJS, SJS/TEN overlap, or TEN based on Bastugi's criteria [2]. We excluded patients without available medical records for clinical course and relevant laboratory data. Culprit drugs were identified based on ALDEN score [7].
Data collection and statistical analysis were done using JAMOVI 2.2.5 current. Descriptive statistics were performed, and p < 0.05 was considered to indicate a statistically significant difference.
A total of thirty-four patients including 18 (52.9%) of SJS, 2 (5.8%) SJS/TEN overlap, and 14 (41.1%) of TEN were enrolled (Table 1). The average age was 53.6 +/- 14.8 years. Of the thirty-four cases, 55.8% were female and 44.1% were male, with a female to male ratio of 1.2. The majority of the patients (88.2%) had concurrent medical conditions. The most common conditions were hypertension (47%), diabetes mellitus (32.3%), hyperlipemia (26.4%), tuberculosis (26.4%), and gout (20.5%) (Table 2).
Table 1: Patient characteristics. View Table 1
Table 1: Patient characteristics. View Table 2
The most frequent culprit drug was antibiotics (29.4%), followed by carbamazepine (23.5%) and allopurinol (11.7%) (Figure 1). The time of latency was between 8-21 days in 70.5% of patients and all patients were admitted to the hospital, with a mean duration of hospitalization of 14 ± 9 days.
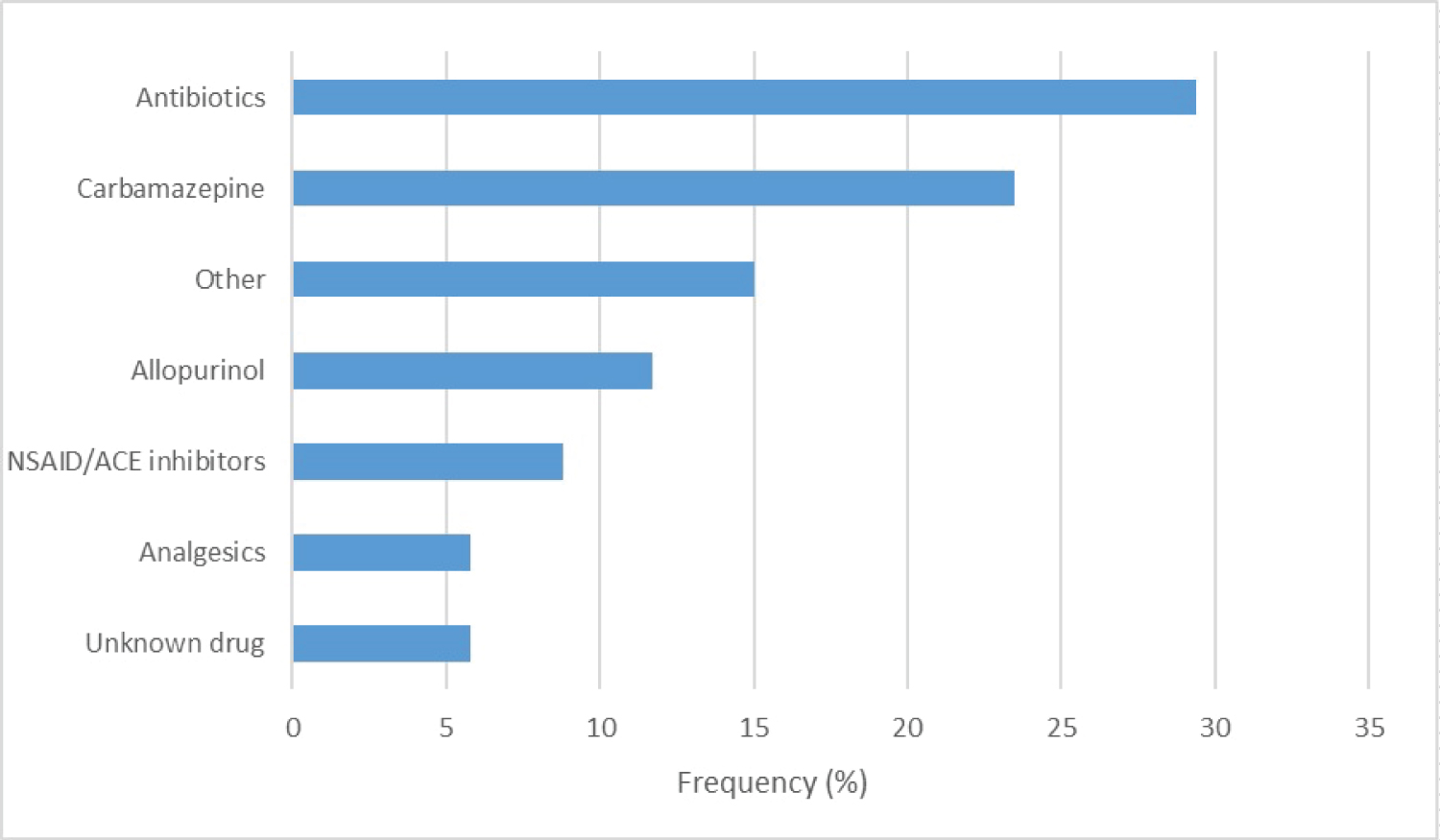 Figure 1: The frequency of culprit drugs.
View Figure 1
Figure 1: The frequency of culprit drugs.
View Figure 1
The SCORTEN score was calculated for all the patients and ranged from 0 to 5. Deaths occurred for SCORTEN > 2.
All patients had mucosal involvement, 47% had also ophthalmic involvement, and 38.2% had fever 5.8% of patients had complications during hospitalization, 8.8% had long-term complications and 14.5% were dead.
Results of univariate analysis showed that there were significant differences in the initial dosage and the total dosage of corticosteroids between the SJS group and the TEN groups (p < 0.001), and there were significant differences also in the duration of hospitalization between the SJS group and the TEN group (p < 0.001). However, there were no significant differences in time of medication consumption to onset of symptoms between the SJS group and the TEN groups (p = 0.38) (Table 3).
Table 3 : Patient's clinical findings and kind of treatment. View Table 3
TEN and SJS are a rare and severe cutaneous reaction, most often secondary to drug reactions [8,9]. It is one of the serious dermatological diseases that constitute a true medical emergency. Our study aims to describe the epidemiologic, clinical, and treatment outcomes of patients with SJS/TEN.
In our study, affected patients had a mean age of 53.6 years +/- 14.8, with a female predominance which matches with other studies [10,11]. However, some studies have reported a male preponderance [12,13].
Even if SJS and TEN are considered to take part of a similar clinical continuum, we found that cases of SJS (52.9%) were more reported than those of TEN (41.1%) which consistent with previous studies [3]. SJS/TEN could be caused by infections such as mycoplasma pneumonia and herpes simplex virus but are predominantly drug induced. We found in our study that antibiotics were the most implicated, followed by carbamazepine, in agreement with a previous moroccan study and a multicenter study in the United States [14,15]. However, In the Asian population, the most frequent culprit medication was antiepileptic drugs followed by antibiotics [16].
Several risk factors have been identified, including genetic susceptibility associated with specific HLA alleles, the coexistence of cancer, older age, and race/ethnicity [17,18]. The pathogenesis of SJS/TEN is still unknown. Several hypotheses have been suggested to explain the abnormal immune response due to the recognition and secretion of granulysin by cytotoxic CD8 T-cells, natural killer cells and the Fas-FasL interaction after exposure to certain drug metabolites which lead to keratinocyte apoptosis [19].
SJS/TEN begins within 4 weeks after a first exposure to the causative drug and a few days if reexposure to the same causative drug [20]. The severity of SJS/TEN depends on the extended of the skin detachment. It can be determined by using clinical and histological funding. Clinically, SCORTEN is a score developed to stratify the severity and predict mortality that has been validated for use on days 1 and 3 post admission [21,22]. Histologically, the extent of dermal mononuclear inflammation can be used to predict the clinical Outcome [23].
In our study, the average mortality rate was 14.5%, which was similar to mortality rate reported in the United State and in a previous Moroccan study [14,24]. The treatment consists of a multidisciplinary approach. It is based on the recognisation and retreat of the Culprit Drug, supportive care, and medical treatment. In our institution, all patients received early supportive care including airway protection, fluid replacement, nutrition and psychological support, pain management, thermoregulation, and venous thromboembolism prophylaxis. No consensus for the management of SJS/TEN is available, due probably to the low number of cases [3,8].
Several therapies were suggested for the medical management of SJS/TEN, including intravenous immunoglobulin, cyclosporine, systemic Corticosteroids, and TNF Inhibitors [25,26]. Based on the European Study of Severe Cutaneous Adverse Reactions, all our cases received systemic corticosteroids (intravenous methylprednisolone) with a good clinical course [27,28]. However, some studies suggested that corticosteroids were associated with infection, increase in mortality rate, and duration of hospitalization [29,30]. The use of intravenous immunoglobulins and cyclosporine is still controversial [10,31,32].
The strength of our study included the detailed reporting of clinical data of the patients, but it was limited by its low prevalence rate and retrospective design.
SJS/TEN are rare and constitute a medical emergency caused mainly by drugs. An early recognition of the culprit drugs and an expedited initiation of supportive care lead to lifesaving. However, more research are needed to establish an international consensus for the management of patients with SJS/TEN.
No conflicts of interest.
No funding sources received.