Introduction: Acne is a common dermatologic condition affecting more than 80% of 11 to 30-year-olds, who often suffer from acne scars. Despite the scarcity of data, acne scarring is thought to negatively impact the quality of life of patients. Therefore, the aim of the present study was to evaluate the prevalence of acne scars and their impact on the quality of life (QOL) in moroccan acne patients.
Methods: A retrospective study was conducted on patients admitted to our dermatology department. We included 147 patients with acne. Data collected from medical records included: age at the onset of acne, age at the time of initial management, Sex, acne severity, the impact of acne scarring on quality of life was performed by using the Dermatology Life Quality Index (DLQI).
Results: A total of 147 patients with acne were included. 66.7% were women and 33.3% were men. Their mean age was 24.4 ± 5.26 years. For all the patients, the age at the onset of acne, ages at the time of initial treatment were 16.4 ± 1.58, and 19.4 ± 2.11 years, respectively. For acne severity, 27.2% of the patients had mild acne, 53.1% moderate acne, 12.2% severe acne and 7.5% very severe acne. Of the 147 acne patients, 124 patients (84.4%) had acne scars. The mean total DLQI scores were 6.1 ± 3.9 for patients with scars, which is significantly higher than 4.5 ± 3.4 for patients without scars.
Conclusion: This study highlights the high prevalence of scars on acne patient and its significant impact on quality of life that increases with scars severity.
Acne severity, Acne scars, DLQI
Acne vulgaris is a common chronic inflammatory disease of the pilosebaceous follicule. It affects 80% of adolescents, young adults and is known to have a negative impact on the quality of life [1,2]. Healing of acne often produces scarring that can be peristent and can be lifelong [3].
Several studies have described the high psycho-social burden of acne, which leads to the development of depression or anxiety disorders, but few have explored the effects of acne scarring [4].
In Morocco, there have been few studies on the prevalence of scars in acne patients, and, to our knowledge, there have been no studies investigating the effect of scars on patient QOL and productivity. In this study we aimed to determine the prevalence, and the impact of facial acne scars on quality of life.
A total of 157 patients with acne vulgaris were enrolled in this study. Acne and scarring were assessed by dermatologists.
Data collected from medical records included: Age at the onset of acne, age at the time of initial management, Sex, The impact of acne scarring on QOL was performed by using the Dermatology Life Quality Index (DLQI). The DLQI has 10 items that address: symptoms, feelings, leisure, work/school, personal relationships and treatment.
Severity of acne was established by the dermatologist by using the Global Acne Severity (GEA) score. Acne scars were classified into three types: Mini-scars, atrophic scars and hypertrophic scars. Their numbers were counted.
Mini-scars were defined as atrophic scars of ≥ 0.5 and 2 mm in diameter, atrophic scars: More than 2 mm in diameter.
All data analyses and statistical processes were performed using JAMOVI version 2.3.16. Baseline respondent characteristics were determined. Descriptive statistics were performed, and p < 0.05 was considered to indicate a statistically significant difference.
Student's t-test was used to test the difference between current age, age at onset, age at initial treatment in patients with and without scars.
Chi-squared test was used to test the association between Acne severity and the presence of acne scars.
A total of 147 patients with acne were included. 66.7% (98 patients) were women and 33.3% (49 patients) were men. Their mean age was 24.4 ± 5.26 years (Table 1). The mean ages of the female and male patients were 25.6 ± 5.45 and 22 ± 3.91 years.
Table 1: Patient characteristics. View Table 1
For all the patients, the age at the onset of acne, age at the time of initial treatment were 16.4 ± 1.58, and 19.4 ± 2.11 years, respectively.
For acne severity, 27.2% of the patients had mild acne, 53.1% moderate acne, 12.2% severe acne and 7.5% very severe acne.
Of the 147 acne patients, 124 patients (84.4%) had acne scars. 24.2% of patients had only mini-scars; 57.3% had both mini-scars and atrophic scars; 8.1% of patients had atrophic scars and 10.5% had hypertrophic scars.
The mean total number of scars for all 147 patients was 26.6 ± 30.2.
To compare the background factors we divided our patients into two categories: Patients with scars (n = 124) and without scars (n = 23) (Table 2).
Table 2: Background factors and acne scars. View Table 2
The mean ages at the onset of acne for patients with scars and patients without scars were 16.5 ± 1.63 and 16.3 ± 1.29 years, respectively (P = 0.148). The mean ages at the time of initial treatment for patients with scars and patients without scars were 19.9 ± 1.89 and 16.9 ± 1.31 years, respectively (P < 0.001).
There were significant differences in the development of acne scars between the different stages of acne severity.
47.5% of patients with mild acne, 97.4% with moderate acne, and 100% of patients with severe and very severe acne experienced acne scars (Table 3).
Table 3: Acne severity and acne scars. View Table 3
The mean total DLQI scores were 6.1 ± 3.9 for patients with scars, which is significantly higher than 4.5 ± 3.4 for patients without scars (Figure 1).
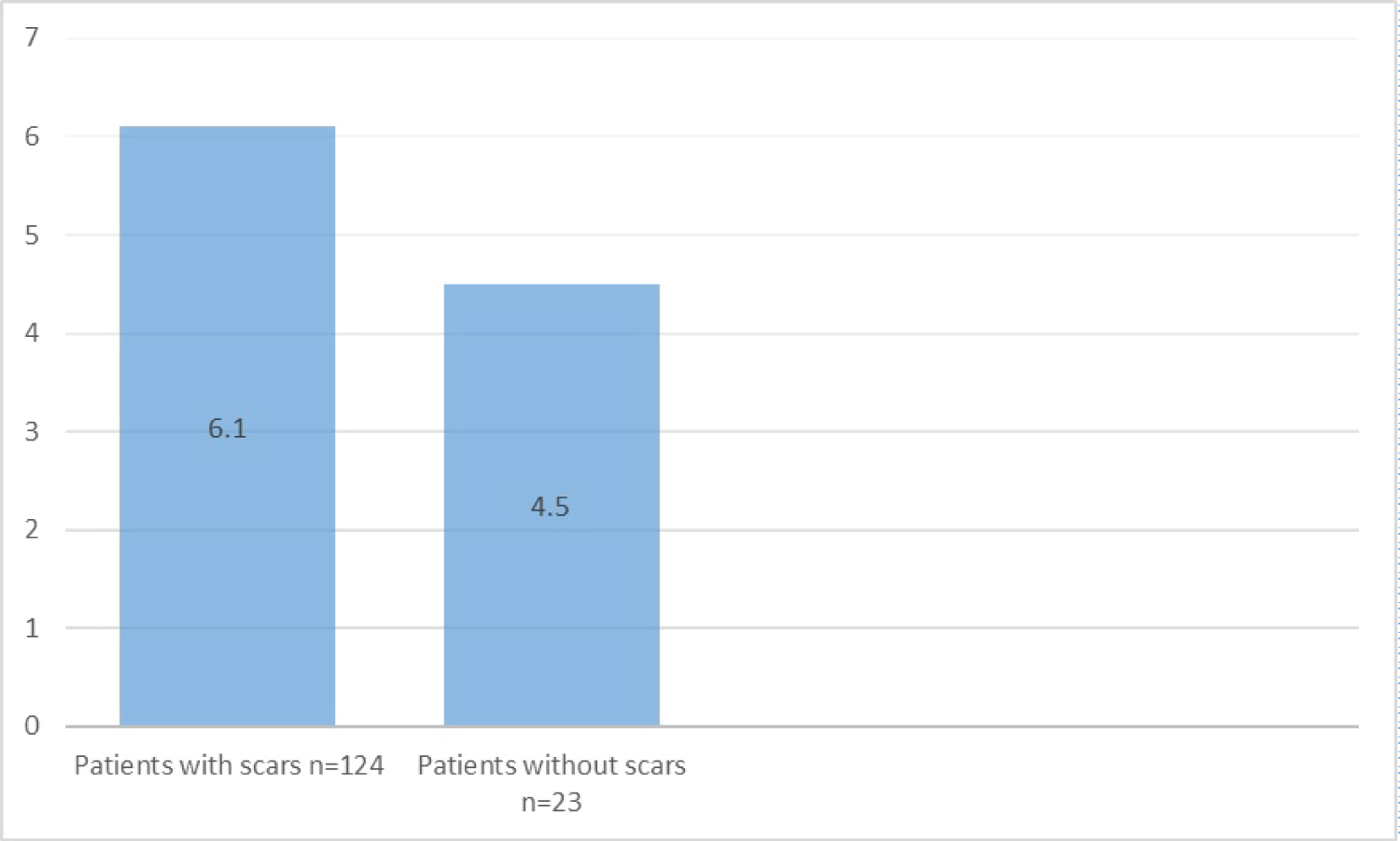 Figure 1: DLQI scores according to the presence or absence of acne scars.
View Figure 1
Figure 1: DLQI scores according to the presence or absence of acne scars.
View Figure 1
Acne is a common chronic skin condition, most often had a significant impact on quality of life. The most frequent complication of acne is scars which is often hard to treat [5].
Based on their morphology, acne scars can be classified in 3 types: ice pick, rolling, and box-car [6]. We used a simplified Japanese classification of acne scars to evaluate the prevalence of acne scars and their impact on quality of life [7].
In our study, the prevalence of acne scars was 84.4% which is similar to previous studies 90% [3,7,8]. The prevalence of types of acne scars was 24.2%, 57.3%, 8.1%, 10.5% for miniscars, miniscars and atrophic scars, atrophic scars and hypertrophic scars.
Moreover, more than a half of our patients experienced moderate acne, 12.2% had severe acne and 7.5% had very severe acne.
An interesting observation was that there was no difference in the age of onset between patients without and with scars, but the age at the time of initial treatment was significantly higher in patients with scars than in patient without scars. Which highlights the importance of early management of acne to prevent acne scars.
In line with the few reports, the risk of acne scars increased with the severity of acne. All our patients with severe and very severe acne experienced acne scars.
This point strongly indicates the importance of early adequate treatment of acne symptoms to prevent acne scars.
Another key finding revealed by our study was the impact of acne scars on patient quality of life, with a DLQI mean score of 6.1 suggesting the acne scars have a DLQI comparable to other skin diseases such as rosacea (DLQI = 6.1), Hailey Hailey disease (DLQI = 6.06) and cutaneous lupus erythematosus (DLQI = 6.50) [9].
This study highlights the significant impact of acne scars on acne patients quality of life. Therefore, effective therapies must start at the beginning of acne symptom to prevent the development of indelible acne scars.
In conclusion, this study highlights the high prevalence of scars on acne patient and its significant impact on quality of life that increases with scars severity. Therefore, quality of life impact of acne scars must be considered for therapeutic decision-making.
No conflicts of interest.
No funding sources received.