Aim: To report the visual and anatomic outcomes of surgery for complex rhegmatogenous retinal detachment in a tertiary eye hospital in Africa over a 5 year period.
Methods: Data was obtained from case files of patients who had surgery for complex rhegmatogenous retinal detachment between January 2014 and December 2018 in Eye Foundation Hospital Lagos, Nigeria. Visual and anatomic outcomes were analyzed and logistic regression done to identify factors associated with primary anatomic success, final anatomic success and good visual outcome.
Results: A total of 343 eyes of 340 patients that met the inclusion criteria were analyzed. There were 249 (73.2%) males and 91 (26.8%) females with age ranging from 7 to 87 years with a mean age of 49.43 years. Only 41 (12.9%) eyes presented within a week of onset of symptoms, 263 (76.9%) eyes had vitrectomy with silicon oil exchange, 13 (3.8%) eyes had vitrectomy with gas, 15(4.4%) eyes had scleral buckling surgery alone while 51 (14.9%) eyes had combined scleral buckle with vitrectomy. Primary anatomical success was achieved in 281 (88.7%) eyes, Final anatomical success was achieved in 288 (92.9%) eyes and good visual outcomes achieved in 208 (61.4%) eyes. Using a simple logistic regression, eyes with normal or near normal visual acuity at presentation were more likely to have good visual outcomes (p = 0.00034). When compared with macula off rhegmatogenous retinal detachment, eyes with macula on at presentation also had a higher likelihood of final anatomic success (p = 0.001).
Conclusion: Despite complex pathology in eyes with rhegmatogenous retinal detachment, good anatomic and visual outcomes can be achieved after surgery. Primary anatomic success was achieved in 88.7% of eyes and 92.9% of eyes achieved final anatomic success. Good visual outcomes were achieved in 61.4% of eyes. Eyes with normal or near normal visual acuity at presentation were more likely to have good visual outcomes (p = 0.00034). When compared with macula off RRD, eyes with macula on at presentation had a higher likelihood of final anatomic success (p = 0.001).
Rhegmatogenous retinal detachment (RRD) develops when there is a retinal ‘break' or full-thickness defect in the neurosensory retina (NSR) that allows the ingress of fluid from the vitreous cavity into the subretinal space, resulting in separation of the NSR from the underlying retinal pigment epithelium (RPE) [1]. It is the most common form of retinal detachment (RD) occurring in approximately 1 in 10,000 of the population per annum [2]. There are several risk factors for RRDs; most RRDs are associated with retinal tear formation at the time of PVD [3]. There is an increased risk of RRD in myopic patients, with an up to 10-fold increase in myopia over three diopters (D) [4], pseudophakic retinal detachments (PPRD) occurs in 0.36-2.9% of cases within 10 years of phacoemulsification [5]. Other risk factors include trauma, peripheral retina degenerations, systemic diseases like Marfans Syndrome and Sticklers Syndrome, occupational lifting of heavy weights has also been suggested as a possible risk factor [6].
Pars plana vitrectomy (PPV), scleral buckling (SB), and pneumatic retinopexy (PnR) are used for the treatment of RRD, with primary success rates of up to 90% [7]. PPV is currently the most common procedure used for the treatment of RRD [8]. The reported primary anatomical success of SB ranges between 53% and 83% [9-11], while that for vitrectomy ranges from 72% to 93% as reported by two large comparative randomised studies by Heimann, et al. [9] and Hillier, et al. [12]. A previous study in our hospital in 2012 reported a primary anatomic success of 80.5% [13].
Outcomes of retina detachment surgery are often reported as both anatomic and visual. Anatomic success refers to successful reattachment of the neurosensory retina with the underlying retina pigment epithelium, whereas the visual outcomes are measured in terms of the visual acuity after surgery [13,14]. There is however a paucity of information about outcomes of retina detachment surgery in Africa, our study reports these outcomes over a 5-year period.
This is a retrospective interventional study. Data was obtained from records of patients who had surgery for complex rhegmatogenous retinal detachment between January 2014 and December 2018 at Eye Foundation Hospital Lagos Nigeria. Patients who had either tractional or exudative retina detachments were excluded, as well as patients who had other retinal complications from non rhegmatogenous causes eg retina vein occlusions, diabetic retinopathy, age related macula degeneration and polypoidal choroidal vasculopathy. The study protocol was conducted according to the principles described in the Declaration of Helsinki. Ethics committee approval was obtained.
Two retinal surgeons (O.O and O.O) performed all surgeries with The Alcon Constellation using 23G or 25G instruments. Perflourocarbon fluids were used at the surgeons' discretion for both giant tears and other holes or tears. Data was analyzed for demographic characteristics, preoperative, intraoperative and postoperative features. Surgical variables were analyzed using the Chi squared test and Student's t test. Categorical variables were expressed as a frequency (percentage) and simple logistic regression was done to identify impact of identified factors on both the visual and anatomic outcomes. Analysis was done with IBM SPSS statistics version 22 (IBM Corp. Armonk, NY, USA) and p < 0.05 was considered statistically significant.
Primary anatomic success: Retinal reattachment maintained at least 3 months after primary surgery without reoperation.
Final anatomic success: Retinal reattachment maintained at least 3 months after the last intervention. Good visual outcome: Snellen visual acuity better or equal to 6/60 at 3 months post-interrvention. Retina tears extending more than 45 degrees of the retina associated with posterior vitreous detachments were described as giant tears.
Visual acuity (VA) was defined by WHO [15] visual acuity standards into blindness/profound visual impairment for distant visual acuity less than 3/60, severe visual impairment for acuity better than 3/60 but less than 6/60, moderate visual impairment for acuity of 6/60 and better but less than 6/18, acuity of 6/18 and better was considered near normal/normal.
Rhegmatogenous retinal detachment (RRD) was clinically classified as simple or complex detachment. Simple RRD, was retinal detachment (RD) localized to a single, small retinal tear or hole at the retinal periphery accompanied by good visibility of the fundus, while in complex RRD, the detachment wass partial, subtotal or total with a giant retinal tear, retinal dialysis, multiple retinal breaks, posterior breaks and also, it may be associated with vitreous hemorrhage, ocular trauma and proliferative vitreoretinopathy [16,17].
A total of 343 patients that met the inclusion criteria were analyzed. There were 249 (73.2%) males and 91 (26.8%) females. The patients ages ranged from 7 to 87 years with a mean of 49.43 ± 14.9 years.
Most of the RRDs were idiopathic RRDs 123 (46.6%) eyes. Post-traumatic 56 (21.2) eyes, myopic 51 (19.3%) eyes and post-surgical 28 (10.6%) eyes, other causes accounted for 6 (2.3%) eyes. Majority of eyes 123 (38.7%) presented between 1 week to 6 weeks (moderate) of symptoms of visual loss, 41(12.9%) eyes presented within a week (early), 61 (19.2%) eyes between 6-12 weeks (chronic), while 93( 29.2%) eyes presented after 12 weeks (very chronic) of onset of symptoms, the duration of symptoms was not specified in 25 (7.3%) eyes. Post-operative follow up ranged from 3 to 21 months with an average of 16.49 months (Table 1).
Table 1: Summary percentages of visual and anatomic outcomes based on preoperative characteristics of macula status, aetiology, gender, duration of detachment and presenting visual acuity. View Table 1
Most of the retinal detachments were due to tears or holes 195 (70.5%) eyes. Giant tears were identified in 81 (29.5%) eyes of patients. Majority of the detachments were superior 115 (40.4%) eyes, inferior in 84 (29.5%) eyes, temporal in 46 (16.0%) eyes and unspecified in 40 (14.0%) eyes. Majority of patients presented with blindness (70.2%). The macula was off in majority (82%) of patients. The lens status was not specified in 4 (1.2%) eyes, while 297 (86.6%) eyes were phakic, 31 eyes (9.0%) pseudophakic and 11 (3.2%) eyes aphakic. Proliferative vitreoretinopathy was not evaluated because of significant inconsistency in the records and the use of different grading systems by different evaluating surgeons.
Pars plana vitrectomy (PPV) alone was done in 276 (80.7%) eyes, out of which 263 (76.9%) eyes had PPV with silicon oil exchange, 13 (3.8%) eyes had PPV with sulphur hexafloride (SF6) gas, while 15 (4.4%) eyes had scleral buckle (SB) and 51 (14.9%) eyes had combined SB with PPV.
Overall 281 (88.6%) eyes had primary anatomical success, while 288 (92.9%) eyes had final anatomical success and 208 (61.4%) eyes had good visual outcomes.
Using a simple logistic regression, eyes with normal or near normal visual acuity at presentation were more likely to achieve good visual outcomes (p =< 0.0001). It was found from the study that patients with VA < 3/60 at presentation were more likely to have poor visual outcomes (OR = 0.232 95% CI = 0.086-0.629, p = 0.004). Gender, status of macula and aetiology did not significantly influence the likelihood of good visual outcome (0.119, 0.095, 0.500 respectively). Patients with duration of detachment between 1 week to 6 weeks were less likely to have good visual outcome compared to early presentation within a week (B = -0.096, OR = 0.909 CI = 0.327-2.526, p = 0.854). In the same way patients with chronic RRDs (greater than 6 weeks) (B = 0.046, OR = 1.047, CI = 0.338-3.239, p = 0.937) and very chronic duration RRDs (greater than 12 weeks) of detachment (B = -0.874, OR = 0.417, CI = 0.146-1.190, p = 0.102) respectively had a strong negative correlation for good visual outcomes. Status of the macula did not show any significant probability of good visual outcome (B = 0.031, OR = 1.031, CI 0.414-2.567, p = 0.948) Table 1.
Visual acuity, gender, duration, status of macula, etiology did not statistically significantly influence the likelihood of good visual outcome using simple regression analysis. (0.369, 0.137, 0.870, 0.241, 0.969 respectively) Table 1.
Using a simple logistic regression eyes with macula on at presentation had a higher likelihood of achieving final anatomic success when compared with macula off RRD (p = 0.001). Also, eyes with preoperative VA > 6/18 had statistically significant likelihood of final anatomic success (p = 0.031). Duration, etiology and gender did not statistically significantly determine the likelihood of final anatomic success (0.303, 0.683, and 0.399 respectively) Table 1.
About 74.9% (197/263) of patients who had PPV + silicon oil were blind at presentation, 5.7% (15/263) had severe visual impairment, 13.7% (36/263) had moderate visual impairment while 5.7% (15/263) had near normal/normal vision. Furthermore, 53.8% (7/13) of those who had PPV + gas were blind at presentation while 15.4% (2/13) had severe visual impairment and 30.8% (4/13) had near normal/normal vision. Majority of patients who had SB had near normal/normal vision 86.7% (13/15) and 13.3% (2/15) of them presented with blindness. Lastly, 66.7% (34/51) of those who had PPV + SB presented with blindness, 5.9% (3/51) had severe visual impairment, 15.7% (8/51) had moderate visual impairment and 11.8% (6/51) had normal/near normal vision. There is a highly statistically significant association between technique of surgery and presenting visual acuity (p < 0.001) Table 2.
Table 2: Technique of surgery and presenting visual acuity. View Table 2
The highest percentage of 93.3% (14/15) of eyes that had good visual outcome was recorded among SB patients, followed by PPV + gas with 76.9% (10/13), PPV + silicon oil with 59.9% (157/262) and PPV+SB with 55.1% (27/49). This association was statistically significant (p = 0.032) Table 3.
Table 3: Table showing primary anatomical success rate, final anatomic success rate and rate of good visual outcome with technique of surgery. View Table 3
Our study showed that the least primary anatomical success was recorded among 66.7% (10/15) of eyes that had SB, the highest primary anatomical success of 90.1% (219/243) was recorded among eyes who had PPV + silicon oil. About 83.3% (10/12) of eyes that had PPV+ gas, and 89.4% (42/47) of eyes that had PPV + SB also had primary anatomic success. This association was statistically significant (p = 0.044) Table 3.
About 92.8% final anatomic success was recorded amongst patient who had PPV + silicon oil, 91.7% was recorded among those who had PPV + gas, 100% final anatomical success was recorded among patients with SB and 91.3% final anatomic success was recorded among PPV + SB. There was no statistically significant difference between the technique of surgery and attainment of final anatomical success (p = 0.716). Eyes that did not achieve primary anatomic success had PPV + silicon oil as a second procedure, regardless of which surgical technique was used initially Table 3.
The overall primary anatomical success rate among all aphakic eyes was 80%, among pseudophakic eyes 85.7% and among phakic eyes 89.2%. Final anatomic success was achieved in 94.1% of phakic eyes, 85.7% of pseudophakic eyes and 77.8% of aphakic eyes. While 63.5% of phakic eyes, 60% of aphakic eyes and 41.9% of all pseudophakic eyes had good visual outcomes.
Out of 297 phakic eyes, 279 had adequate data for visual outcome and primary anatomic success analysis. The primary anatomic success percentage was similar with all eyes that had PPV, 90.6% (192/212) for PPV + silicon oil, 90% (9/10) for PPV + gas and 90.5% (38/42) for PPV + SB. The primary anatomical success rate was lowest 66.7% (10/15) in phakics who had SB only. This finding was statistically significant (p = 0.038). In addition, 61.8% of phakics who had PPV + oil had good visual outcome while among patients who had PPV + gas, SB and PPV + SB; 90.9%, 93.3% and 55.6% had good visual outcome respectively. Rate for good visual outcome was lowest in phakics who had PPV + SB (p = 0.013).
Among 31 pseudophakic eyes included in the study, only 28 had adequate data for analysis of anatomic and visual outcomes. Primary anatomical success was achieved in 84.0% (21/25) of eyes that had PPV + silicon oil, and 100% (3/3) of eyes that had PPV + SB. No pseudophakic eye had repair using SB or PPV + gas. Our study showed that 42.9% (12/28) of patients who had PPV + oil had good visual outcome while 33.3% (1/3) of those who had PPV+SB had good visual outcome. This association was not statistically significant (p = 0.624).
Out of 11 aphakic eyes included in our study, 10 eyes had adequate records for analysis of primary anatomic success and visual outcome. The rate of primary anatomical success with various techniques includes 100% for PPV + silicon oil, 50% for PPV + gas and PPV + SB respectively. No aphakic patient had SB only (p = 0.153). Good visual outcomes were seen in 70.0% (7/10) of aphakics who had PPV+oil and 50% (5/10) of aphakic eyes that had PPV + SB. All aphakic eyes 100% (2/2) who had PPV + gas failed to achieve good visual outcome (p = 0.132).
Anatomic retina reattachment is the main aim of surgery for RRD, presently many surgeons report reattachment rates above 90% irrespective of techniques used [12-14,18]. In our study, 88.6% of patients had primary anatomical success, while 92.9% of patients had final anatomical success. Improvements in successful outcomes with retinal detachment surgery are due in part, to recent advances in instrumentation, techniques and technology. The advent of use of perflorocarbon liquids, small guage vitrectomy, more efficient cutters, better microscopes with improved optics and viewing systems all contribute to this improvements, the vitreous gel can be more safely removed as much as possible without causing damage to the retina. These improvements also allow the eye to have less inflammation postoperatively thus reducing complications from severe inflammation [14,19]. Improving surgeon skill and understanding of the pathology of a retinal detachment, careful planning and appropriate patient selection, are contributors to good patient outcomes [19]. Preoperative visual acuity has been reported to be the most important factor predicting primary and final anatomical success after retinal detachment surgery, [20] our study results equally show the same likelihood, eyes with VA > 6/18 preoperatively had statistically significant likelihood of final anatomic success (p = 0.031). There was a male preponderance and the mean age of patients with RRD was 47 years this is similar to results from our previous studies [13,14,18], however, duration, etiology and gender did not statistically significantly determine the likelihood of final anatomic success (0.303, 0.683, and 0.399 respectively).
Eyes with macula on (18.0%) at presentation had a statistically significant likelihood of final anatomic success (p = 0.001) when compared to eyes with macula off (82.0%) at presentation, similar findings were reported by Eva Smretschnig, et al. [19]. The above suggest that patients who had less complicated detachments (macula on with VA > 6/18) at presentation had a higher likelihood of achieving final anatomic success Figure 1, shows fundus pictures and ultrasound Bscan of macula on RRD in the right eye of a 54-year-old high myope. This patient presented early and was able to maintain his best corrected 6/9 preoperative vision after removal of silicon oil, when compared to patient in Figure 2 who presented with a macula off bullous RRD, 6/60 vision, and was able to achieve a best corrected vision of 6/18 after removal of silicon oil.
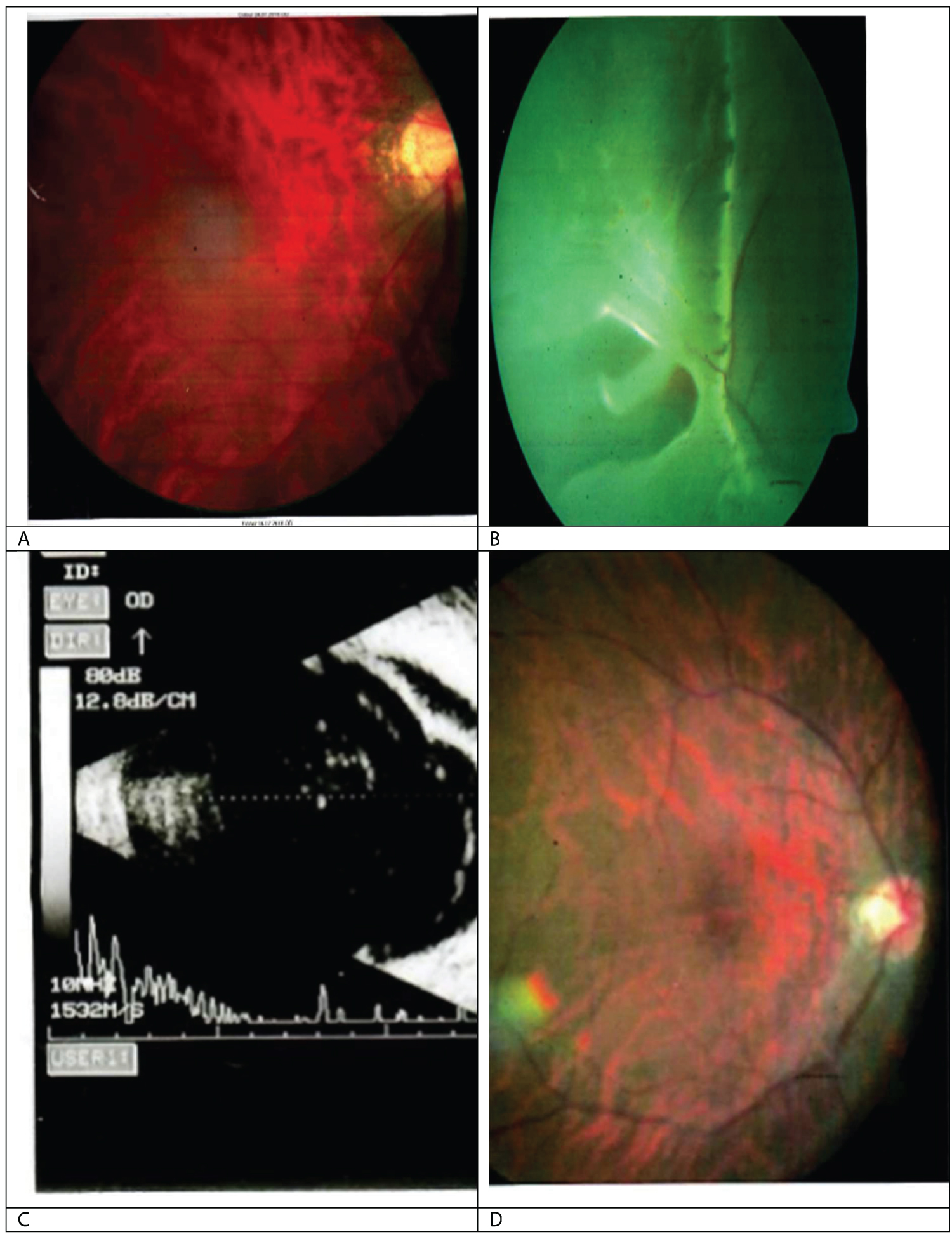 Figure 1: Features of macula on rhegmatogenous retinal detachment in the right eye of a 54-year-old high myope. (A) Shows macula on with presenting best-corrected visual acuities of 6/9; (B) Shows one of two peripheral retina tears at 9 o'clock with temporal retina detachment (second tear at 11 o'clock was not visible on fundus photograph); (C) Ultrasound B scan features of retinal detachment with associated posterior vitreous detachment; (D) Posterior pole of reattached retina after removal of silicon oil with vision maintained at 6/9 best corrected.
View Figure 1
Figure 1: Features of macula on rhegmatogenous retinal detachment in the right eye of a 54-year-old high myope. (A) Shows macula on with presenting best-corrected visual acuities of 6/9; (B) Shows one of two peripheral retina tears at 9 o'clock with temporal retina detachment (second tear at 11 o'clock was not visible on fundus photograph); (C) Ultrasound B scan features of retinal detachment with associated posterior vitreous detachment; (D) Posterior pole of reattached retina after removal of silicon oil with vision maintained at 6/9 best corrected.
View Figure 1
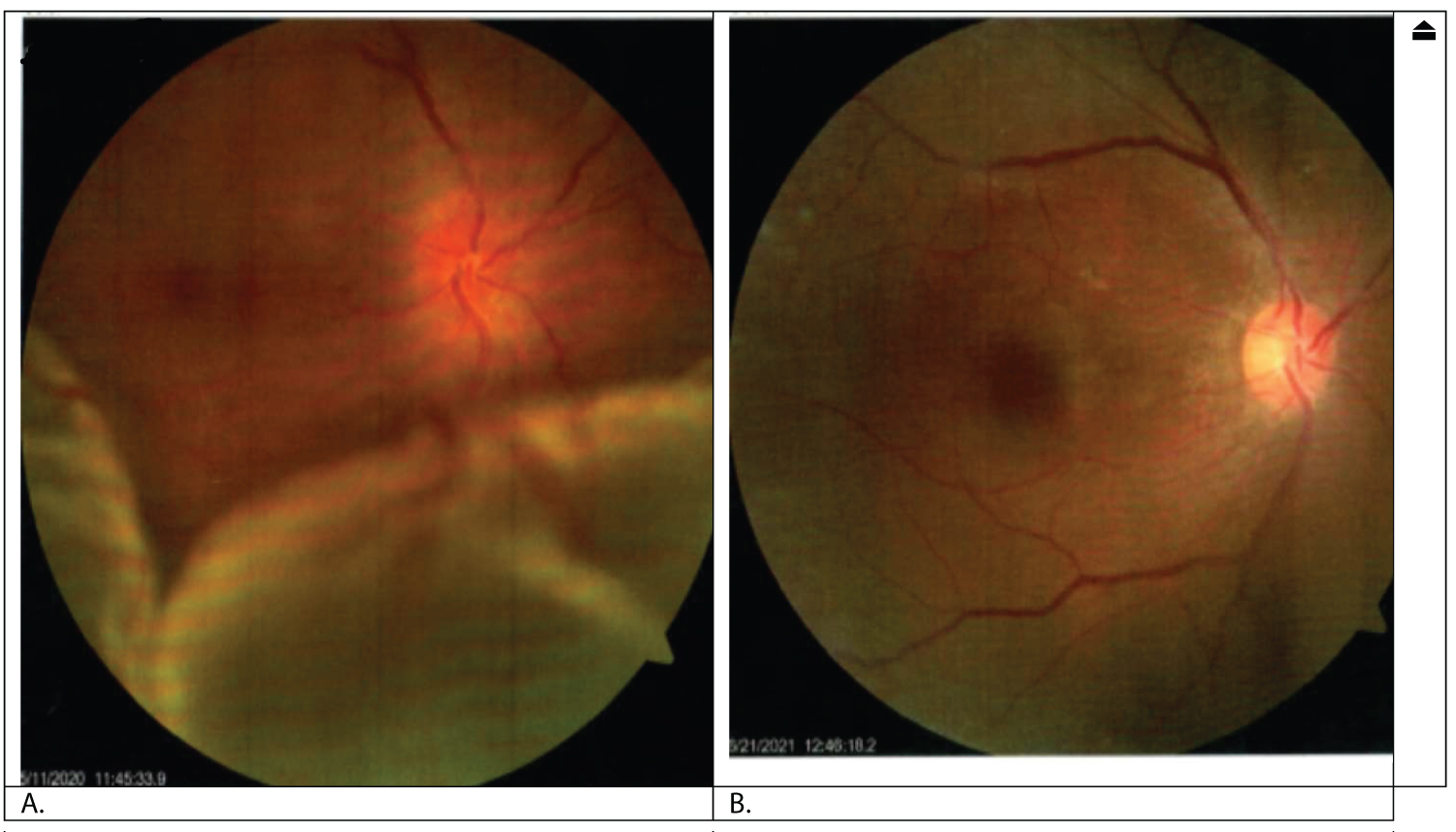 Figure 2: Features of a macula off bullous inferior rhegmatogenous retinal detachment in the right eye of a 46-year-old man. (A) Shows the bullous macula on appearance at presentation; (B) Reattached retina maintained at 6 months after removal of silicon oil.
View Figure 2
Figure 2: Features of a macula off bullous inferior rhegmatogenous retinal detachment in the right eye of a 46-year-old man. (A) Shows the bullous macula on appearance at presentation; (B) Reattached retina maintained at 6 months after removal of silicon oil.
View Figure 2
Eyes with normal or near normal visual acuity at presentation were more likely to have good visual outcomes (p =< 0.0001). It was found from our study that patients with VA < 3/60 at presentation were more likely to have poor visual outcomes (OR = 0.232 95% CI = 0.086-0.629, p = 0.004) Gender, duration, status of macula and etiology did not statistically significantly influence the likelihood of good visual outcome (0.119, 0.095, 0.500 respectively). Patients with early presentation within a week of detachment had an increased likelihood to achieve good visual outcomes when compared to patients who presented late, this was however not statistically significant (B =-0.096, OR = 0.909 CI = 0.327-2.526, p = 0.854) same as the status of the macula (on or off) which did not show any statistical significant probability of good visual outcome (B = 0.031, OR = 1.031, CI 0.414-2.567, p = 0.948). However, a recent study has reported that the height of macular detachment not just its detachment alone is a statistical predictor of postoperative visual acuity. Supposedly, the shallower the macular detachment is, the greater the likelihood of a good visual outcome [21].
The optimal technique for repair of a RRD has been a subject of debate for sometime. Scleral buckle is considered a more traditional method and requires less sophisticated equipment than par plana vitrectomy (PPV). The choice of procedure used for RRDs in our cohort of patients was basically at the surgeon's discretion. Decisions were made by surgeons based on the nature of the detachment, presence of complications like proliferative vitreoretinopathy and surgeon preference. Although there was no uniform criteria for deciding which surgery to perform for RRDs, patients who had scleral buckles generally had better presenting visual acuities than those who had other techniques of RRD repair, only 13.3% of eyes who had SB surgery were blind at presentation compared to 74.9% of patients who had PPV with silicon oil . This finding was statistically significant (p =< 0.001), as a result a higher percentage of patients in the SB group achieved good visual outcomes (93.3%) when compared with PPV + gas (76.9%), PPV + silicon oil (59.9%) and PPV + SB (55.1%) (p = 0.032). However, when relating the technique used to achievement of primary anatomic attachment our study showed that the least primary anatomical success was recorded among 66.7% (10/15) of eyes that had SB, the highest primary anatomical success of 90.1% (219/243) was recorded among eyes who had PPV + silicon oil. About 83.3% (10/12) of eyes that had PPV + gas, and 89.4% (42/47) of eyes that had PPV + SB also had primary anatomic success. This association was statistically significant (p = 0.044) Table 3. In essence we found that although a higher percentage of eyes who had SB achieved good visual outcomes, SB was less effective in achieving primary anatomic success when compared to PPV. A higher percentage of eyes who had PPV with gas also achieved good visual outcomes when compared to PPV with silicon oil. Recent reports point to reduced vision after silicon oil use or removal when compared to gas, the vitreous potassium sink theory and a possible similar optic nerve head sink have been suggested as possible causes. The interphase between the retina/optic nerve and the silicon oil meniscus seems inadequate for proper function of the potassium pump [22]. Hence early removal of silicon oil when not contraindicated should be contemplated rather than late.
The strong preference for PPV (80.7%) in our series of eyes, with silicon oil the preferred tamponade (76.9%) , compared to SF6 gas (3.8%) is due to the presence of complex pathologies at presentation, 29.5% of eyes had giant tears, 70.2% were blind at presentation and 82% of eyes had their maculas affected. Howbeit, PPV is now considered a preferable technique for primary RDS in many departments. In the United Kingdom Wickham, et al. [23] reported PPV is now the method of choice in 70–80% of all cases of retinal detachment and Johanson, et al. [24] reporting a rise of use of PPV from 1% to almost 50% within a decade when compared to SB procedures. Fewer surgeons are combining SBs with PPV, however we still performed this combined procedure in 14.9% of eyes in our study. Scleral buckles were added to PPV when there was an inferior retina hole at 6 o'clock or when as a result of PVR it was important to alter the equatorial diameter of the globe thus reducing the effect of tangential traction.
Although giant retina tears are considered uncommon [25], a high percentage (29.5%) of eyes in our series had giant retina tears , this was different from our previous findings with 8.7% of eyes [13] and the experience in another study from Africa [26]. Our instituition is a tertiary instutuition, we receive referrals of complex retina pathology from other centers, this likely contributes to the high percentage of RRDs with giant tears referred to our hospital. A good number of centres in our country perform SB but just a few do PPV, since RRDs with giant tears are more amendable to PPV [14] we get a lot more referrals of this indication.
We observed some trends in choice of technique for surgery and outcomes in our series of eyes. Patients who had SB procedures had good presenting visual acuities and thus better visual outcomes. All eyes that had PPV had a significantly higher percentage of anatomic success when compared to SB. No pseudophakic or aphakic eye was managed with scleral buckle alone. All pseudophakic eyes that had SB+PPV achieved primary anatomic success. Among phakic eyes primary anatomic success rate was similar with all eyes that had PPV, but low in eyes that had scleral buckle alone, this finding was statistically significant.
We noticed an improvement in surgical outcomes in our previous report. In our previous report in 2012 [13]. Primary anatomic success was achieved in 80.5% of eyes, while final anatomic success was achieved in 90.2% of eyes and good visual outcome was achieved in 38.8% of eyes. Compared to 88.6% of eyes achieving primary anatomical success, 92.9% of eyes with final anatomical success and 61.4% eyes with good visual outcomes. When intraocular gas was used SF6 is now the preferred gas compared to C3F8 in our earlier series with a strong preference for PPV and silicon oil still obvious.
This study is limited by its retrospective design, a purely retrospective study like ours limits the amount of information that can be evaluated. Decisions like which technique of retina reattachment surgery to use and whether or not to use perfluorocarbon liquids were completely at the surgeons discretion.
This study shows that despite complex pathology seen in eyes with RRD in Africa, good anatomic and visual outcomes can still be achieved after surgery. Eyes with macula on at presentation (p = 0.001) and preoperative visual acuity > 6/18 (p = 0.031) had a higher likelihood of final anatomic success, while eyes with near normal or normal visual acuity at presentation were more likely to achieve good visual outcomes (p =< 0.0001). Eyes that had scleral buckles had better presenting visual acuities and thus were more likely to achieve good visual outcomes (p = 0.0032), while patients who had pars plana vitrectomy were more likely to achieve primary anatomic success (p = 0.044).