Background: Cataract is the leading cause of blindness in developing countries including Nepal. Cataract surgical coverage is relatively low in rural areas where prevalence of blindness is high.
Objective: To find the proportion of patients who are blind or have low vision prior to undergoing free cataract surgery at a tertiary eye care hospital.
Material and methods: This a descriptive cross-sectional camp-based study conducted at tertiary level eye hospital of Nepal over a period of six months from Oct 2021 to April 2022.
Results: A total of 6916 patients received free eye service from camps, out of which 3136 were male (45.34%) and 3780 were female (54.66%). 3059 patients were selected for cataract and other ocular surgeries of which 1776 patients (58.05%) came to receive various ocular surgeries. 853 were male (48%) and 923 were female (52%); Of which 1706 patients received free cataract surgery, 69 patients received pterygium (PERFECT) surgery and only one patient came to receive entropion correction surgery. females have lower coverage to access health facility and comprises 52% of all cataract cases in the study populations. The mean age of operated patients in our study was 60.84 ± 11.6 years.
Conclusion: Cataract remains to be the major cause of blindness in Nepal and free eye camps are still a requisite in a vast part of the country for backward classes, under-privileged, women and senior citizens. Surgical eye camps can aid in reducing the preventable blindness and closing the gender gap could significantly decrease the prevalence of cataract blindness, gender sensitive intervention programmes are needed to improve cataract surgical coverage among females.
Blindness, Cataract, Eye camp, Nepal blindness survey
Nepal is a culturally, ethnically, and geographically diverse country perched on the southern slopes of the Himalayan mountains. Because of its landlocked nature and rugged geography, the country is underdeveloped. The burden of problems typically for underserved populations, continues to be an issue for the Nepalese population.
In most developing countries, prevalence of blindness has not decreased significantly mainly because of the increase in population and longevity of people. Aging is the most important factor in visual impairment and blindness. However, Nepal, inspite of the increase in population and longevity of people, difficult geographical terrain and transportation and long-standing political unrest, has been successful in reducing the prevalence of blindness from 0.84% of 1981 to 0.35% at present [1]. This is apparently a great achievement which is the result of tireless concerted efforts of national NGO’s involved in implementing eye care program, government of Nepal and the international NGO’s and other stakeholders supporting eye care service of Nepal.
The Nepal blindness survey (NBS) conducted in 1981 [2] was the major milestone in the history of eye care service of Nepal and after three decade of eye care service delivery and one decade of vision 2020 in Nepal, Nepal Netra Jyoti Sangh took the initiation for reassessing the situation of blindness adopting the Rapid Assessment of Avoidable Blindness (RAAB) survey in the country. The report of these surveys shows the overall prevalence of blindness has reduced to 0.35% compared to that of 0.84% in 1981 [1].
Cataract is the main cause of bilateral blindness (62.2%), posterior segment diseases (16.5%), glaucoma (5.9%), corneal scar and other than trachoma (5.2%) and uncorrected aphakia (3.4%). Blindness in Nepal is treatable in 66%, preventable in 16% and permanent in 19% of the affected persons [3]. Barriers to cataract surgery- In Nepal, ‘cannot afford’ is major barrier to surgery in bilaterally blind due to cataract is 23% followed by ‘No company’ (18%), ‘unaware of treatment’ (15%), ‘old age, no need’ (12%), ‘No services’ and ‘contra-indications’ (5%); ‘wait for maturity’, ‘how to get surgery’ and ‘fear of operation’ (5%), ‘No time; (3%) [4].
Cataract is responsible for 65%of blindness in Nepal [1], so to reduce the bulk of cataract blindness, R.M. Kedia Eye Hospital (RMKEH) from its beginning, started an eye screening program at the community level. The objective of the program is to serve community who is unable to come themselves at hospital to take their treatment. It provides its services mainly to those who are poor and marginalized and not able to come directly to hospital. This study is done to find the proportion of patients who are blind or have low vision prior to undergoing free cataract surgery at a tertiary eye care hospital, selected from free eye camps at different rural places of parsa and bara district within a period of six months.
A descriptive cross-sectional study was conducted, and a preoperative clinical and social data of patients were selected for cataract surgery through eye camps conducted by our hospital for a period of 6 months from Oct 2021 till April 2022. Ethical clearance from the hospital Institutional Review Committee was taken to carry out the study. Posters, banners, and announcement were made through local FM radios to the areas where camps were to be conducted for the people around that area to participate at the camp and have their eyes checked.
As per Nepal Blindness survey vision categories were defined as:
1) Normal or near normal vision: 6/6-6/18 in both eyes;
2) Visual impairment: < 6/18 to 6/60 in worse eye and 6/60 in better eye;
3) Unilateral blindness: < 6/60 in worse eye and 6/60 in better eye;
4) Moderate bilateral blindness: < 6/60 in worse eye and < 6/60 to 3/60 in better eye;
5) Severe bilateral blindness: < 3/60 in both eyes.
The community eye camps organized by our hospital to screen patients in their villages consisted of six staffs: 1 Ophthalmic Assistant for screening, 1 optometrist for refraction, eye health worker for counseling, primary eye health worker for vision examination, optical helper for optical dispensing each and a driver. Patients selected for cataract surgery were divided into groups and counselled for visiting our hospital to receive surgery free of cost.
Cataract patients identified at camps at the time of their visit to hospital, meticulous examination of each patient including distant vision, clinical examination by slit lamp, tonometry, ocular biometry, IOL power calculation, fundus examination, condition of other eye, and presence of any associated pathology was done prior to surgery. A well-informed verbal and written consent were taken from all the patients undergoing ocular surgeries.
Patients underwent cataract surgery under aseptic precautions under peribulbar block at our hospital during the period of 6 months. The method of cataract surgery was manual sutureless small incision cataract surgery (SICS), whereby the whole of the nucleus is removed through a self-sealing sclero-corneal tunnel and a single-piece PMMA IOL manufactured in Nepal was inserted into the capsular bag. This technique requires no sophisticated equipment, is machine-independent, sutureless, provides excellent visual outcome and quick rehabilitation. After surgery patients were discharged after post of evaluation on the first post-op day with topical steroid+ antibiotics drops and black goggles all free of cost provided by the hospital. Consent was taken from the hospital ethical committee to carry out the study.
In camp, total of 6916 patients attended to receive free service, out of which 3136 were male (45.34%) and 3780 were female (54.66%). A total of 3059 patients were selected for cataract and other ocular surgeries and the remaining 3857 patients’ visual acuity was improved with prescribed glasses (Table 1).
Table 1: Presenting visual acuity of camp patients. View Table 1
Out of the 3059 selected patients for ocular surgeries, only 1776 patients (58.05%) came to receive various ocular surgeries, 853 were male (48%) and 923 were female (52%); Of which 1706 patients received free cataract surgery, 69 patients received pterygium (PERFECT) surgery and only one patient came to receive entropion correction surgery and the remaining 3780 patients of the total mainly came to receive refractive error glasses and topical medications (Figure 1).
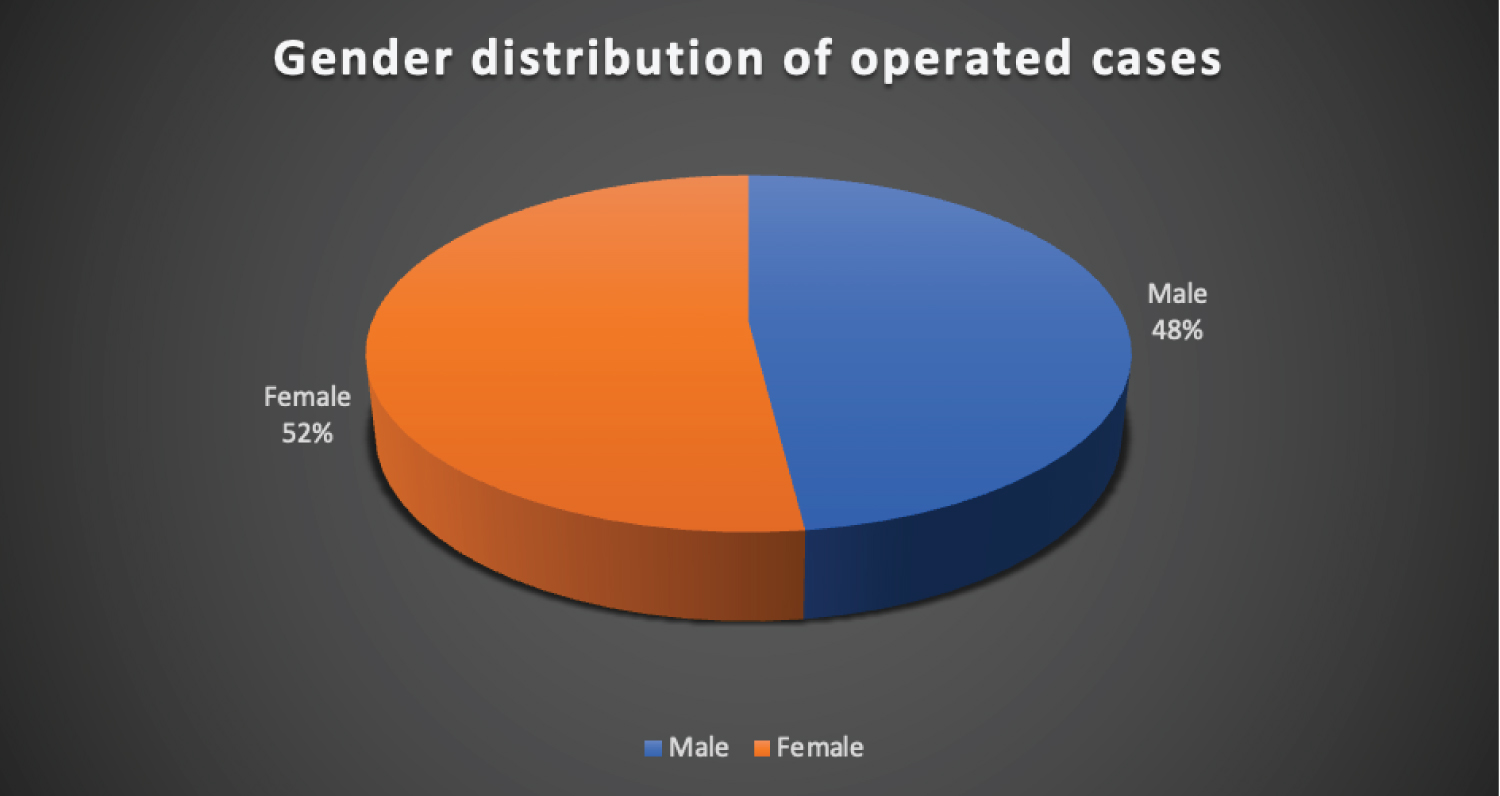 Figure 1: Pie chart showing the gender distribution of operated cases.
View Figure 1
Figure 1: Pie chart showing the gender distribution of operated cases.
View Figure 1
Vision in two eyes varies and multiple probabilities may occur from 6/6 in both eyes to no vision in both or either eye. Table 2 provides the details of number of patients undergoing surgery.
Table 2: Provides the details of number of patients undergoing surgery. View Table 2
The chi-square test was performed using excel sheet and the result was highly statistically significant with p-value of 0.0005. Out of 1776 operated cases, 809 (45.55%) patients were operated in their right eye and 967 (54.45%) patients were operated in their left eye, showing difference in distribution of surgical cases by laterality (Figure 2).
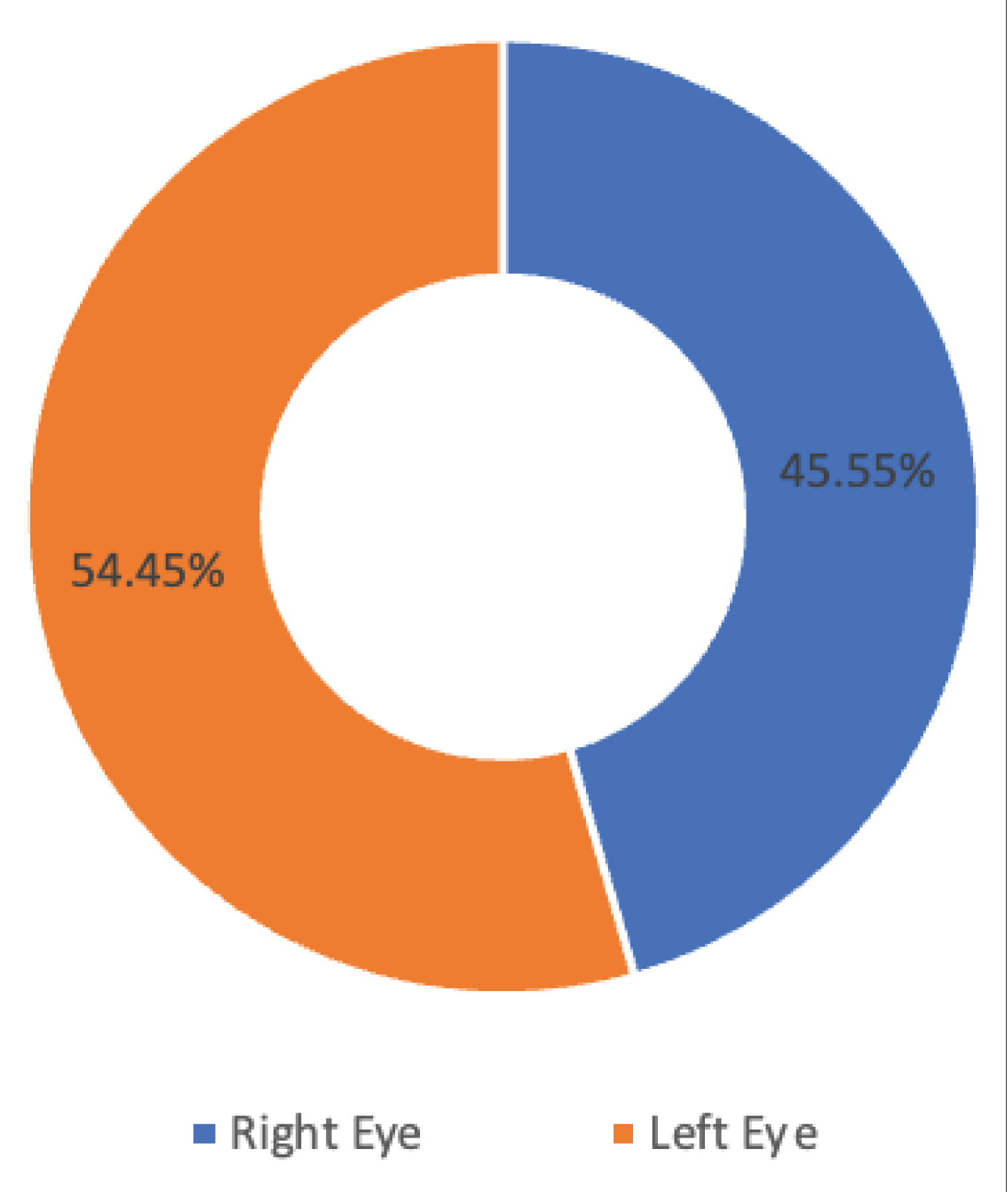 Figure 2: Distribution of operated cases by Laterality.
View Figure 2
Figure 2: Distribution of operated cases by Laterality.
View Figure 2
Most of the operated patients were in their 5 th to 7 th decade with age range from 21 to 86 years of age (Figure 3).
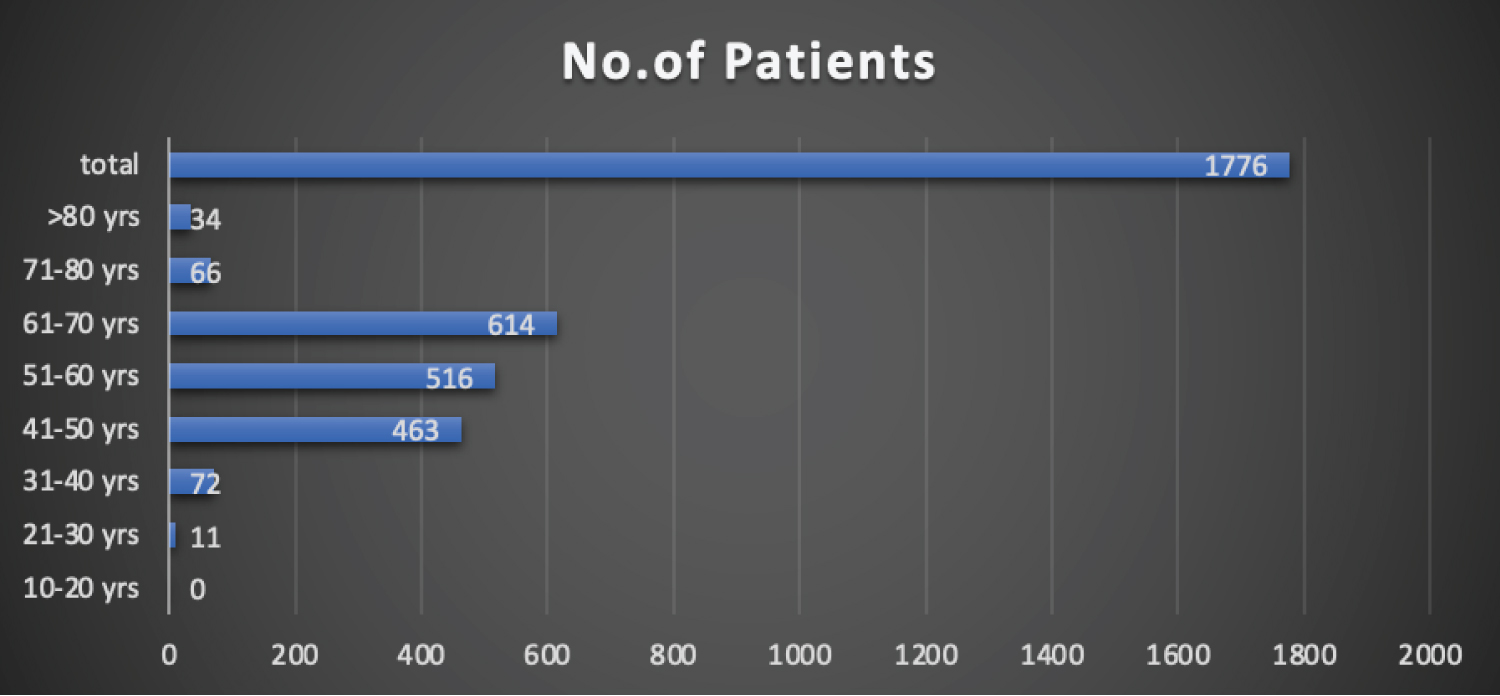 Figure 3: Bar diagram showing age range of operated cases.
View Figure 3
Figure 3: Bar diagram showing age range of operated cases.
View Figure 3
Blindness continues to remain a major public health problem in our country reinforcing call for sustained effort at its control. A Mid Term Review (MTR) [1] committee established in 2010 reviewed the implementation of Vision 2020 in Nepal and showed that the prevalence of blindness has declined from 0.84% in 1981 to 0.39% in 2010 [1].
Cataract is a condition of senility, which is a major cause of reversible blindness accounting for about 62% blindness, prevalence of blindness in population of 50 years and above is bound to be high, estimated to be 8.5% in comparison to 1.1.5 in general population in 2001 National survey of blindness [5].
Although gender inequity remains a significant problem in Nepal; since it is still believed in our part of the far rural society that only men are the head of the family, and the head of the family should be prioritized and benefited with all the facilities available in their society as it being a male dominant society. However, it is not necessarily true for all programs. Thapa, et al., reported that the cataract surgical coverage was high in females in Bhaktapur study which is like our study where 52% of the subjects were female to receive cataract surgery in our study [6].
It was estimated that cataract blindness could have been reduced to a rate of 12.5% in 2000 and 10.8% in 2008 if males and females had the same cataract surgical coverage rates [7], in contrast, our results showed that female patients (52%) has visited our hospital to receive surgical service more in comparison to male patients (48%). The life expectancy of Nepalese people is 71.45 years [8], and the mean age of operated patients in our study was 60.84 ± 11.6 years, which is like the study by Gilbert, et al. [9] showing the prevalence of cataract blindness was above the age of 50 years.
Although a total of 3059 patients were selected for cataract and other ocular surgeries, only 1776 patients came to receive the service, which shows that there is still a belief in the far rural community that they should get operated only when they are not able to see at all. Since Poverty and transportation remains one of the contributory factors for lower access to prevail eye care services to reduce preventable blindness, our hospital has been conducting free eye surgical camps for very remote areas of local districts. Even though females have lower coverage rate due to the cultural burden, illiteracy, and low socio-economic status, they comprise of 52% of all cataract cases in our study populations. If they get the surgical modality at the same rate as males, the prevalence of cataract blindness would be reduced significantly [10].
Manual SICS is proved to be effective and faster surgical technique and far less expensive to perform than phacoemulsification. PMMA lenses have been manufactured in Nepal and are about One-tenth the cost of foldable IOL’s imported from abroad [11].
Despite the number of free eye camps organized in our part of the world, still, a large backlog of cataract cases can still be seen in the community due to male-dominant society. Free eye camps are still a requisite in a vast part of the country for backward classes, underprivileged women, and senior citizens. Since our community still has a dominant community with female gender lacking equal facilities in all aspects, it remains a significant barrier to access to cataract surgery in our community, and we assume that once the female population achieves an equal cataract service coverage compared to males, the prevalence of cataract blindness can be reduced.
None.
None.