Purpose: This study evaluates the outcome of anatomical success in macular hole (MH) surgery.
Materials and methods: This was a prospective study on patients operated for idiopathic MH at Preah Ang Duong Hospital. Patients underwent pars plana vitrectomy with inverted internal limiting membrane (ILM) flap and postoperative prone positioning. The primary outcome measure was anatomical closure of MH. The secondary outcome measure was postoperative best-corrected visual acuity (BCVA) and ocular complications.
Results: Anatomical closure of MH was achieved in all 22 eyes operated (100%). Mean best-corrected visual acuity (BCVA) improved from 1.35 ± 0.32 at baseline to 1.14 ± 0.41 logMAR at last follow-up (p = 0.01). The mean improvement in BCVA was 2.3 lines. 12 patients or 54.5% presented with the final visual acuity improvement of two or more line of Snellen Chart.
Conclusion: The inverted ILM flap technique is a safe technique improving both anatomical and functional outcomes of vitrectomy for macular holes with a diameter greater than 400 μm.
Macular hole, Internal limiting membrane, Inverted ILM flap
The gold standard treatment of macular holes is vitrectomy with an anatomical success rate of 93-98% [1]. However, only 40-80% anatomical success is shown in large macular holes [2]. As a result, most surgeons are discouraged from performing vitrectomy on these patients given the poor prognosis [3].
Inverted internal limiting membrane (ILM) flap technique was first introduced as a management for large macular holes by Michalewska, et al. [4]. In comparison to conventional ILM peeling (ILMP), inverted (ILM) flaps provide better anatomical and visual outcomes. Recent studies have suggested that the inverted ILM flap technique (IFT) showed better results for the treatment of large macular holes [5]. The visual improvement and anatomical closure rates were up to 75% and 95% respectively for full-thickness macular hole with a minimum diameter (MD) > 400 μm treated with an inverted ILM flap technique in a meta-analysis [6]. However, many previous studies on the subject were retrospective in nature; none of which explored the clinical parameters, including diameter of macular hole and axial length, as prognostic indicators of macular hole closure and visual outcome.
Therefore, this study aims to prospectively evaluate the anatomical success in macular hole surgery using the inverted internal limiting membrane flap technique in the Cambodian population.
This was a prospective study of patients operated for idiopathic full-thickness macular hole from July 2020 to November 2021 at Preah Ang Duong Hospital, Phnom Penh, Cambodia, after obtaining approval from the National Ethics Committee for Health Research (Registration N° 142 NECHR dated 20 th May 2020). Prior to surgery, each patient signed a written informed consent for participation.
Inclusion criteria included patients, aged 18 years and above, with a baseline best corrected visual acuity (BCVA) of 6/60 or better and diagnosed as having an idiopathic full-thickness macular hole of stage II and above. Exclusion criteria were high myopia (> 6D), age-related macular degeneration, diabetic retinopathy, glaucoma, previous intraocular surgeries except for uncomplicated phacoemulsification, history of trauma, patients unable to maintain postoperative prone position and any systemic contraindication for surgery.
Patient data including age and gender, baseline best-corrected visual acuity, and intraocular pressure (IOP) were recorded. The Snellen visual acuity was converted into a logarithm of the minimum angle of resolution (logMAR) for statistical analysis. MH diameter was defined as the minimum distance between the open MH and a line parallel to the retinal pigment epithelium and was measured with optical coherence tomography (OCT) (CIRRUS photo 800; Carl Zeiss Meditec AG, Germany) using 512 × 128 macular cube scans passing through the fovea, before and after the surgery [7].
All surgeries were conducted by a single surgeon under local anesthesia with a 23-gauge needle. First, core vitrectomy and induction of posterior vitreous detachment were performed. Followed by 0.05% Brilliant Blue G dye staining of the ILM, an approximately 2-disc-diameter flap was peeled off circularly around the macular hole with its margin remaining attached to the macular hole’s rim and the ILM flap was tucked into the hole. Fluid-air exchange was done followed by sclerotomy sites sutured with a 7-0 Vicryl suture. 48-hour postoperative prone positioning was strictly required for all patients.
The postoperative regimen included topical antibiotics, steroids, and oral analgesics were prescribed and gradually tapered.
Patients were appointed for follow-up visits on day 1, 2 weeks, 1 month, and 3 months. At each appointment, the examiners recorded BCVA, IOP, and SD-OCT. The main outcome measures were anatomical and visual outcomes at the end of 3 months. In this study, anatomical closure is defined as the flattening of the macular hole with resolution of subretinal fluid and complete coverage of the fovea by neurosensory retina [8].
Statistical analysis was performed using SPSS advanced statistical software version 20.0 (SPSS Inc., Chicago, IL) for Mac. For statistical analysis, BCVA was converted to logMAR units. Counting fingers, hand motion, and light perception were converted as a logMAR value of 1.8, 2.3, and 2.8 respectively [9-11]. Qualitative data was recorded as a percentage and quantitative data was mean ± standard deviation. The Wilcoxon signed-rank test was used to analyze time-course differences in VA. P value £0.05 was considered statistically significant.
Twenty-two patients with macular hole (9 male, 13 female) were recruited for the study. The pre-operative baseline characteristics were shown in Table 1. The patients’ age was ranged from 52 to 76-years-old (mean ± SD = 65 years ± 7.16). Among 22 patients, 16 patients or 72.7% had MH in right eyes while 6 patients or 27.3% had in left eyes. Twelve patients (54.44%) were phakic and ten patients (45.45%) were pseudophakic. Nine patients (40.91%) underwent pars plana vitrectomy combining with phacoemulsification procedure whereas thirteen patients (59.09%) underwent pars plana vitrectomy only. All included patients had stage 4 macular holes with the mean base diameter of 593.45 ± 91.90 μm SD, which ranged from 420 μm to 844 μm. The mean pre-operative best corrected visual acuity was logMAR 1.35 ± 0.32.
Table 1: The Baseline characteristics. View Table 1
Anatomical closure was achieved in all patients (100%). At least two-line improvement postoperatively was seen in 54.5% (n = 12/22) eyes (Table 2) and no visual acuity improvement was seen in 40.91% (n = 9/22) eyes. One patient, on the other hand, had his final visual acuity worsen from logMAR 1.3 to logMAR 1.8 (Sellen equivalent 6/120 to CF1m). Mean BCVA was logMAR 1.23 ± 0.43 at post-operative 1-month and logMAR 1.14 ± 0.41 at postoperative 6-month respectively. The mean improvement in BCVA was 2.3 lines.
Table 2: Anatomical and functional outcomes. View Table 2
Changes in visual acuity (VA) are shown in Figure 1. One-month postoperative VA was not statistically different comparing to the preoperative VA ( p = 0.089). Three-month postoperative VA, however, was significantly better than preoperative VA ( p < 0.05).
 Figure 1: Time course of post-operative improvement in visual acuity (VA).
View Figure 1
Figure 1: Time course of post-operative improvement in visual acuity (VA).
View Figure 1
In the follow-up periods, there was no record of patient developing retinal tear or retinal detachment. Two phakic eyes 9.1% developed cataract and eventually required cataract surgery. Postoperatively, at first month and third month, the measurement of intraocular pressure was 14.37 ± mmHg and 13.59 ± 3.55 mmHg and no anti-glaucoma medications was required during that period. No significant postoperative complicated were noted.
Tomography analysis : Case 1: 55-year-old female presented with dimness of vision in right eye for past 6 months with BCVA of 6/120. Stage 4 idiopathic macular hole with base diameter of 844 μm was detected on SDOCT (Figure 2A and Figure 2B). Case 2: A 76-year-old male presented with dimness of vision in left eye for past 4 months with BCVA of 6/60. Stage 4 idiopathic macular hole with base diameter of 1.15 μm was detected on SDOCT (Figure 2C and Figure 2D).
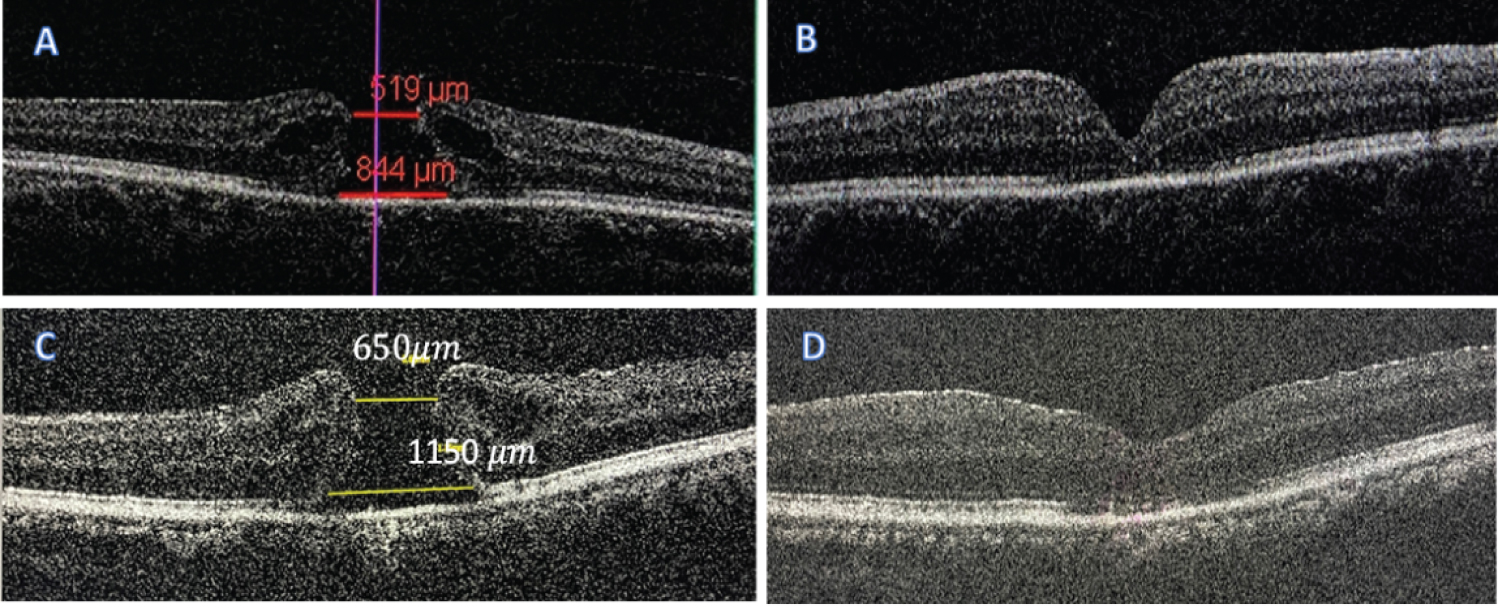 Figure 2: Spectral-domain optical coherence (SD-OCT) of representative cases: (A) Preoperative SD-OCT image at baseline 3 months; (B) Postoperative SD-OCT image at 3 months follow up; (C) Preoperative SD-OCT image at baseline 3 months; (D) Postoperative SD-OCT image at 3 months follow up. Discontinuity in outer retinal structures was detected postoperatively, as shown in the images.
View Figure 2
Figure 2: Spectral-domain optical coherence (SD-OCT) of representative cases: (A) Preoperative SD-OCT image at baseline 3 months; (B) Postoperative SD-OCT image at 3 months follow up; (C) Preoperative SD-OCT image at baseline 3 months; (D) Postoperative SD-OCT image at 3 months follow up. Discontinuity in outer retinal structures was detected postoperatively, as shown in the images.
View Figure 2
In our study, the closure rate of idiopathic large MHs (> 400 μm) was 100% after initial surgery of inverted ILM flap technique, which demonstrates similar results to previous studies. The introduction of ILM flap technique by Michalewska and colleagues [4] was recognized, in 2010. The flap was inverted upside down to be filled inside the FTMH and the fragment of ILM is attached to the FTMH’s margin. The closure rate was 98% in 46 eyes. Another study done in 2014 by Kumar, et al. [12] on 62 Indian people stated that the anatomical closure rate in idiopathic macular hole surgery using inverted ILM flap technique was 88.7%. In addition, Chakrabarti, et al. [13] found in their study in 2017 the closure rate of 100% in 26 eyes of MHs using the modified technique. In addition, two more comparative studies of internal limiting membrane flap inversion and internal limiting membrane peeling for macular holes, which was published in 2018 by Ota, et al. [7] and Kannan, et al. [8] showed the better successful rate of anatomical closure of 100% versus 93% and 90% versus 76.7% respectively. The most recent study by Carpineto, et al. [14] in 2021 revealed that the successful rate of anatomical closure in idiopathic MHs using inverted ILM flap technique was 93.75%.
Inverted ILM flap is one of the complex techniques which its mechanism of how it works is not well understood. Histopathologic studies confirmed that ILM being a base membrane acts as a scaffold for gliosis to close large MHs [15]. One experiment by Shiode, et al. revealed that the proliferation and migration of the muller cells was reinforced by the neurotrophic factors and growth factors that remained on the ILM flap surface, and the survival of retinal neurons and photoreceptor cells was maintained by the secretion by the Muller cells of neurotrophic and growth factors [16]. Thus, it is likely that Muller cell gliosis, and humoral factors could contribute to the closure of large MHs. Besides, the ILM flap seals the MH resulting from closing the communication between the vitreous and subretinal space, allowing the fluid to be pumped out effectively, thus lessening the leakage from the hole and eventually, drying out the fluid from the hole [17].
Functional outcome was evaluated according to the evolution of the visual acuity postoperatively and the improvement was comparatively 2.3 lines of Snellen chart. After 3 months follow-up, in a total of 22 patient, 54.5% experienced a significant visual gain from baseline value. The finding was corresponding to the result of study done by Kannan, et al. [8] in 2018, which revealed 53.3% of visual improvement in patients underwent ILM flap inversion technique. More studies demonstrated better visual outcomes using the same surgery technique. Kumar, et al, in 2014, showed that MHs patients had BCVA improvement from 0.94 ± 0.26 at baseline to 0.40 ± 0.23 logMAR at last follow-up with functional success shown in 88.7% of all patients [12]. In addition, Gu, et al. had done their systemic review in 2017 on eight journals of inverted internal limiting membrane flap technique and resulted in 75% of postoperative visual improvement rate [6]. Recent papers, moreover, supports the finding of improved functional outcomes of ILM flap inversion technique in MH patients. Bottini, et al. found that mean BCVA improved significantly from baseline to final follow-up visit [18]. Carpineto, et al. demonstrated in their paper done in 2021 that 93% of patients had an improvement of the visual acuity after the surgery [14].
In our study, there are limitations that should be taken into account. Small sample size is one of the main concerns of our study. However, as macular hole is an uncommon pathology, it is difficult to collect large sample size data operated by a single surgeon in one center study under a limited time period. Second, a very short follow-up period will provide an inadequate and biased result. To ensure a more accurate anatomical and functional result, longer follow-up period such as six to twelve months are encouraged in future studies.
In summary, this study showed that ILM flap inversion is a new and safe technique for idiopathic macular hole. The surgery resulted in a significant anatomical closure with better visual improvement in large macular hole. More importantly, the technique caused no severe ocular complications.
The authors declare no financial interest in this study.