The main objective of this manual is to describe and explain the Vision Screening Guidelines for Schools, (government, and private) in the State of Qatar.

It is a fact that the burden of visual disability among school age children; low vision and blindness, across the globe is significant, furthermore the condition of low vision is an important disability worldwide. School vision screening program has a great benefit in detection of obscure visual abnormalities which interfere with daily living activities of students and hinder their academic success and learning achievements. Schools are an ideal place to monitor the health of children. Screening is intended to facilitate early identification and diagnosis of disease and functional disorders. Visual impairment has an unfavorable implication on students’ eye health and will negatively affect their academic performance and learning skills. PHCC has a school health program that aims for integration of the “Health-Promoting School” program and includes a training package for school nurses and teachers. The number of health centers provide ophthalmology and optometry services is also being increased. In collaboration with the MEHE (private schools department) and the PHCC (school health department), the MOPH is adopting and developing a model of school eye health program at school clinics. Schools are being reminded about the screening program through letter and/or email from MEHE, prior to the beginning of a new academic year, nurses are further reminded by the team of Blindness Prevention Program (MOPH). The PHCC supplies the governmental schools with manpower (nurses), medical supplies and other requirements, furthermore, nurses are coordinating with school admins to facilitate the screening process. On the other hand, private schools are obligated to ensure the availability of licensed and qualified nurses. MOPH supplies the private schools with some requirements for vision screening (e.g., charts).
VA: Visual Acuity; Q: Qatari; NQ: Non-Qatari; MOPH: Ministry of Public Health; MEHE: Ministry of Education and Higher Education; PHCC: Primary Health Care Corporation; WHO: World Health Organization; DR: Diabetic Retinopathy; BPP: Blindness Prevention Program; RE: Right Eye; LE: Left Eye; HM: Hand Movements; PL: Perception of Light; HC: Health Center
Globally, world report on vision showed that 2.2 billion people have a vision impairment or blindness and at least 1 billion of whom have a condition which could have been either prevented or not yet to has been diagnosed [1]. Global Burden of Disease (GBD) Study ranked vision impairment as the third cause among all impairments for years lived with disability. Visual impairment constitutes a societal burden because of its impact on employment, quality of life and efforts related to caretaking, the two most avoidable causes of visual impairment are uncorrected refractive errors (42%) and cataracts (33%) [1-3]. It has been estimated that the annual global costs of productivity losses associated with vision impairment from uncorrected myopia and presbyopia alone are US$244 billion and US$25.4 billion, respectively. Vision screening in schools has been widely adopted by eye health programs in many countries. Almost 18.9 million students (World Health Organization WHO report), under 15 years of age are visually impaired globally [3]. The main objective of visual acuity screening in schools is to identify students with low vision or visual impairment that can affect their visual and intellectual (cognitive) development [4-6]. Screening for visual defects is an effective and important part of school health services, therefore it has been recommended to implement an annual survey, that is able to detect low vision and/or lazy eye conditions in school-age students, furthermore the early detection of such conditions helps in improving student`s academic performance and learning ability [7-15]. It is worthy to mention that about 80% of children with difficulty reading (dyslexia), have vision problems which can be resolved [16,17]. In Qatar, the visual disability accounts for around 15% of all disabilities [18].
Public health strategy 2017-2022 has been informed by an in-depth assessment of the health status of the population of Qatar [19]. It is essential that public health programs and initiatives are cognizant of interdependencies across diseases, health behaviors, risk factors and population characteristics. This strategy pledges to improve the health and wellbeing of the population across 63 objectives, one of them is the vision. Vision objective focuses on developing the needed eye care as an integral part of primary health care. The vision objective aims to comprehensive and effective eye health education and screening services for the population. Two important projects have been included in this objective: 1) The annual routine VA measurement program and 2) The annual updating of knowledge and skills of medical staff working at schools.
Ministry of Public Health (MOPH) conducts an annual vision screening survey in collaboration with Ministry of Education and Higher Education (MEHE) and Primary Health Care Corporation (PHCC), it aims to detect the magnitude of visual impairment in targeted students who enroll in government and private schools Visual acuity (VA) should be measured by vision screeners (usually registered school nurses) followed by referring the low vision students to health centers for further eye examination, alongside they should contact and follow-up with parents. VA measurement cannot determine the eyeglasses prescription required to correct vision; it is simply a measure of visual performance. The team of blindness prevention program at MOPH, coordinates this process and conducts periodically workshops to train vision screeners in how to measure visual acuity and to deal with common eye diseases or trauma.
The School Eye Health Program collaborators have been conducting an annual vision screening survey since 2008 in Government schools and 2012 in Private schools. A standard annual vision-screening protocol was administered in the governmental and private schools. The updated schools list with contact details needs to be obtained from the school affair department of MEHE. Blindness Prevention Program (BPP) team members usually contact all targeted schools through emails and telephone calls to remind them about vision screening guidelines. Vision screeners measure the VA, record data, and send the filled screening forms, subsequently, the members of BPP enter the data, analyze it, and do the reporting. During the academic year 2019-2020, around one hundred thousand students were included in the screening, divided into 48,179 in governmental schools and 51,482 in private schools. The visual acuity of 16,882 students (16.94%) was within the criteria of abnormal vision [19]. Distance visual acuity of both eyes was measured using the Snellen chart at 6 meters with E symbol in which the 6/6 line is the standard for normal vision. The rates of low vision students who had no spectacles among government and private school, were approximately 86% and 76% respectively. Students with abnormal vision measurement were referred to either the ophthalmologists or optometrists for further evaluation and treatment.
Visual acuity (VA) screening should be done annually to all students in grades, 1, 3, 5, 7, and 9.
- The VA screening should start during at the beginning of the first term of the school academic year (the first three months).
- Before starting the screening, a workshop will be provided to the new nurses and a refreshment course to the old staff, also nurses will be provided with materials summarizing the training.
- A communication email including any updated guidelines and regulations will be sent to PHCC ophthalmologists and optometrists as a reminder informing them regarding the start of the screening and keep them on the track of what will be the expectations.
The screeners usually are school nurses, they are delegated to implement and coordinate school health programs; they should be trained and get certificates as well. Untrained nurses are not allowed to perform this screening. The screener (nurse) has the following tasks:
- Discussion with school admins and school health supervisors to about day, time and location of the VA measurement, the required tools, needed materials and other special preparations. Furthermore, school nurses should explain to school admins about referral method, parents’ notification and follow up of low vision students.
- Preparation all required tools and materials. (Snellen chart, pointer, list of students etc.…)
- Measurement of visual acuity for the targeted students.
- Reexamine students with abnormal visual acuity at least one week from the initial exam.
- Recording the screening results on student’s health file/Cerner.
- Refer students with confirmed abnormal VA through filling the referral form/CERNER.
- Submission the VA screening report via email to MOPH and others.
- Follow-up with referred students.
The screener should select a spacious, quite room, (minimum of 6 meters length or 3 meters with a mirror), that could be school clinic, sports hall, classroom, or meeting room. A well-lit room is preferred with natural lighting (sunlight), any glare must be eliminated from the chart surface/location. Chart should be placed in a clean white wall and at the child’s eye level.
1. Show and allow students to familiarize themselves with the Snellen chart; explain the purpose and how the test is going to be performed, take the chart close to the student and explain that they should point at the direction of the “legs” of the E.
2. Let them know that this is not an exam to be passed, rather a way to see how their eyes are working. The important that they do not need to guess if they cannot see clearly. Tell them not to say the direction (left or right - up or down), they should match and show the direction of the “legs” of the E using their hand (Figure 1 and Figure 2).
 Figure 1: A vision screener illustrates to all students the methods of VA measurement.
View Figure 1
Figure 1: A vision screener illustrates to all students the methods of VA measurement.
View Figure 1
 Figure 2: The vision screening demonstrates the direction of E letter.
View Figure 2
Figure 2: The vision screening demonstrates the direction of E letter.
View Figure 2
1. Prepare the necessary tools for visual acuity measurement such as the E Snellen chart and pointer. The “Tumbling E” vision chart (six meters) is used as a standard chart in all schools, this chart uses a capital letter E that faces in different directions.
2.If a student normally wears eyeglasses (or corrective lenses) for distance, tell her/him to wear them during the test.
3. Mark off the six meters line, (measure the distance using the tape or rope provided). It may be marked with masking tape or paper feet print placed on the floor so that the student will be at the required distance from the chart. Do not allow him/her to lean their body or head forward or backward.
4. At the beginning, to make sure that students have understood the procedure, ask them to keep both eyes open and read the largest E (line 6/60).
5. Ask the student to cover their left eye, the student must be observed while being tested to get their full reaction, younger students may have a short attention span and get easily distracted by turning their head in other directions during the eye exam.
6. Begin with right eye, ask the student to cover his left eye with a tissue, students with refractive errors should wear spectacles during the test (if their spectacles are broken or lost, the test can still be conducted, but this must be mentioned in the report/referral form).
7. By using a pen or a pencil, point at the largest E letter (E on the line 6/60 which represents an acuity of 6/60 = 20/200) on the chart, ask the student “In which direction legs of letter ‘E’ pointing to?” (Figure 3). N.B. be careful during pointing; the tip of pen should be below the letter on chart.
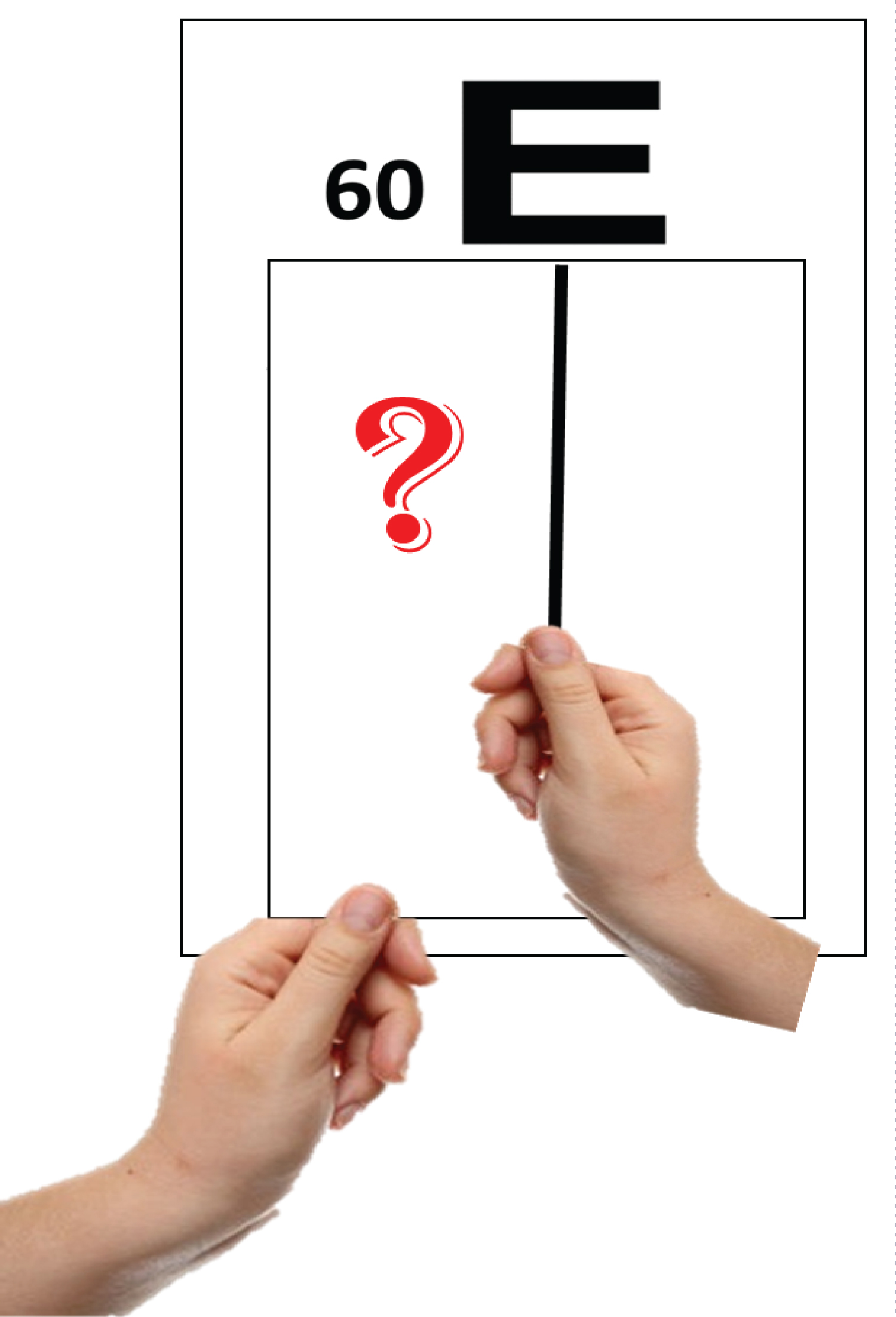 Figure 3: The largest E letter.
View Figure 3
Figure 3: The largest E letter.
View Figure 3
8. If the student fails the largest E letter, re-explain the procedure, if the student still cannot answer correctly, move him/her closer to the chart, 1 meter at a time, until the largest letter will be seen correctly; the VA will then be recorded as 5/60 if the distance is 5 meters, or 4/60 if the distance is 4 meters, etc.
9. If the student passes the E on the line 6/60, cover the chart and keep only one line (Figure 4). Continue asking for down the chart to reach the smallest letters in line 6/6 . If the student identifies at least four letters from the line 6/6 (more than half), he/she is considered to have normal 6/6 vision acuity. Take into consideration that students aged 5 years (grade 1 in some schools), have a normal VA of 6/9 (20/30), therefore do to not enforce them to read all letters in line 6/6, the normal visual acuity for them is 6/9; so, no need for referral.
 Figure 4: Isolation of horizontal line.
View Figure 4
Figure 4: Isolation of horizontal line.
View Figure 4
10. If the student fails to identify at least half of the number of letters in any line of the chart, therefore you should record the result as the line above.
• Example 1: The student was able to identify 2 letters out of 4 in line 6/18, (and was not able to identify half of the letters in the line below), therefore the result of VA measurement is 6/18.
• Example 2: The student was able to identify 3 letters out of 5 in line 6/12, (and was not able to identify half of letters in the line below), therefore the result of VA measurement is 6/12.
• Example 3: The student was able to identify 3 out of 6 letters in line 6/9 (and was not able to identify any letters in the line below), therefore the result of VA measurement is 6/9.
• Example 4: The student was able to identify only 2 out of 8 letters in line 6/6 therefore the result of VA measurement is the line above which is 6/9.
11. Students who failed to reach the age-appropriate visual acuity will need to be re-tested in the next week with more quiet conditions and preferred to be in the morning to confirm the results before referring to the health Center (HC).
1. You need to memorize some important abbreviations such as, right eye = RE, left eye = LE, hand motion (HM), VA is recorded as HM, when the low vision student sees only hand motion of the screener, perception of light = PL. In case if a student has severe eye trauma or congenital anomaly of one eye and he/she cannot see the light in this eye, VA will be recorded as no perception of light (NPL ).
2. Distance VA should be tested with correction or spectacles for those students’ using glasses. In the report it will be recorded “vision with glasses” or without correction for students not using glasses “vision without glasses”.
1. The VA checkup option was included in CERNER under the visit reason (Figure 5).
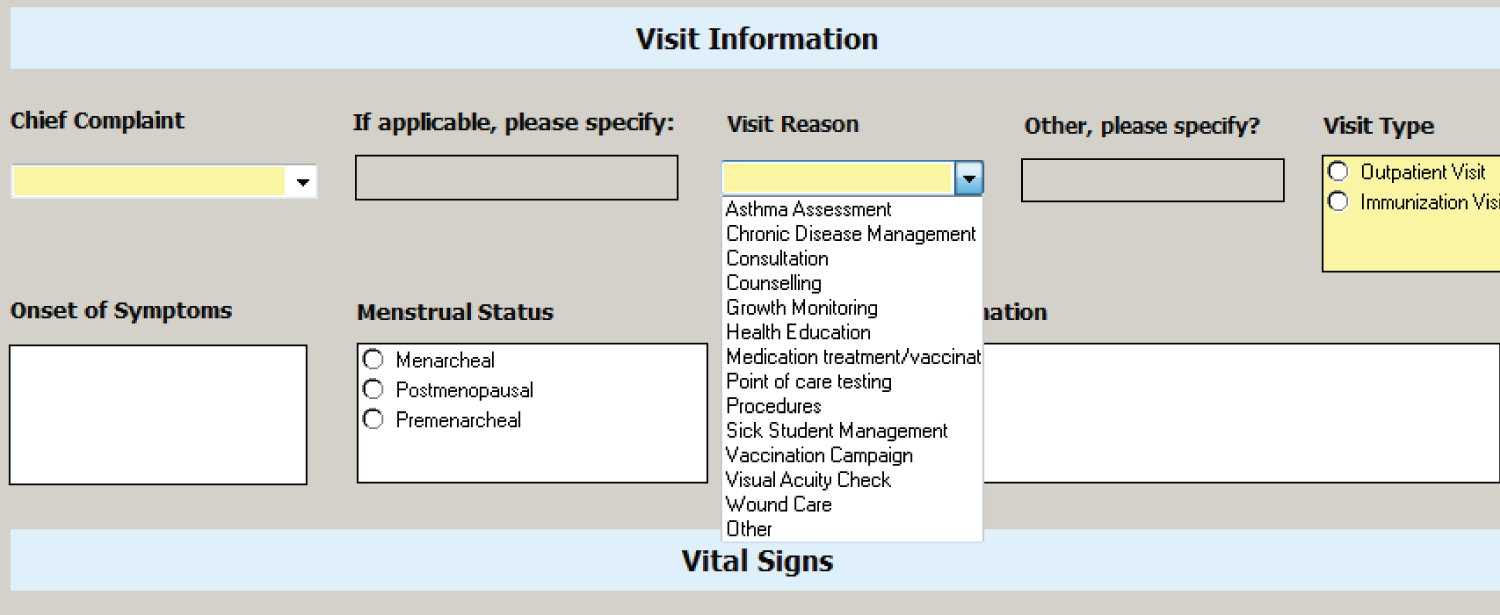 Figure 5: Selection the visit reason.
View Figure 5
Figure 5: Selection the visit reason.
View Figure 5
2. Select the level (KG, Primary-Elementary-Secondary) and grade of student (Figure 6).
 Figure 6: Selection the student's level and grade.
View Figure 6
Figure 6: Selection the student's level and grade.
View Figure 6
3. Record the VA by selecting the appropriate value from the dropdown list (Figure 7).
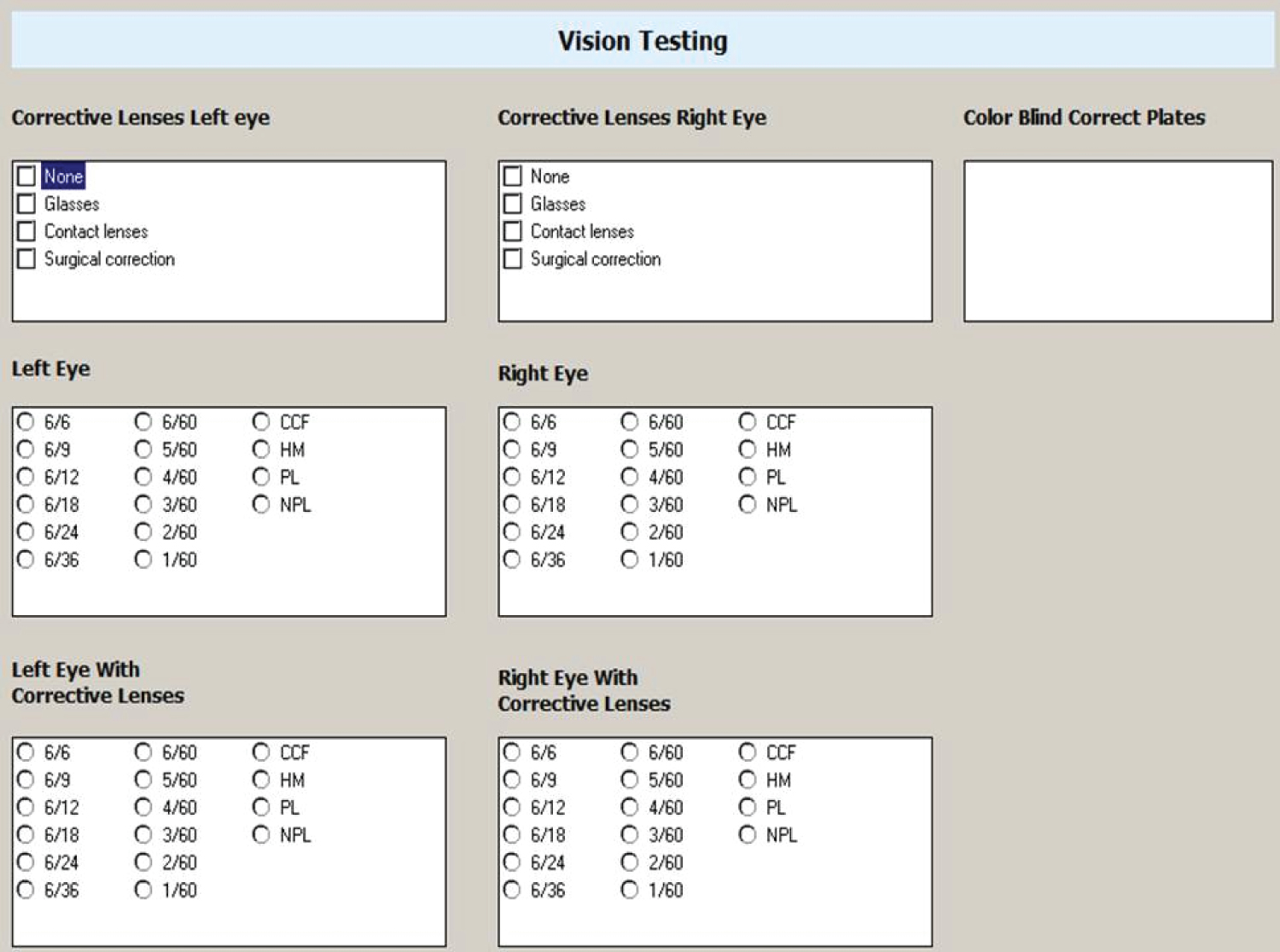 Figure 7: Selection the visit reason.
View Figure 7
Figure 7: Selection the visit reason.
View Figure 7
4. At the end of academic year (March- April), the MOPH will receive the data of all schools from our colleagues at school health department (PHCC).
1. MOPH vision screening report, is an excel workbook consisting of the following three worksheets:
A. Precautionary measures for COVID-19.
B. Form A (Figure 8 and Figure 9) for students with vision acuity 6/9 or less.
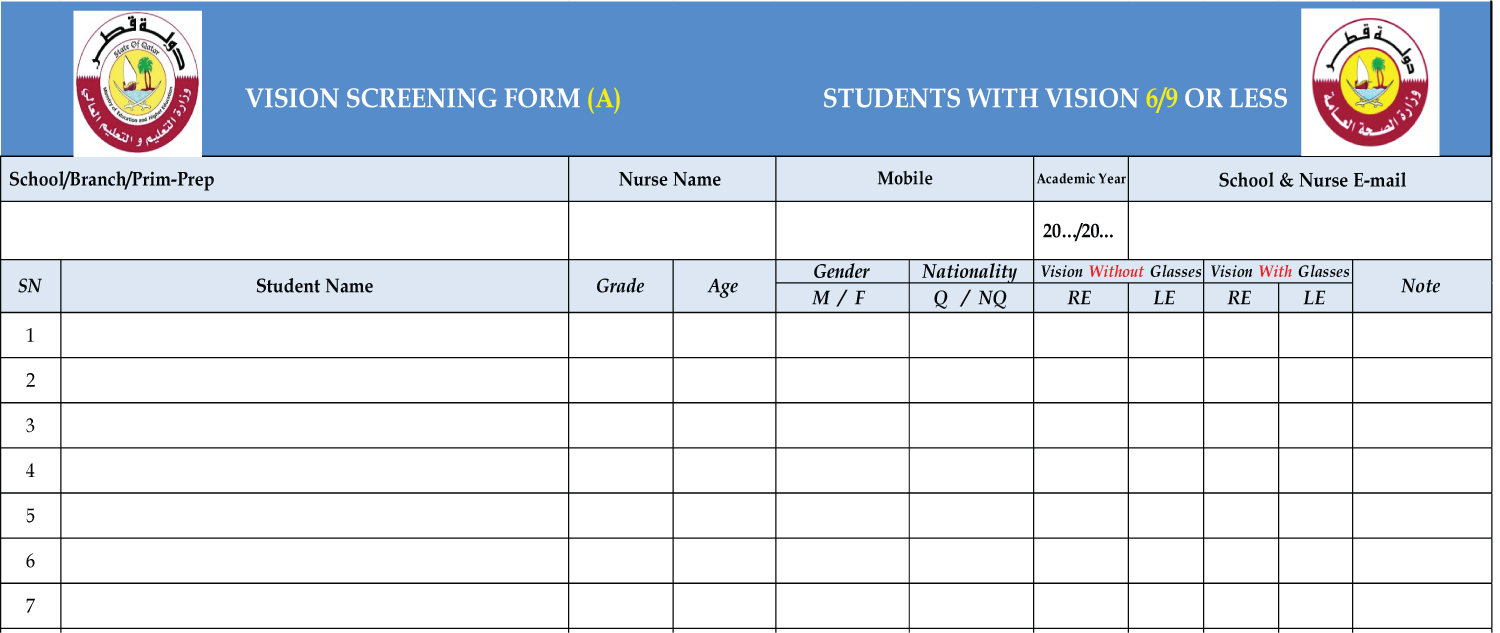 Figure 8: Form A for visually impaired students.
View Figure 8
Figure 8: Form A for visually impaired students.
View Figure 8
 Figure 9: Form A for visually impaired students.
View Figure 9
Figure 9: Form A for visually impaired students.
View Figure 9
C. Form B (Figure 10 and Figure 11) for students with normal vision acuity (6/6).
 Figure 10: Form B for normal vision students.
View Figure 10
Figure 10: Form B for normal vision students.
View Figure 10
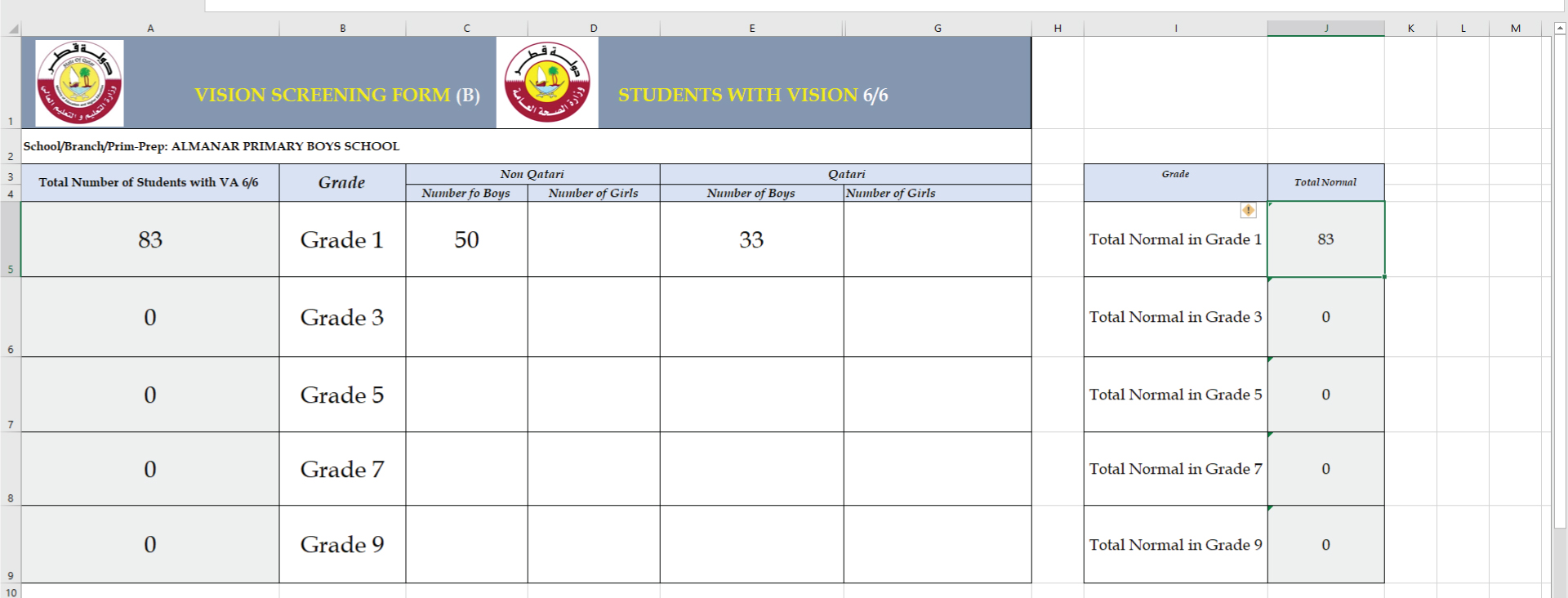 Figure 11: Form B for normal vision students.
View Figure 11
Figure 11: Form B for normal vision students.
View Figure 11
2. To access and fill the screening forms, you should use the Microsoft EXCEL program.
3. Write the full name of the school, and branch if exist.
4. Fill data of each student in a separate row, use the acronym to describe gender (M = Male, F = Female) and nationality (Q = Qatari, NQ = non-Qatari).
5. Fill the students age and grade in numbers, (e.g., 7 for the student who is 7-years-old).
6. Screen all students in target grades as mentioned above, then divide the collected data into two groups:
a. Normal vision students (should be filled in FORM B)
b. Abnormal vision students (should be filled in FORM A).
7. FORM A has two columns, Vision without Glasses and Vision with Glasses.
8. Students who have any refractive errors and wear glasses (or contact lenses), should be screened with glasses. In case if visual acuity is 6/9 or less, fill data in FORM A, (Vision with Glasses column). On the other hand, if visual acuity is 6/6, data needs to be filled in FORM B. Take into consideration that students aged 5 years (grade 1 in some schools), have a normal VA of 6/9 (20/30), and do not need a referral.
9. Students who failed to reach the age-appropriate visual acuity will need to be re-tested in the next week with more quiet conditions and preferred to early in the morning to confirm the results before referring to the ophthalmologists.
10. When visual acuity measurement and forms filling processes are finished for all students, kindly send data as a single attached excel file to the following addresses: -
11. mkhalfallah@MOPH.GOV.QA Mzoughi Khalfallah
12. BPP@MOPH.GOV.QA Blindness Prevention Program
13. Subsequently, you will receive an acknowledgement email reply.
14. For all inquiries, please contact Mr. Mzoughi Khalfallah mkhalfallah@MOPH.GOV.QA Tel: 44070645.
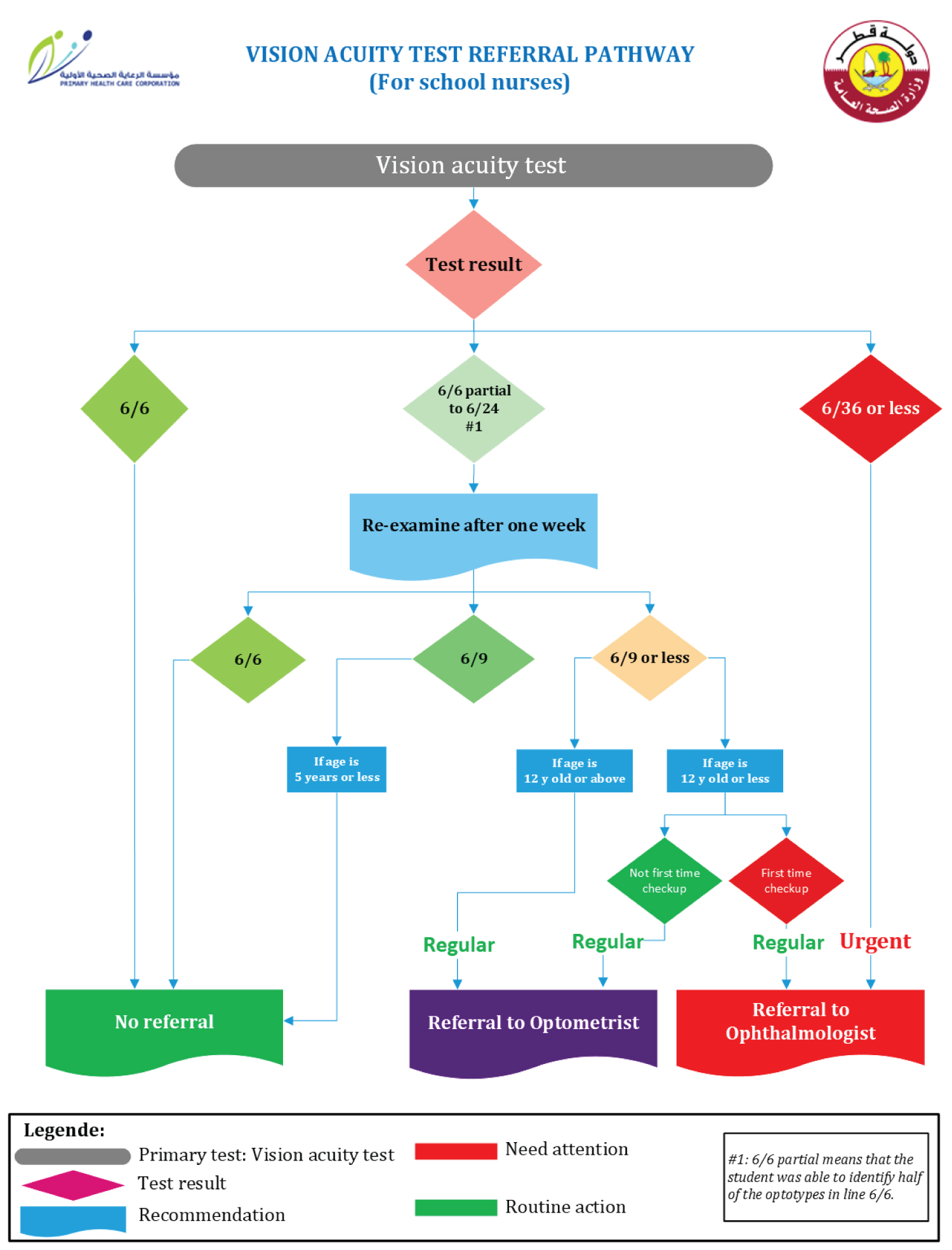 Figure 12: Referral pathways flowchart.
View Figure 12
Figure 12: Referral pathways flowchart.
View Figure 12
1. Any student with VA 6/9 line or worse needs to be referred to the specialized clinic in PHCC, except for 5 years aged students (year one in some schools) will be referred if visual acuity is less than 6/9.
2. The referral will be routine unless VA result is 6/36 or less, or there is a sudden drop of VA in one or both eyes, in this case referral will be urgent.
3. For students 12-years-old or less whom will be tested for the first time will be referred to the ophthalmologist.
4. For students 12-years-old or less who have glasses but not been followed up in the last 6 months or their vision not reaching 6/6 with the glasses will be referred to the optometrist.
5. Students who are older than 12 years age or already had glasses (whatever the age) will be referred to the optometrist.
6. Referral will be to student`s registered health center (if no ophthalmology clinic in HC, referral will be referred to other HC in the same region with ophthalmology clinic) and student must be escorted with parents or care givers.
7. For school nurses in governmental schools, an electronic referral order on Cerner will be placed with routine priority selection, and parents are expected to take the appointment from the HC assigned by the school nurse or to call 107 to take the appointment (to be noticed the appointment will not be in the same day so the parent doesn't need to get their child with him when taking the appointment.
8. Parents need to be oriented and explained about the importance of vision screening of their children.
9. Parents instructed to have a routine appointment with ophthalmology or optometry according to the referral form provided from the school nurse, followed by returning the form back with the results.
10. The parents requested to have the referral form with them at the day of the examination, the form needed to be filled up by the ophthalmologist or optometrist. The filled form will be returned back by the student to the school nurse with the result of the examination.
11. At the level of the HC, if glasses to be prescribed then follow up appointment will be booked on the same visit day.
12. Private school nurses can formalize their own Ophthalmology Referral Form and write the important information.
13. The follow-up report helps in forming a clear idea of the effectiveness of the program, furthermore, statistics of real number of students with low vision, will be a baseline data for future studies.
14. School nurses need to follow up all referred students and insert (add) the result of examination been done in the HC (this follow up result should be added to the report that to be sent to MOPH.
15. The results can be obtained either from the form that returned by the student after the examination, or from Cerner.
16. To document the results, the nurse needs to enter the results into one of the following categories:
1. Normal exam
2. Border line and no glasses for now but follow up
3. Glasses prescribed and for follow up
We would like to thank all our colleagues, partners, and others for their support in implementation of school screening program, we are grateful to our colleagues working for school health department (PHCC) and nurses of government and private schools for their cooperation. We also convey our thanks to school affair departments at Ministry of Education and Higher Education for their coordination during the annual vision screening in schools.
The authors declare no conflict of interest related to the content of the Guidelines.
The author did not receive any external funding related to the guidelines.