Using a safer alternative guide material in the operating room for silicone intubation in case of dacryosistorhinostomy operations and in case of ptosis surgery with poor levator function.
The metal probes of the silicone tube that we use in dacryocystorhinostomy operations can sometimes break off during the surgery. In order to prevent material waste by opening the second tube, or sometimes the 2nd tube is not available, we tried to use 18-gauge, intravascular catheter as a guide material. And after removing the port part of the catheter, it is introduced together with the lacrimal prob into the punctum and advanced to the rhinostomy site and then silicone tube inserted into the catheter. We also tried to use the 18-gauge, intravascular catheter, as an alternative guide material for Wright needle in case of Frontal sling surgery. After insertion the catheter, the needle withdrawn and silicone rode introduced through the catheter easily via a closed-insicion pentagonal configuration.
Twenty of dacryocystorhinostomy patients and 10 of ptosis patients were analyzed. There were no intraoperative or postoperative complications associated with the insertion of catheter, such as punctal erosion, corneal erosion, granuloma formation, adhesion in the canalicular system, or iatrogenic canalicular laserations. Also in ptosis surgery the average surgical time was short and there were no intraoperative or postoperative complications associated with the insertion of catheter, such as edema, hematoma, echymosis or allergic reactions.
Using an intravascular catheter, as a channel to place the silicone tubing into the nasolacrimal system in case of dacryocystorhinostomy operations and also in frontal sling operations, is not only inexpensive but also effortless with no complications.
Dacryocystorhinostomy, Frontalis sling surgery, Silicone stent
Bicanalicular silicone tube placement and frontal sling material are widely used in dacryocystorhinostomy (DCR) and also in ptosis surgeries. In DCR operations silicone tube aims to maintain canalicular or anastomotic patency during the healing period and may improve surgical results when used appropriately [1-3]. Prepackaged set consisting of silicone tube attached to metal probes is commonly used for silicone intubation [1,4]. The disadvantages associated with this device is that it is expensive and sometimes the metal end of silicone tube can break off during the surgery [1].
Another clinical condition is blepharoptosis, which causes many psychological and visual problems. Correct diagnosis and treatment can prevent possible amblyopia through visual deprivation in patients with severe [5,6]. Frontalis sling surgery, as described by Fox, can be used for the surgery, along with various materials [5,7]. Silicone rods produce little tissue reaction and are elastic, thus allowing the patient´s eyes to close properly through the contraction of the orbicularis muscle. Another advantage of the silicone rod is the fact that we do not need to use another surgical site on the patient, as in the withdrawal of fascia lata or fascia temporalis, which would improve the mobility [5].
Here, we would like to talk about an easy and at the same time economical method of inserting a tube into the nasolacrimal system using the intravenous catheter as guide material and also its pratical use in ptosis surgery.
The medical records of 30 reviewed restrospectively. The study protocol adhered to the tenets of Declaration of Helsinki and was approved by the ethics committee. Patient consent to publish identifiable photograph archival was taken. The patients demographic information, clinical history, visual acuity, indication for surgery, duration of follow up, complications encounterred during the follow-up period were all noted.
Patients were operated under general or local anesthesia. In DCR operations the metal probes of the silicone tube, can sometimes break off during the surgery. In order to prevent material waste by opening the second tube, or sometimes the 2nd tube is not available, we tried to use 18-gauge, intravascular catheter (45 mm length with 0.90 mm inner diameter and 1.3 mm outside diameter), a very small, flexible tube which is designed for placing into veins, as a guide material to place a silicone tubing into the nasolacrimal system. The lacrimal puncta is enlarged using puctum dilalator (Punctum dilator/Lacrimal probe has 0.28 mm × 25 mm Dilator part, 0.7 mm × 44.5 mm Probe part, and 70 mm Handle part). And after removing the port part of the catheter, it is introduced together with the lacrimal prob into the punctum and advanced to the rhinostomy site and then silicone tube, which is comprises of two flexible stainless steel wires 0.40 mm diameter and a hallow silicone tube with an outside diameter of 0.64 mm and a 0.30 mm lumen, inserted into the catheter. The other canaliculus is intubated in similar manner. The tubes are passed out through the rhinostomy site and nose, and tied inside the nose (Figure1).
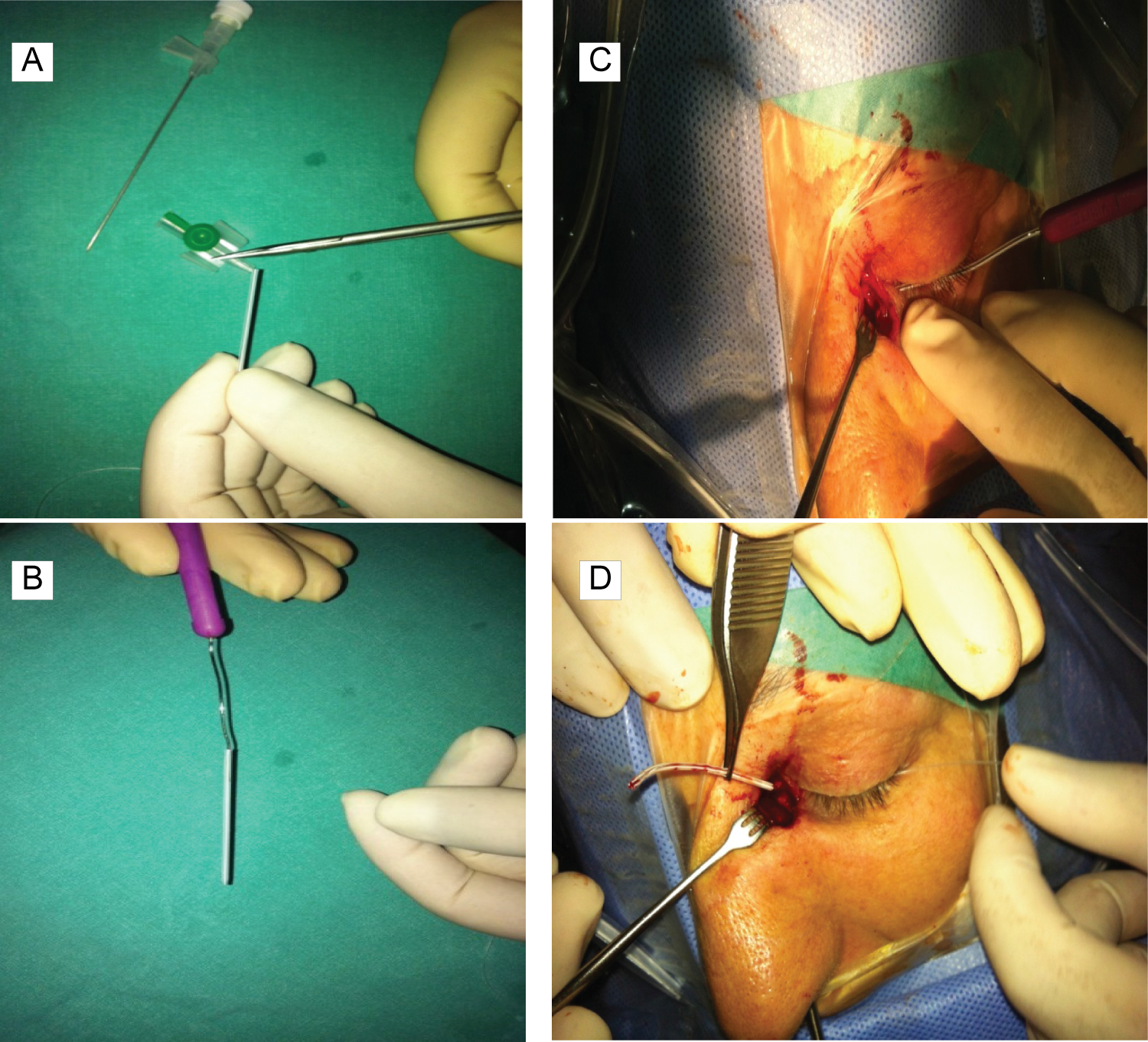 Figure 1: (A-D) The preparation and insertion of the 18-gauge intravenous catheter with silicone tube into nasolacrimal system.
View Figure 1
Figure 1: (A-D) The preparation and insertion of the 18-gauge intravenous catheter with silicone tube into nasolacrimal system.
View Figure 1
We also tried to use 18-gauge, intravascular catheter, as an alternative guide material for Wright needle in case of Frontal sling surgery. A fox pentagon was used with five stab incisions using no. 11 blade, two in the eyelid, two in the superior eye-brow margin, and one in the forehead. After removing the port part of the catheter, the 18-gauge intravenous catheter was inserted through the incision site, then the needle withdrawn and silicone rode introduced through the catheter lumen easily to be placed deep to the orbicularis and frontalis muscle (Figure 2).
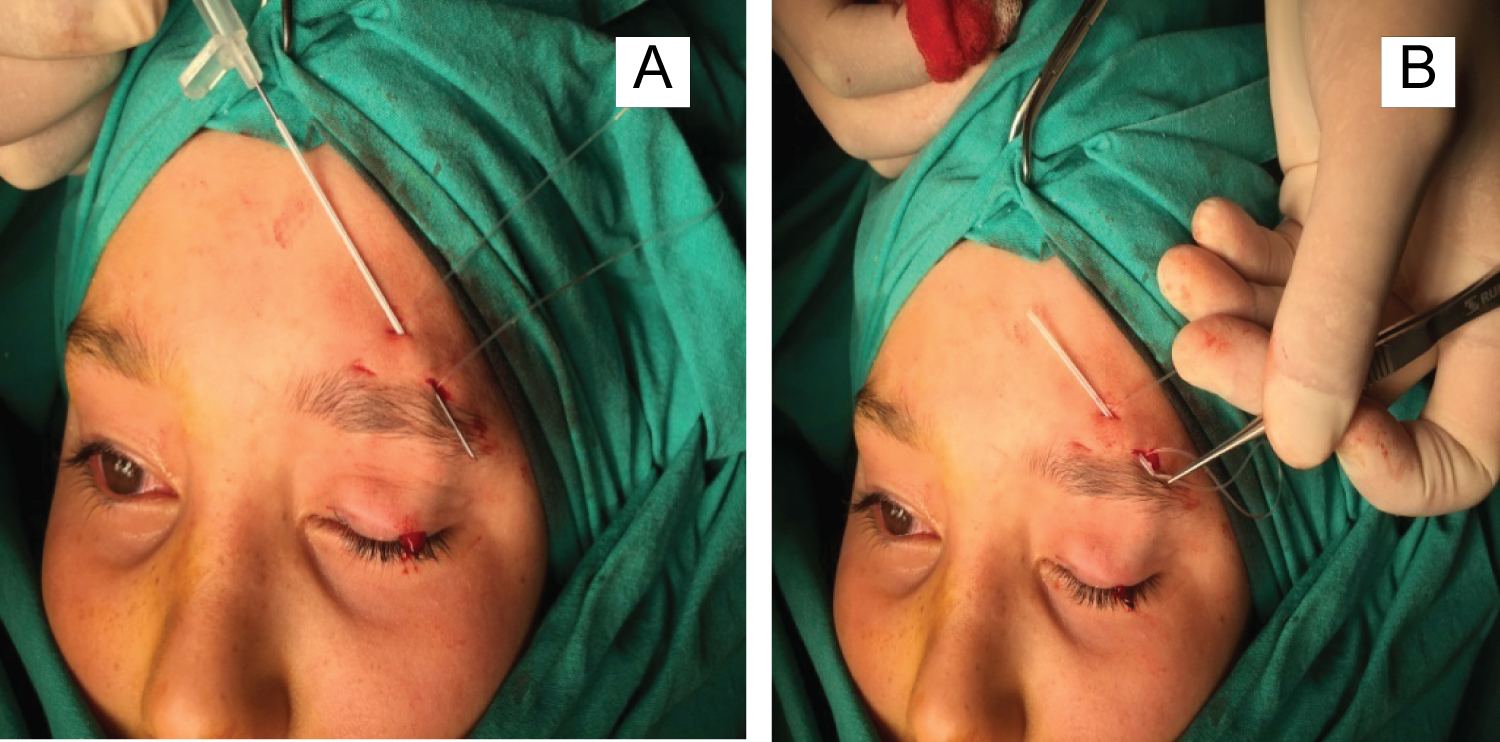 Figure 2: (A,B) 18 gauge intravascular catheter was used as a guide for insertion of silicone rods.
View Figure 2
Figure 2: (A,B) 18 gauge intravascular catheter was used as a guide for insertion of silicone rods.
View Figure 2
Twenty of DCR patients with aged 45-55 years and 10 of ptosis patients, aged between 10-30 years. were included in the study. Each patient undergoing external DSR surgery was routinely placed with a bicanalicular silicone tube. All DCR patients were free of symptoms and signs after insertion of silicone tubing.There were no intraoperative or postoperative complications associated with the insertion of catheter, such as punctal erosion, corneal erosion, granuloma formation, adhesion in the canalicular system, or iatrogenic canalicular laserations.
Also in ptosis surgery the main advantages noted intraoperatively were easy maneuverability and control of the catheter during tissue passage and smooth threading of the silicone rod. The average surgical time was short and there were no intraoperative or postoperative complications associated with the insertion of catheter, such as edema, hematoma, echymosis or allergic reactions.
Many surgical techniques and instruments for stent placement have been described. The material of choice for stenting in the lacrimal system is silicone, which is generally inert within the system [8,9]. Stents implanted with in nasolacrimal system prevent adherence of the mucosal lining of the ducts during healing and maintain long term patency after removal [8,10].
Various sets and methods have been described for lacrimal intubation [1,11,12]. The O'Donough, Quickert and Crawford intubations sets are the most commonly preferred ones [1]. In these sets, silicone tubes are attached to metal probes ranging in length from 45 mm to 177 mm, and while inserting one of these tubes, the metal probe passes from the canaliculi first and the silicone tube follows it. To place the tube, it is necessary to pass the whole probe from the canalicular segment and to retrieve it from the rhinostomy site [1]. Although curved and shorter metal probes are used, there are some difficulties in the manipulation of the metal probes. The difficulty in retrieving the probe from the wound and the nose, possible canalicular trauma, and relative expense are the main disadvantages of this method [1].
Archer and Hurwitz have suggested a different intubation method for external DCR surgery [13]. In this method, a lacrimal probe (Bowman No. 1 probe, 0.90 mm in diameter) is used for passing the tubes through the canaliculus. The outer diameter of the silicone tubes is 0.94 mm. Oblique incisions are made 3 mm away from the ends of the tubes. The lacrimal probe is inserted into this incision and advanced about 2 mm. The probe with the tube is inserted into the punctum, advanced through the canaliculus, and pulled out from the cavity of the sac. The disadvantages of this technique include the difficulty in adjusting the length of vertical incision on the tube, inserting the metal probe into the incision, and breaking of the fragile part at the end of the tube. In addition, it may be difficult to pass the lacrimal probe attached to the silicone tube through the relatively narrower canaliculus [1].
Yıldız, et al., described an alternative techique, in which the silicone tube is advanced in front of an introducer, i.e. a lacrimal canula. They used a canula 0.45 mm in diameter, and inserted into the silicone tube. Enlargement of the lacrimal punctum with one snip facilitates both the entrance of the silicone tube and postoperative lacrimal irrigation [1].
Other alternative methods to silicone intubation are known as T-sheet made from a penrose drain tube, otologic T-tubes, polypropylene suture material have also been used to retain the lacrimal aperture following DCR [9].
During lacrimal intubation, the metal probes may easily cause canalicular injury. To avoid this complication, the tubes should be advanced gently according to the trace of the canaliculus [1].
In our technique, 18-gauge, intravascular catheter was used as a guide material to place a silicone tubing into the nasolacrimal system. Silicone tube can be easily inserted into the catheter, and forms a relatively tight connection. Enlargement of the lacrimal punctum with punctum dilatator the catheter introduced into the punctum and then silicone tube inserted into the catheter and advanced to rhinostomy site. In DCR operations the metal probes of the silicone tube, can sometimes break off during the surgery. The main advantages of this technique is to prevent material waste by opening the second tube, or sometimes the 2nd tube is not available, and also no canalicular damaged was observed.
We also used intravenous catheter in ptosis surgery with poor levator function. As it's known, either synthetic materials or autologous tissue are used to perform frontalis suspension and the most commonly used instrument to introduce these materials is the Wright needle [14,15]. As the Wright needle requires a bigger skin wound and causes more trauma, 18-gauge intravenous catheter was used in surgery, and mentioned some advantages of this material, such as smaller size means better cosmetic result and less trauma, it is cheap and disposable, the tip is always sharp because it is not re-used [5,15].
Alhady, et al., described a technique in which they used 2/0 prolene suture as a sling material and introduced it through the 18-gauge needle lumen to be placed deep to the orbicularis and frontalis muscle [15]. The disanvantage of 18 gauge intravenous catheter, they said that, as the lumen of the needle is small, it cannot be used from the introduction of larger materials, such as fascia lata or mersilene mesh. The other reason is that the needle is straight and may be difficult to use in adult who has a prominent forehead. They said that bending the needle with an artery forceps can get around the problem [15].
What alternative instruments may be used to reduce scarring and swelling? Some investigators used epidural needle in place of Wright needle, some used 18 gauge hyodermic needle as a simple and cost effective alternative tool in frontalis slicone suspension ptosis surgery, 18 gauge intravenous catheter needlei and abdominal needle [5,14-16]. The disadvantages of epidural needle is that, it is long and very flexible maxng creation of a straighy track difficult and it is many times the cost of an intravenous catheter needle [15]. The advantages of 18-gauge intravenous catheter needle is a cost effective, safe, and a better cosmetic result reducing the incision scars and tissue swelling [15]. In the passage of the silicone rod, Eduardo, et al., used a curved eyed needle instead of Wright needle. Therefore, the depth of the passage of the rod can be better controlled, avoiding eye injuries [5].
As mentioned in the Goel, et al., study silicon sling has gained wide spread acceptance due to its ease of use, less surgical time and minimal patient morbidity [14]. They produce little tissue reaction and are elastic, thus allowing the patient´s eyes to close properly through the contraction of the orbicularis muscle. Another advantage of the silicone rod is the fact that we do not need to use another surgical site on the patient, as in the withdrawal of fascia lata or fascia temporalis, which would improve the mobility [5,17].
It is stated that the silicon rods, during the passage became blunt and at times get detached from the stainless steel portion [14]. It is also mentioned that when the needle is passed upwards from lid towards the brow leading to frequent detachment of silicon rod [14].
In our study, we prefer to use silicone stent as it has a better bio-integration with the tissues. While inserting it through the incision site we used 18-gauge intravenous catheter, and silicone rode is introduced through the catheter lumen easily to be placed deep to the orbicularis and frontalis muscle. It is a simple, effective, safe and low-cost technique and also prevents all the problems about the silicone rod, such as they become blunt, not easy to pass the needle upwards from lid towards the brow and the frequent detachment of silicon rod as it is mentioned in Goel, et al., study [14].
We describe a new technique of managing 18 gauge intravenous catheter allowing smooth passage of the silicone rod in DCR and also in ptosis surgery. The intravenous catheter, which is very easy to supply, is a life-saving problem when we experience a problem with the material we use during the surgery. It is not only inexpensive but also effortless with no complications.
I'm grateful to all with whom I have had work together.
The author has no relevant affiliations or financial involvement with a financial interest in or financial with the subject matter or materials discussed in the manuscript.
The study protocol was approved by the Ethics committee of Kartal, Lutfi Kirdar Education and Training Hospital, Istanbul, Turkey (decision number).
There is no conflict of interest.