Fibrous dysplasia (FD) commonly affects the craniofacial structures including the orbit. Rarely, growth involving the orbital apex can cause intra-orbital or intracanalicular optic nerve compression leading to permanent vision loss. Any sign of optic nerve compression is an indication for surgical resection. We report a case of compressive optic neuropathy secondary to craniofacial FD that was treated with combined endoscopic and trans-orbital resection as well as orbital wall and facial reconstruction, a novel technique for optimal management. Surgical challenges including avoiding thermal and mechanical injury to the optic nerve, reduced access to the posterior medial orbital wall, and meticulous reconstruction of the medial and inferior wall were overcome by the combined approach. A successful functional and aesthetic outcome was achieved post-operatively with evidence of visual improvement.
Endoscopic, Trans-orbital, Fibrous dysplasia, Resection, Reconstruction
Fibrous dysplasia (FD) is a benign, dysplastic process of altered osteogenesis that replaces normal bone with abnormal fibrous tissue and immature trabecular bone [1,2]. It can affect any bone in the body, with craniofacial involvement occurring in about half of cases. Of the craniofacial bones, the maxillary bone is most commonly affected [3]. The mass can aggressively grow into the orbital floor causing diplopia, globe displacement, and in severe cases, vision loss. These lesions are sometimes asymptomatic and detected incidentally; however, they can also be severely disfiguring and disabling. While surgical debulking and resection are the mainstay of treatment in vision-threatening conditions, indications for surgical intervention are poorly defined. Current guidelines are based upon the size and location of the lesion itself; however, surgical consideration should instead depend on factors such as symptoms, appearance, and patient needs. For example, the presence of neurologic symptom warrants surgical intervention even if guidelines would advise against such [4]. Nonetheless, the literature consensus is that optic nerve compression is an indication for surgical resection [5].
The optimal surgical technique has been debated with both radical resection and conservative debulking techniques being described in the literature [6,7]. Although conservative approaches may be complicated by recurrence, it is often difficult to treat extensive cases by complete resection due to risk of complications such as optic nerve damage and hemorrhage [8]. We report a case of recurrent craniofacial FD with optic nerve compromise that was surgically resected via combined external orbitotomy and endoscopic approach. Patient consent to obtain photographs was obtained and archived. All collection and evaluation of patient health information were HIPAA-compliant, and this report adheres to the Declaration of Helsinki.
A 21-year-old male with a history of histo-pathologically confirmed FD of the maxilla status post-surgical debulking presented with diplopia, proptosis, orbital pain, and gradual vision loss in the left eye over three months. On ophthalmic examination, his best corrected visual acuity (BCVA) was 20/20 and 20/40 in the right and left eyes, respectively. A relative afferent pupillary defect (RAPD) was detected in his left eye. Extraocular motility was intact, but the left globe was displaced supero-temporally resulting in telecanthus. Decreased sensation of the left cheek was detected on neurologic examination. On fundus exam, there was Frisen grade 3 edema of the left optic nerve. Ishihara test showed decreased color vision in the left eye. Visual field testing of the left eye revealed scattered, non-specific deficits.
Computerized tomography (CT) scan of the orbits showed a heterogeneous mass with calcifications and well-defined margins involving the left maxilla and ethmoid sinuses extending to the orbit medially and to the cribriform plate superiorly (Figure 1). There was evidence of medial and inferior optic nerve compression by the mass. Given the decline in BCVA and RAPD in the left eye with optic nerve edema suggesting visual compromise, the decision was made to proceed with tumor debulking.
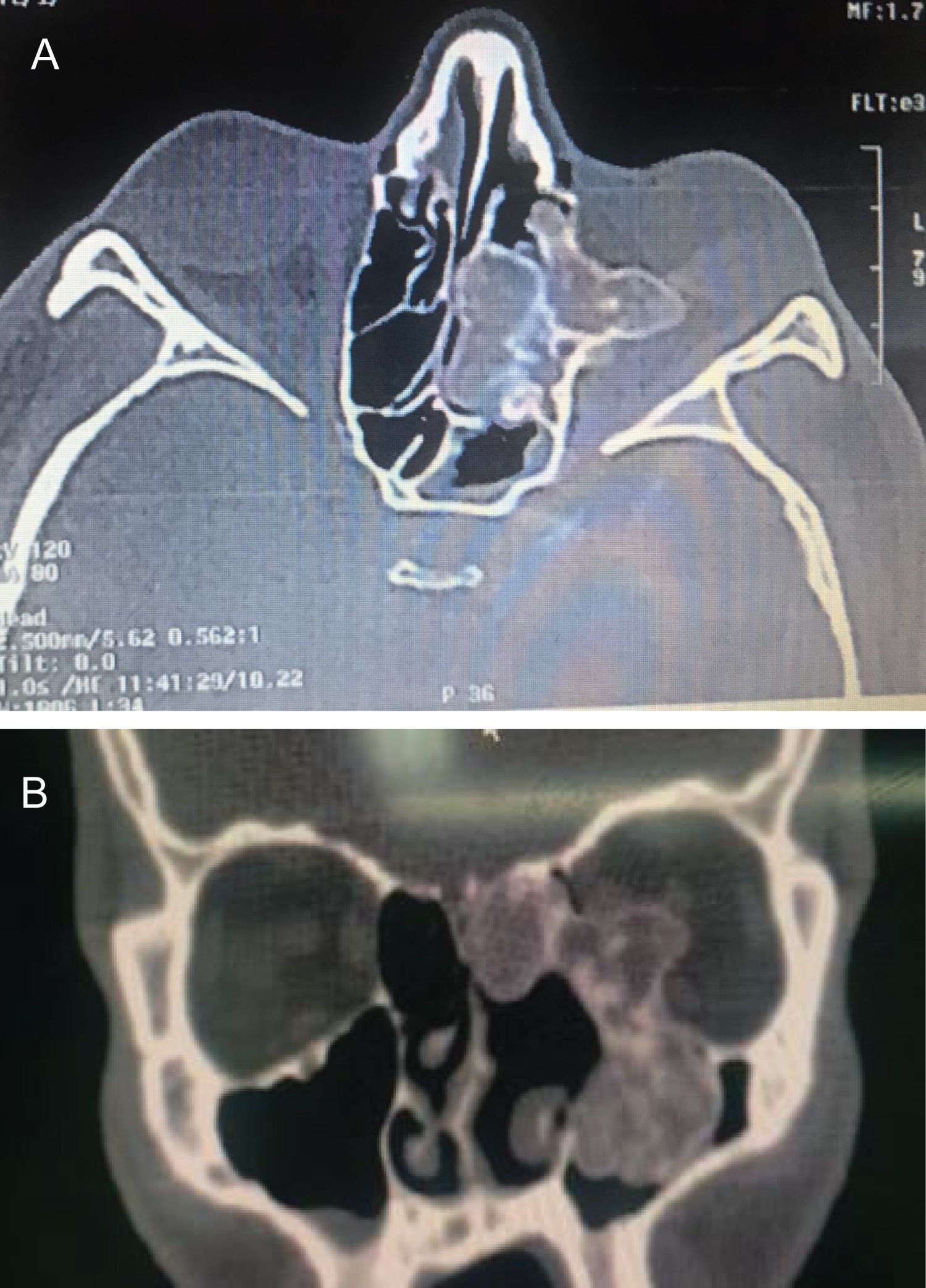 Figure 1 (a): Axial orbital CT scan showing extension of a heterogeneous bony mass through the retrobulbar space extending across the intraorbital optic nerve.
Figure 1 (a): Axial orbital CT scan showing extension of a heterogeneous bony mass through the retrobulbar space extending across the intraorbital optic nerve.
Figure 1 (b): Coronal CT shows inferomedial optic nerve compression by the mass.
View Figure 1
A multimodal endoscopic, endonasal, and trans-orbital approach was used with insertion of a 0-degree endoscope into the left nostril. The multi-lobular mass occupying the middle meatal area was encountered, and the mucosal lining was dissected off the surface. The ethmo-sphenoidal portion of the mass was debulked by anterior drilling until the sphenoid sinus was exposed and proceeding posteriorly until the intra-orbital mass was identified. The lesion was carefully resected superiorly from the cribriform plate by gentle staged endoscopic drilling, leaving behind some residual lesion at the cranial base. No leakage of cerebrospinal fluid was noted.
A transconjunctival, inferior orbitotomy was performed inferior to the tarsal border using Wescott scissors. The dissection was carried through the insertion of the lower lid retractors and inferiorly toward the orbital rim. Once the dissection reached the level of the orbital rim, a malleable retractor was used to retract the orbital tissues. An incision was made through the periosteum, which was dissected off the bone to expose the mass invading the orbital floor. A hole was made through the mass with an osteotome to facilitate visualization, and the orbital floor portion was resected and delivered through the nostril using concurrent endoscopy. A hook was used to shield and protect the optic nerve during resection of the mass. Additional tissue was resected from the lateral wall of the maxillary sinus with a high-speed drill via this concurrent orbitotomy and endoscopic approach. The conjunctival incision from the inferior orbitotomy was extended through the caruncle to create a continuous medial orbitotomy for better exposure. The globe was gently retracted with a malleable retractor, and subperiosteal dissection was performed along the medial wall for improved visualization. The optic nerve was protected from the heat and vibration of the drill with a malleable retractor covered by a multi-layer plastic material. The medial wall mass was then removed via high-speed drilling, and continuous visualization of the mass and optic nerve was made possible with the endoscope. The residual mass was delivered into the nasal cavity and removed with straight nasal forceps. A mesh implant was used to reconstruct the medial wall and floor defects. It was trimmed to an appropriate size and shape, bent to simulate the natural orbital curve, and fixed to the orbital rim with titanium screws.
At this point, orbital fat was visualized herniating into the nasal cavity with the endoscope, which was re-positioned into the orbit. At the end of the case, forced ductions were tested, which were normal. The case was concluded by suturing of the conjunctival and caruncle incisions.
At one-week follow up, BCVA improved to 20/25 in the left eye, and the diplopia had resolved. On 6-month follow-up examination, the optic disc swelling, and RAPD had resolved. Subsequent visual field testing was normal in both eyes. The patient reported no symptoms at last follow-up of 1 year via telemedicine due to geographic circumstances.
FD is a slowly proliferative, fibro-osseous mass, caused by disorder of the adenylyl cyclase system secondary to an activating mutation in the GNAS gene [9]. It can involve the orbital walls in a monofocal or multifocal manner and may cause permanent vision loss via compression of the intra-orbital or intra-canalicular segments of the optic nerve [1,2]. While some authors support prophylactic decompression of the optic canal prior to evidence of optic nerve compression, others believe that compressive optic neuropathy is a rare complication and surgical intervention is not necessary until there are signs of visual compromise [8]. In patients with impending visual compromise, prophylactic resection and decompression may be considered if the patient is already undergoing resection of an anterior skull base lesion [10]. Either way, there are limited treatment options for advanced cases of FD with orbital involvement. A recent report by Dr. Cho, et al. highlighted a technique with the assistance of an endoscope in resecting a maxillary sinus FD mass via a trans-oral gingivobuccal and navigation system approach [11].
Few nonsurgical options exist to treat orbito-facial FD. Radiotherapy has not been shown to be efficacious, and it may increase the risk of malignant transformation [12]. Medical treatment with bisphosphonates, however, has demonstrated varying results, with some papers reporting utility and others conferring treatment failure [12,13]. Lastly, denosumab is a monoclonal antibody targeting the RANK ligand that has shown to be promising for slowing tumor progression and pain [14] Further studies are required to determine utility in cases of optic nerve compression [15].
This patient suffered from recurrent craniofacial FD involving the medial and inferior orbital walls with extension into the orbit causing compressive optic neuropathy. Surgical resection of the mass was indicated, given the signs of visual compromise. While total surgical resection is considered the definitive treatment, a subtotal resection was performed in this patient due to the extent of the lesion. Radical resection would have required removal and reconstruction of the entire medial and inferior orbital walls with substantial removal and reconstruction of the midface. Using an endoscopic approach, however, we were able to avoid such an invasive and complex surgery and debulk most of the mass through the nasal cavity (Figure 2).
 Figure 2: Endonasal views of Medpore after orbital reconstruction.
View Figure 2
Figure 2: Endonasal views of Medpore after orbital reconstruction.
View Figure 2
Using an external approach, it is often difficult to protect the optic nerve due to poor visualization posterior to the globe. In the setting of bony resection, one must worry about mechanical and thermal damage from bone drilling. However, the combined endoscopic and external approach provided excellent visualization to the deep medial and posterior orbit, which allowed almost all the mass to be resected without optic nerve compromise. Additionally, orbital fat was noted to be prolapsed into the nasal cavity prior to the conclusion of the case via the endoscope. It was then re-positioned to avoid tethering of orbital tissue. If a traditional external approach had been singularly used, this would have been missed, and the patient likely would have suffered from restrictive strabismus, enophthalmos, and/or orbital volume deficit.
This technique offered a significant advantage with minimal risk and led to an excellent post-operative functional and aesthetic result. There has been no sign of radiographic recurrence at six months (Figure 3) or symptomatic recurrence at one year. Continued observation is essential for these patients to monitor for clinical recurrence. This study highlights advantages to improve surgical outcomes for patients with vision-threatening cases of FD via a time-sensitive and minimally invasive multimodal approach.
 Figure 3: Axial orbital CT scan 6 months after surgery.
View Figure 3
Figure 3: Axial orbital CT scan 6 months after surgery.
View Figure 3
The authors have no conflicts of interest to declare.
This study received no funding.