Background: What is the impact of the exponential increase in the car fleet in cities?
Aim: To describe the epidemiological, clinical, therapeutic and prognostic features of ocular trauma in Kara.
Materials and methods: We conducted a retrospective and descriptive study from January 1st, 2017, to December 31st, 2020, a period of 4 years. Mechanical traumas were classified according to the Birmingham Eye Trauma Terminology (BETT), and prognosis was assessed according to the Ocular Trauma Score (OTS).
Results: During the study period, 418 cases of ocular trauma were recorded, out of a total of 14652 consultations, corresponding to a frequency of 2.8%. The mean age was 28.5 ± 15.6 [1.92] years with a sex ratio of 2.22 (288M/130 F). In 5.5% of cases, patients consulted within 6 hours of trauma, and in 66.7% of cases, the delay of consultation time was more than 72 hours. The injury was bilateral in 11.5% of cases. Mechanical trauma accounted for 379 cases (90.7%), chemical burns 20 cases (4.8%) and thermal burns 19 cases (4.5%). Of the 379 cases of mechanical trauma, 342 cases (90.2%) were closed globe trauma, and 37 cases (9.8%) were open globe trauma. The circumstances of injury were domestic accidents with 115 cases (27.5%) followed by road accidents with 115 cases (25.1%), work accidents and brawls in equal proportion with 65 cases (15.6%), According to the OTS score, 345 cases (82.5%) had a score of 5, there were 35 cases (8.4%) with a score of 4, the score of 3 were found in 3 patients(6.2%) and the score of 2 and 1 were found in 6 patients each (1.4% ). Treatment was surgical in 8.9% of cases and medical in 91.1% of cases.
Conclusion: Ocular trauma is relatively common, better awareness will reduce consultation delays and improve prognosis. The best treatment remains prevention.
Ocular trauma, Open globe trauma, Closed globe trauma, Eye burn
Ocular trauma includes all aggressions of the eyeball or its appendages regardless of their origins. Aggression can be mechanical, chemical, physical or thermal. The eye accounts for only 0.27% of the total body surface and 4% of the facial surface, but it is the third organ most often affected by trauma after the hands and feet [1]. Worldwide, the annual incidence of eye trauma is about 55 million and eye damage accounts for 5 to 16% of ophthalmology consultations [2]. Eye trauma is a real public health problem because it is a preventable cause of morbidity and visual impairment [3]. Several studies carried out around the world and in Africa have highlighted the prevalence and severity of eye trauma. A frequency of 3.5% was noted in higher education institutions in south-eastern Nigeria [4], 3.56% in Yaoundé in Cameroon [5] and 3.4% in Ghana [6]. In Togo, according to a study carried out by Ayéna, et al. [7] in 2009, the frequency of eye trauma was 7.63%. Recent years have been marked by the increase in population and especially in the car fleet. Under these conditions, what are the characteristics of eye trauma in Kara? This study aims to describe the epidemiological, clinical and therapeutic characteristics of eye trauma in Kara.
We conducted a retrospective and descriptive study from January 1, 2017, to December 31, 2020, a period of 4 years. All patient records with eye trauma followed in the ophthalmology department of Regional Hospital Center Kara during the study period were included in this study. Mechanical trauma was classified according to the Birmingham Eye Trauma Terminology (BETT) [8], and the prognosis was assessed according to the Ocular Trauma Score (OTS) [9]. The parameters studied were age, sex, type of trauma according to the BETT, circumstances of trauma, consultation time, prognostic score according to OTS, treatment instituted. The parameters studied were analyzed with the SPSS 20 software. This study was carried out in accordance with the principles of ethics and professional conduct and in accordance with the Declaration of Helsinki.
During our study period, 4652 patients were consulted in the department, and 410 cases of trauma were recorded, which corresponds to a frequency of 8.81%. The average age of patients was 28.5 ± 15.49 [1-92] years. The age group of [21-30] years was the most represented with 134 patients or 32.7% (Figure 1). Students were the most represented with 97 cases (23.66%) (Table 1). There was a male predominance with a sex ratio of 2.25 (288H/130 F). The consultation time was specified in 166 patients (40.26%). The average consultation time was 50.17 ± 182.3 [1-1460] hours. According to the consultation time, 9 patients (5.4%) consulted within 6 hours of the trauma (Figure 2). The trauma was bilateral in 48 cases (11.7%). It involved only the left eye in 207 cases (50.5%) and the right eye in 155 cases (37.8%). The circumstances of the most frequent trauma were the domestic accident with 113 cases (27.6%) (Table 2). Mechanical trauma was found in 372 patients or 90.73%. The chemical burn was found in 20 cases or 4.88% and the thermal burn in 18 cases or 4.39%. According to the BETT classification (379 cases of mechanical trauma), 342 cases or 90.2% were closed globe trauma and 37 cases of open globe trauma or 9.8% of cases. According to the OTS score, 345 cases or 82.5% had a score of 5 (Figure 2). Medical treatment was instituted in 657 cases (94.53%) and surgical treatment in 38 cases (5.47%). For medical treatment, corticosteroids eye drops were the most widely used drug in 261 cases (63.7%) (Table 3).
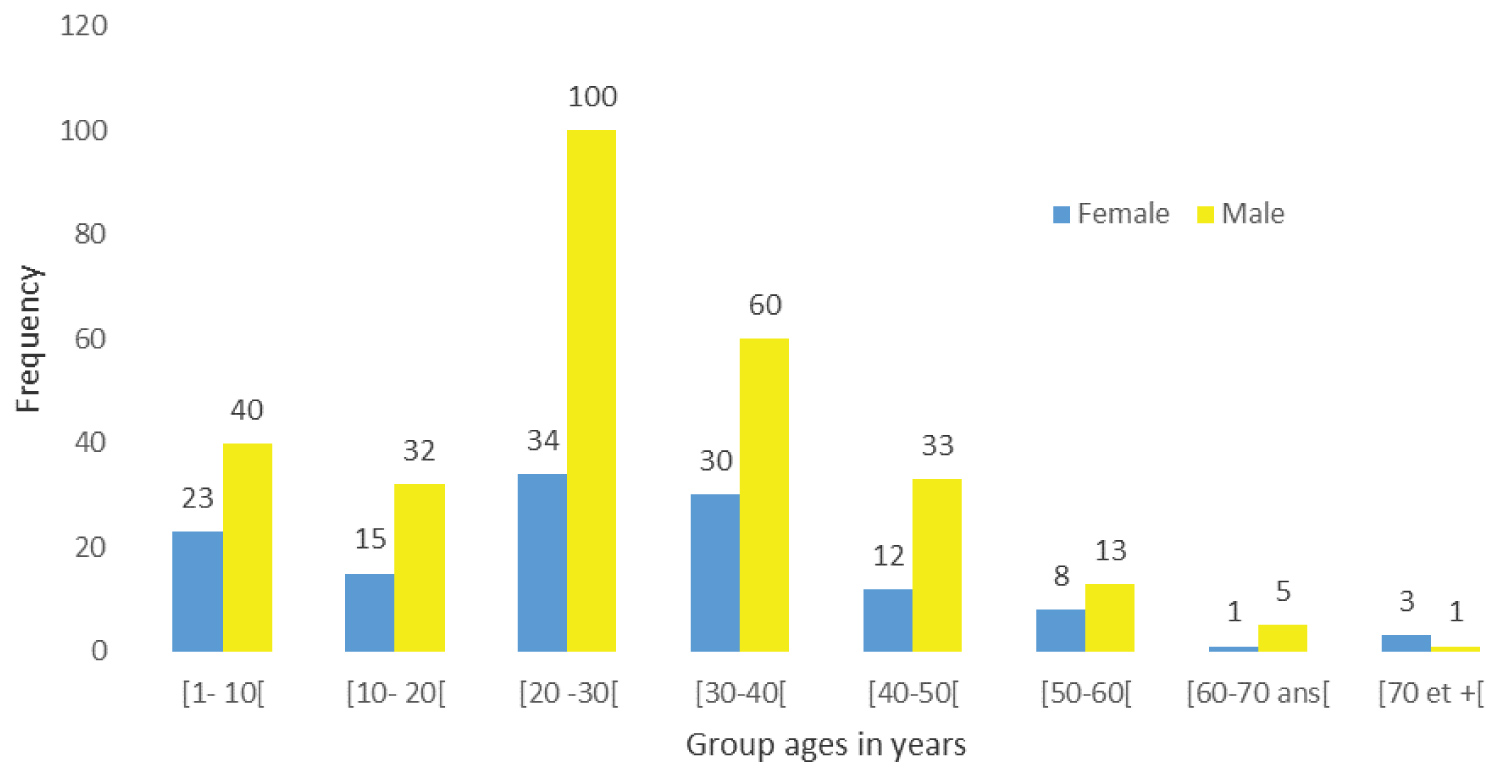 Figure 1: Patients' repartition according to group age and genre.
View Figure 1
Figure 1: Patients' repartition according to group age and genre.
View Figure 1
 Figure 2: Patients' repartition according to consultation delay.
View Figure 2
Figure 2: Patients' repartition according to consultation delay.
View Figure 2
Table 1: Patients' repartition according to occupation. View Table 1
Table 2: Patient's repartition according to trauma circumstances. View Table 2
Table 3: Patients' repartition according to medical treatment. View Table 3
In our study, the frequency of trauma was 8.81%. Our result is higher than the results of Ayéna, et al. [7] in 2009 in Togo and Koki, et al. [5] in 2015 in Cameroon in which had reported frequencies of 7.63% and 3.56% respectively. Our high frequency is probably due to an increase in the motorcycle fleet and non-compliance with the rules of the road. The average age of the patients was 28.5 ± 15.49 years, which is lower than the results of de Koki, et al. [5] who reported an average of 32.95 ± 16.15 years. These results are evidence that the youth population is the most affected and this could be explained by the fact that young people are more often engaged in traumatic risk activities. There was a male predominance with a sex ratio of 2.25. This predominance was found in most studies [10,11]. This increased prevalence among men is explained, according to the various authors, by the fact that men are more often engaged in activities at traumatic risk. In boys, it is explained by their turbulence and their tendency to violent sports and dangerous games. Added to this would be the fact that the traditional education of girls in Africa confines them at home to household chores while freer young boys engage in games. In our study, 12 patients (7.2%) consulted within 24 hours, and 124 patients (76.7%) consulted beyond 48 hours. For Yaya, et al. [12] only 2.0% of patients were seen before the 6th hour, compared to 43.7% between 48 hours and a week. This delay in consultation results in a delay in care with a reserved prognosis as a corollary. In our study the majority of injuries are those caused by domestic accidents (27.6%) followed by accidents on public roads (25.1%). On the other hand, for Okoye, et al. [13], the majority of trauma occurred in the field and at school during the games. The circumstances of the trauma vary from study to study and depend on the composition of the study population. Most of the trauma in our study occurred unilaterally and mostly in the left eye in 50.50% of cases. Unilateral impairment in eye trauma is recognized by several authors such as Kaya, et al. [14], Beby, et al. [15] and Skiker, et al. [16], on the other hand, the right or left laterality does not seem to have a consensus. According to the BETT, in our study, trauma was mostly closed globe (91.67%). Open-globe trauma testifies to the violence of trauma and is most often found in road accidents and assaults. Eyes classified as OTS 5 were the most numerous (84.39%) followed respectively by OTS 4 (15.61%), OTS 3 (9.51%), OTS 2 (2.93%) and OTS 1 (1.46%) which is similar to the results found by Koki, et al. [5]. The OTS Score is not popularized in our exercise conditions although it is an effective tool for emergency decision-making. Simple and single medical treatment was performed in 94.53% of our patients and surgical in 5.47%. The type of treatment depends on the type of trauma according to the BETT and the OTS score. Ayena, et al. [7] had similar results with 88% of medical treatment, while Traore, et al. [17] reported in 2002 a percentage of 31.9% of patients requiring surgical treatment. The limitations of our study are undoubtedly its retrospective nature. We are considering a cross-sectional study with the use of OTS which will allow us to compare the prognosis of eye trauma based on predictive results of OTS.
Eye trauma is relatively common in our environment, better awareness will reduce consultation delays and improve prognosis. The best treatment remains prevention which involves compliance with security measures and the Highway Code.
The authors do not declare any conflict of interest in relation to this manuscript.