Background: Data on uveitis is rare in Africa. This study aims to describe the epidemiological, clinical, and therapeutic characteristics of uveitis in Lomé (Togo).
Materials and methods: We carried out a retrospective and descriptive study based on patients' records between January 1, 2014, and December 31, 2018, a period of 5 years. The clinical, biological, and therapeutic characteristics of uveitis were analyzed. The Khi 2 test was used to compare percentages and Student's t-test to compare averages with a 5% threshold.
Results: Over 14200 patients' records, 203 cases of uveitis were included, giving a frequency of 1.4%. The mean age was 51.0 ± 16.2 years with a sex ratio of 0.78 (89M/114F). The uveitis was bilateral in 3 cases (1.5%). The average delay of consultation was 22.4 ± 30.1 days. Functional signs were visual blurring (50.7%), pain (34.0%), and redness (24.6%). Anterior uveitis accounted for 55.7%, intermediates for 5.4%, posterior for 19.7% and panuveitis for 19.2%. The etiology was found in 64 cases (31.5%) and is dominated by toxoplasmosis (23.7%). Topical corticosteroid therapy was combined to peribulbar corticosteroid therapy in 38.4% and oral corticosteroid therapy in 11.8%.
Conclusion: Uveitis in our practice is characterized by the delay of consultation and the low rate of etiology found. Further studies will focus on assessment of diagnostic and therapeutic protocols for the management of uveitis.
Uveitis- Delay of consultation, Toxoplasmosis, Corticosteroid therapy, Togo
Uveitis is an inflammation of the uvea: iris, ciliary body and choroid. Their annual incidence is 17 to 52/100,000 and their prevalence from 38 to 284/100,000 [1]. In Africa hospital frequencies vary between 1% and 1.35% [2,3]. The severity of uveitis comes from the functional prognosis that can be engaged and from the severity of the underlying general diseases. Although relatively rare, uveitis is responsible for 5% of legal blindness, often secondary to ocular hypertension, retinal ischemia or macular edema [4]. In developed countries, about a quarter of uveitis are linked to an ophthalmological disease, a quarter to proven systemic diseases, a quarter to systemic diseases, while the last quarter remains undetermined, called idiopathic uveitis [5]. In Africa, there is limited data on uveitis. In our conditions of practice, what are the particularities of uveitis in terms of diagnosis and therapeutic management? It is to answer these questions that we initiated this study with the aim of describing the clinical, biological and therapeutic characteristics of uveitis in Lomé.
We carried out a retrospective descriptive study on the records of patients followed in the Eye Clinic Afia in Lomé from January 1, 2014, to December 31, 2018, a period of 5 years. The sociodemographic, clinical, biological and therapeutic characteristics of uveitis were analysed. The data were analyzed by EpiInfo 7.2 software. The Khi 2 test was used to compare percentages and Student's t-test was used to compare averages with a significance threshold of 5%.
A total of 203 cases of uveitis were identified during the period out of a total of 14200 consultations, giving a hospital frequency of 1.4%. The average age was 51.0 ± 16.2 years with extremes of 17 and 97 years. The age group [37-47] years was the most common with 25.6% of cases (Figure 1). There was a female predominance with a sex ratio of 0.78 (89M/114F). The uveitis was bilateral in 3 cases (1.5%), in right eye in 111 cases (54.7%) and in left eye in 89 cases (43.8%). The average delay of consultation was 22.4 ± 30.1 days with extremes of 1 and 180 days. The functional signs found were visual blurring in 103 cases (50.7%), eye pain in 69 cases (34.0%), and eye redness in 50 cases (24.6%). Mean visual acuity was 0.37 ± 0.37. Blindness was noted in 52 cases (25.6%). The mean intraocular pressure was 17 ± 8 mmHg with the extremes of 8 and 60 mmHg. There was ocular hypertension in 46 cases (23.7%). Anterior uveitis accounted for 113 cases (55.7%), intermediate uveitis for 11 cases (5.4%), posterior uveitis for 40 cases (19.7%) and panuveitis for 39 cases (19.2%). Posterior uveitis was localized predominantly in the upper temporal in 16 cases (40%). Table 1 summarizes the clinical features. Complete blood count and Erythrocyte Sedimentation Rate (ESR) were performed in 62 cases each (30.5%). Leukocyte abnormality was noted in 15 cases (24.2%) and ESR was high in 27 cases (43.5%). Retroviral serology was performed in 38 cases (18.7%) with a positivity rate of 2.9% (6 cases). Toxoplasmosis serology was performed in 67 cases (33%) with a positive IgG of 74.6% (50 cases) and positive IgM of 4.5% (3 cases). The etiology was found in 64 cases (31.5%) and not found in 139 cases (68.5%). The etiologies were toxoplasmosis in 48 cases (23.7%), trauma in 11 cases (5.3%). Topical corticosteroid therapy has been the routine treatment in 100% of cases. It was combined with specific treatment in 52 cases (25.6%), peribulbar corticosteroid injection in 78 cases (38.4%) and oral corticosteroid therapy in 24 cases (11.8%). Table 2 summarizes the biological and therapeutic characteristics.
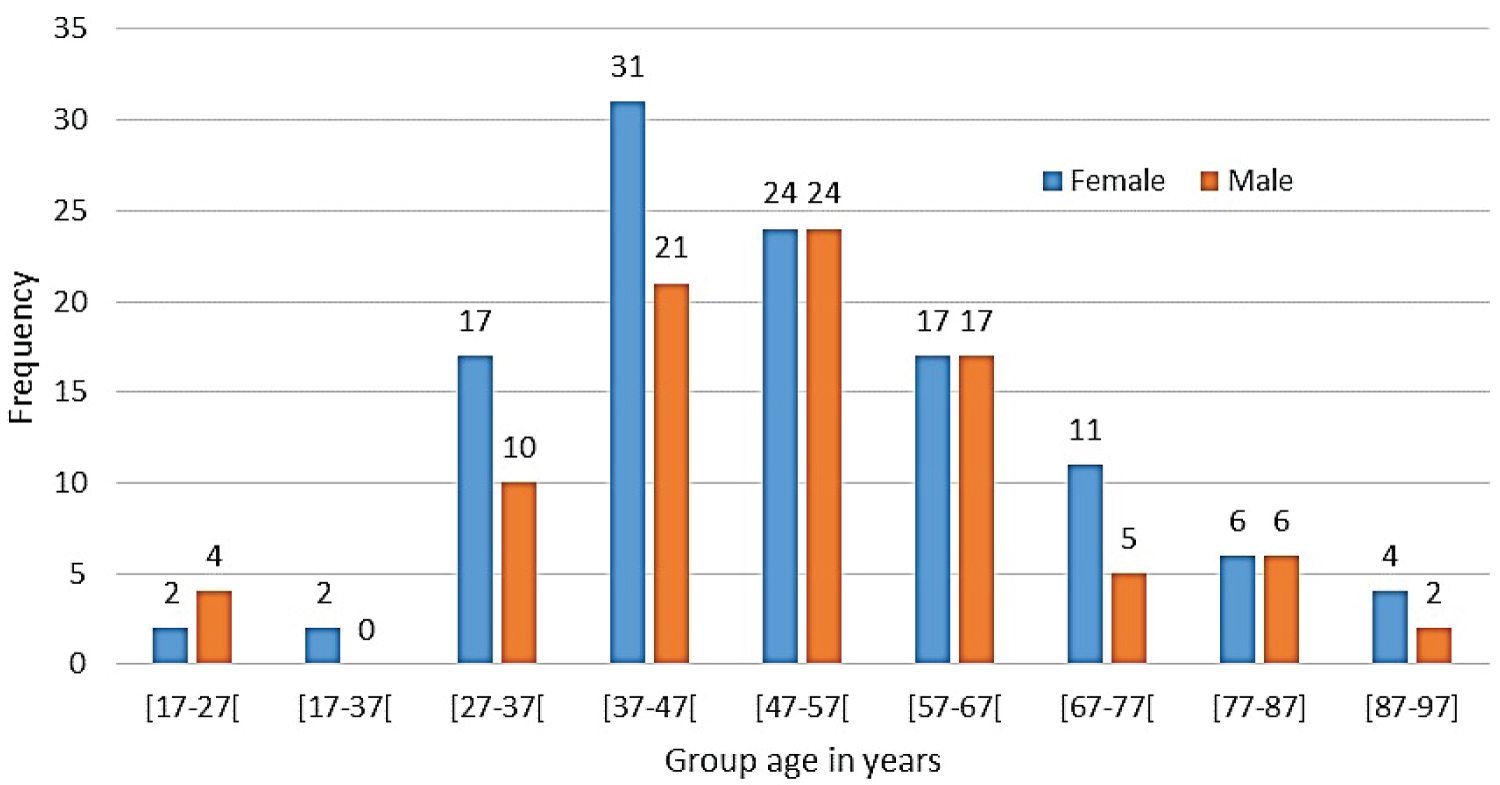 Figure 1: Patient's repartition according to group age and sex.
View Figure 1
Figure 1: Patient's repartition according to group age and sex.
View Figure 1
Table 1: Clinical features of uveitis patients. View Table 1
Table 2: Biological and therapeutics features. View Table 2
The frequency of uveitis in our study was 1.4%. The average age was 51.0 years with a sex ratio of 0.78. Bilateral uveitis accounted for 1.5%. The average consultation delay was 22 days, and the functional signs were visual blurring, pain and redness. Anterior uveitis accounted for 55.7%, intermediates 5.4%, posterior 19.7% and panuveitis 19.2%. The etiology was found in 64 cases (31.5%) of cases and is dominated by toxoplasmosis. Peribulbar corticosteroid therapy was performed in 38.4% of cases and oral corticosteroid therapy in 11.8% of cases.
The strength of this study is the use of minimum biological test to establish the etiology of uveitis. The lack of systematic investigation of general medicine is a weakness that needs to be rectified in further study.
The frequency of uveitis of 1.4% in our study is close to that of Assavédo, et al. [2], Ayéna, et al. [3] and Amédomé, et al. [6] which reported respectively 1.35%, 1%, and 1.02%. The female predominance of our series is in contradiction with the Assavedo, et al. [2], Ayéna, et al. [3] and Amédomé, et al. [6]. But female predominance has been reported in population studies, by García-Aparicio, et al. in Spain [7] and Xu, et al. in the USA [8]. The average age of 51.0 ± 16.2 years in our study is high compared to studies in the same region where the average age ranges from 35 to 40 years [2,3,6]. Mean age and gender predominance vary from one study to another and may be explained by bias in selection. The delay of consultation was 22.4 ± 30.1 days, Assavédo, et al. [2] also reported a delay of consultation of one week in 77.6% of patients. This delay of consultation contrasts with the proportion of 25.2% blindness noted in our study, because a decrease of vision should normally lead to a consultation without delay. This delay can be explained by the difficulties of access to ophthalmological care facilities. The triad blurred vision-eye pain – eye redness is found by most studies done in the same area [2,3,6]. Uveitis was bilateral 1.5% of cases in our study. Amédomé, et al. [6] reported 27% of bilateral uveitis, Ayéna, et al. [3] reported 27.4%. The proportion of bilateral uveitis can be related to the significance of systemic diseases.
Anterior uveitis is the most common (55.7%) followed by posterior uveitis (19.7%), panuveitis (19.2%) and intermediate uveitis (5.4%). The anatomic presentation of uveitis varies according to the target population. For the etiological diagnostic of uveitis, studies recommend an etiological assessment guided by ophthalmological semiology and therapeutic consequences [1]. According to the experts of the ULISSE group (Randomized Controlled Trial Evaluating a Standardized Strategy for Uveitis Etiologic Diagnosis) [9], a standard strategy with a minimum assessment (Complete Blood Count, Erythrocyte Sedimentation Rate, Protein Reactive C, Tuberculin Intradermal Reaction, Syphilis Serology and Chest X-ray) is more effective in etiological research. In our context, complete blood count, ESR, retroviral serology and toxoplasma serology were the minimum assessment. The positivity rate of toxoplasmic serology was 74.6% for IgG and 4.5% for IgM, which is consistent with the study of Wangara, et al. [10] for whom toxoplasmic IgM has an interest in the etiological research of uveitis with positive and negative predictive values of 0.64 and 0.41 for IgG and respectively 1.00 and 0.42 for IgM. The etiology of uveitis was not found in 68.5% of cases, toxoplasmosis accounted for 23.7%, and trauma 5.3%. Similarly, the etiology was not found by Assavédo, et al. [2] in 74.63% nor by Ayéna, et al. [3] in 85.7%. Toxoplasmosis was the etiology most found in 7.5% by Ayéna, et al. [3] and 11.9% by Assavédo, et al. [2]. The high rate of unknown etiology can be explained by the lack of general medicine investigation, and by minimum biological test. Topical corticosteroid therapy was combined with peribulbar corticosteroid injection in 38.4% and oral corticosteroid therapy in 11.8%. There are a growing number of molecules available to optimize the management of uveitis. The choice of systemic, periocular or intravitreal treatment depends on several factors: Chronicity or recurrence of uveitis, age, laterality, association with systemic disease, contraindications to molecules and socio-economic level. It is very important to find the best compromise allowing strict control of ocular inflammation with appropriate systemic and/or local treatment while avoiding complications [11].
A subsequent study with prospective collect with a validated diagnostic and therapeutic protocol adapted to our practice will provide global data on uveitis.
The retrospective aspect of this study, the lack of national consensus on the management of uveitis and the number of cases cannot allow generalization of our results.
This study demonstrates that uveitis, although relatively rare, is potentially blinding in our practice. Uveitis are characterized by a delay of consultation and a high proportion of etiology not found; toxoplasmosis has been the most frequent infectious origin. Further studies will focus on assessment of diagnostic and therapeutic protocols for the management of uveitis.
What is known on this subject: Uveitis is relatively rare. There is a delay of consultation in, and anatomic presentation is dominated by anterior uveitis.
What this study brings: The minimum biological assessment is useful for etiological research. Toxoplasmic serology with dosage of IgG and IgM is helpful. Peribulbar corticosteroids associated with eye drops corticosteroids is the main treatment.
The authors do not declare any conflict of interest in relation to this manuscript.
All authors contributed to the study design, data collection, statistical analysis, writing the article, and validating of the final manuscript.