Resin composite pre-heating is a recent innovative method that could be clinically beneficial by improving handling and marginal adaptation of the unset material paste.
The aim of this study was to gather all the laboratory trials regarding resin composite pre-heating and investigate how this technique affects the material.
An electronic search was carried out in PubMed and Google scholar databases, covering the period from January 2003 to May 2018. Specific criteria were set in order to define the relevance of each study.
Eighteen articles were included. The most commonly studied variable was the degree of conversion. Five studies found it increased and two not statistically significant different. Marginal adaptation, viscosity and polymerization shrinkage were higher. Flexural strength found to be unaffected. The results varied about microhardness and polymerization shrinkage.
Preheating has positive effect on the degree of conversion, viscosity, marginal adaptation and microhardness of composite resins. The flexural strength remains unaffected, the polymerization shrinkage is worsened, while the results for the microleakage are unclear. Further studies are need to take place in order to assess the clinical significance of composite pre-heating.
Composite resins, Composite pre-heating, Pre-heated composite resins
In the last decade, growing requests by patients for esthetic restorations have increased the use of direct resin composites in restorative dentistry [1]. However, drawbacks of composites like high viscosity and stickiness make them difficult for handling and manipulating, resulting in deficient marginal adaptation to preparation walls [2-4]. Flowable composite could minimize the gaps between the tooth and the restoration, due to their greater flow ability. However, their low filler content may cause higher net shrinkage, degrading the mechanical properties of restoration [5]. Another way to overcome this problem is to use a flowable liner in combination with regular composites. One recent alternative innovation is the use conventional composites that are pre-heated in a chairside warming device before polymerization [6-8].
Polymers can present lower viscosity when they are warmed. This is based on the theory that thermal energy forces the monomers or oligomers further apart, allowing them to slide by each other more readily [1,2]. Ideally, increased flow of pre-heated composite would improve adaptation of uncured resin to tooth walls and potentially reduce microleakage [9]. Recent literature shows advantages in increasing the flowability of composite resins by raising their temperature. Better handling improved marginal adaptation, higher degree of monomer conversion, better mechanical properties are some examples of the possible benefits of composite preheating, which made it a popular technique among clinicians [7,10].
The aim of this review is to collect the results of the laboratory trials which have studied resin composite pre-heating and find out the effects of this procedure in the material.
The review followed a process of locating articles through an electronic search in the PubMed and Google scholar databases. Searches were conducted covering the period from January 2003 to May 2018. The combination of the following terms was used to identify the relevant publications: "pre-heating of resin composites", "pre-heated resin composites".
The criteria for the final inclusion of each article were:
1) Laboratory studies that studied one or more variables related to the effects of pre-heating of resin composites prior to their placement in the cavity and their polymerization;
2) Sufficient data on the methodology of the laboratory experiments;
3) Articles written in English.
The exception criteria were:
1) Studies not related to the effects of pre-heating on resin composites;
2) Animal studies;
3) Articles related to the clinical handling of pre-warmed composite resins;
4) Studies with inadequate methodology data;
5) Articles written in languages other than English.
The relevance of each article was initially evaluated by scanning the title and then the summary. Articles found in all databases were reviewed for duplicate printouts that were automatically blocked.
The information selected from each object related to the effect of preheating of resin composite before its polymerization on the following variables: Degree of monomer conversion (DC), marginal adaptation (MA), flexural strength (FS), viscosity, microhardness (KHN), microleakage and polymerization shrinkage (PS).
A total of 167 articles were identified from the above electronic search. Due to the absence of duplicates, the same number remained for title and summary review. At this stage, 144 titles were excluded, and 23 abstracts were selected for reading, resulting in 23 full-text studies being evaluated for eligibility. The sample, following the inclusion and exclusion criteria, was ultimately formed at 18 articles (Figure 1).
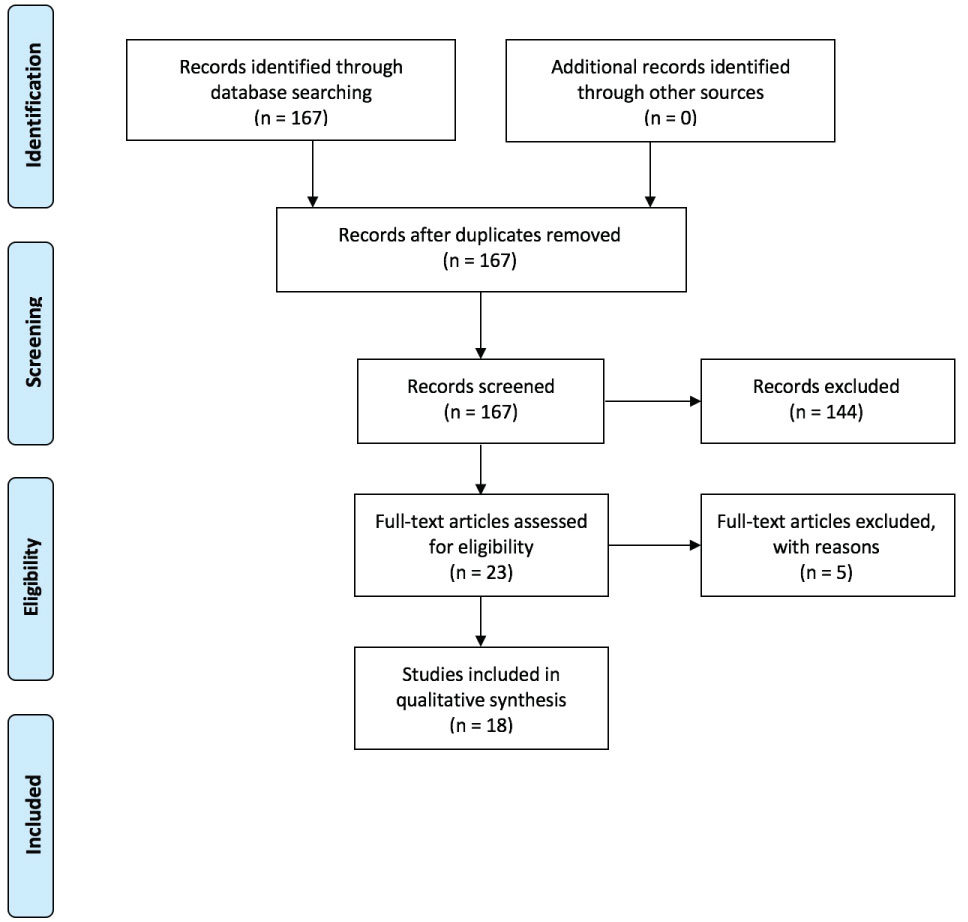 Figure 1: PRISMA 2009 flow diagram.
View Figure 1
Figure 1: PRISMA 2009 flow diagram.
View Figure 1
The laboratory tests and their results included in this study are presented in Table 1.
Table 1: Effect of pre-heating on studied variables. View Table 1
The most commonly studied variable, from seven research teams, was DC. Five of them concluded that pre-heating of resin composite led to an increase in DC while two contended that no statistically significant difference was found in the pre-heated resins. Regarding marginal adaptation, flexural strength and viscosity, the different research groups found unanimous results for each variable respectively. With pre-heating before polymerization MA was increased, FS was unaffected, and viscosity was increased. In contrast, for microhardness and microleakage the results of the laboratory tests vary. Especially, of the five laboratory tests that dealt with microhardness, three supported that the variable increased with preheating and two that it was not affected. Of those studied the microleakage, two showed that it was decreased but only under certain conditions (immediate polymerization and polymerization with a QTH lamp, respectively), one showed that it was unaffected and one that it was reduced. Finally, for polymerization shrinkage two studies concluded that it was increased while one that it was not statistically significant different after 24 h.
The degree of conversion is the rate of reacted C=C monomeric bonds, which are converted to C-C polymeric bonds. It expresses the extent of polymerization and is critical for the mechanical features, solubility, dimensional and color permanency and biocompatibility of resin composites [7,9,11]. A higher degree of conversion corresponds to increased microhardness, flexural strength and modulus, fracture resistance and tensile strength. However, polymers with similar conversion percentages may exhibit different cross-link density due to differences in the formation of their polymer network. Cross-link density is associated with amplified mechanical properties and stability. Thus, conversion alone is not enough for envisaging the performance of a resin composite [9,11]. Five laboratory tests showed that DC was increased after composite pre-heating. As the temperature rises, system viscosity is reduced, the mobility of the roots is boosted, and therefore additional polymerization and thus higher conversion is achieved. As the heating continues, the additional free volume increases, giving increased mobility to the trailing roots, resulting in increased collision frequency of the active species and further monomer conversion [9,10,12]. One study confirmed this higher DC on pre-heating temperature but pointed out that after 24 hours measurements the beneficial increase in DC is less distinguishing [7]. One study, on the other hand, concluded that composite pre-heating did not affect the DC. Τhe difference in this result could possibly attributed to the fact that the experiment took place under a non-isothermal condition. Furthermore, room-temperature composite can show an increase in DC up to 10% over time. This mechanism is unlikely to occur with pre-heated composites, since a higher conversion is reached immediately and so a further increase in the DC is dubious [13].
Of the three papers studying polymerization shrinkage, the two found higher shrinkage in pre-heated resins. This conclusion was expected, as it has been detected that polymerization shrinkage increases correspondingly with the degree of conversion [5,10]. However, one study showed no statistically important difference in shrinkage after 24 h [7]. Despite the highest shrinkage that appears to be present, it may not be clinically significant, as it can be offset by a better marginal adaptation [5]. Indeed, the laboratory results concluded that preheating of resins composites leads to better marginal adaptation and lowers the total gap area [2,13]. This could be explained by the reduced viscosity of pre-heated resins, as confirmed by the laboratory tests [5,14,15]. As the temperature rises, the flow capacity of the resin is improved, resulting in a better adaptability to the walls of a cavity [2]. This is an important finding, from a clinical point of view, since perfect sealing is crucial to expand restoration longevity [13].
It would be expected that the better marginal adaptation of pre-heated resins will be associated with a reduced microleakage. This is confirmed by one study [16]. Two studies resulted in the same conclusion, but only when polymerization occurs immediately after preheating [6] and only with the use of QTH lamp [17], respectively. The first limitation could be explained by the fact that delaying polymerization gives the time to the material to be removed from the walls due to viscoelastic behaviour [6]. The second one happens probably due to the fact that the QTH lamp offers lower polymerization energy, which creates less shrinkage in the resin used in the experiment [17]. The lesser microleakage is not confirmed by two studies [4,5]. This may be due to the non-isothermal conditions of the experiments, namely the abrupt drop in composite temperature during placing [4]. However, these studies have concluded no undesirable effect on microleakage. Thus, even if microleakage is not improved, it is at least not negatively affected [5].
Regarding the flexural strength of composite resins, studies have unanimously shown that it is not statistically significant different in pre-heated composites [3,5,13]. In contrast, the results of three laboratory tests showed that pre-heating led to an increase in microhardness [8,14,15]. Τhis could be explained from the higher rates of monomer conversion and the development of a highly crosslinked network. Contrary to these results, two studies have showed that temperature increase had no significant interference in microhardness values [11,18]. This effect can be attributed to the fillers of resins used in these studies. Lower filler loading of these materials may cannot give adequate support to the highly crosslinked network formed by pre-heating, in order to improve microhardness.
The above bibliographic review met two key constraints. Firstly, the literature extent was limited. The number of studies that have assessed this issue is small, which, due to the fact that each study dealt with a different combination of variables, resulted in fewer research data for each variable. Therefore, in order to evaluate the result of pre-heating for optimum clinical advantage, more trials should be done, which will provide the necessary data for the compilation of clinical studies and meta-analyzes [2]. Secondly, difficulties came up in comparing the results due to the different conditions under which each study was conducted. The heating temperature, the isothermal or non-isothermal conditions, the polymerization time, the specimen's thickness and the resin type were factors that varied between the studies. Some studies carried out their trials under isothermal situation, maintaining the material temperature constant, which does not correspond in clinical conditions. In the time since it is removed from the device until polymerized, heated composite cools quickly. It is expected that the material temperature reduces 50% after 2 min and 90% after 5 min. Consequently, the composite temperature when is photoactivated, is reduced to around 36 ℃ to 38 ℃. Thus, it is essential to estimate the effect of preheating in non-isothermal conditions, simulating the realistic clinical scenario [9,12,13,19]. In addition, the effect of preheating appears to vary from brand to brand and from shade to shade [8,9]. According to the above, in order to have more safely comparable results between surveys, in the future, laboratory tests should take place under similar conditions, using a larger variety of resin composites.
Within the limitations of this study, it is concluded that pre-heating of composite resins positively affects the degree of conversion, viscosity, marginal adaptation and microhardness. The flexural strength remains unaffected, the polymerization shrinkage is adversely affected, while the results for the microleakage are unclear. However, in order to assess the clinical significance of pre-heating, further studies with larger sample size and analogous experimental conditions are required.
This research received no external funding.
The author declares no conflicts of interest.