Background: Good level of oral hygiene practice (OHP) keeps the oral cavity clean and prevents most oral and systemic diseases, especially for children who live in low-income countries. This research aimed to evaluate middle school student's level of OHP and the association with socio-demographic characteristics in the capital city of Eritrea, Asmara.
Methods: A cross-sectional study was conducted to determine the level of OHP among 12-15 years old students in the selected Middle schools in Asmara. Data was collected from 572 study participants through structured interviews using a predetermined questionnaire. Pearson's chi-square test and multiple binary logistic regressions were used to analyze and infer the data.
Result: A total of 572 children with a mean age of 13 ± 0.9 years participated during the study. The majority of them had poor OHP 398 (69.6%). From the respondents, those who cleaned their tooth two times or more a day were 35.2%, dental floss was used as dental cleaning by a few (3.1%), and after meals tooth brushing practice by more than half of them (54.9%). The most utilized oral hygiene tools were a toothbrush (97%), chew-stick (71.9%), and toothpick (33.6%). Almost all children used toothpaste during tooth cleaning (97.4%), but majorities (89%) of them were unaware to fluoride on their toothpaste. From the participants, only one-third changed their brush every three months (34.4%), and approximately ten percent (12.6%) of them applied circular strokes while brushing their teeth. The most frequently consumed sugar foods and drinks were bread and biscuits, sugar-containing chewing gum, and tea cited as 93.7%, 54.8%, and 85%, respectively. About two-thirds (60.2%) of the respondents didn't clean their tongue and didn't visit a dentist at all. Level of Practice was significantly different only for gender and school name (P < 0.05). Female children had better OHP levels than males AOR = 0.636 (0.441-0.918, P = 0.012), and children in Arbate Asmara had better OHP than those in Bana AOR = 0.426 (0.197-0.92, P = 0.030). Hence, gender and the schools they attended had a significant statistical association with Oral Hygiene Practice (P < 0.05).
Conclusions: This study found that the majority of middle school children had poor OHP levels. Gender and school names had a significant correlation with practice. Development and implementation of Comprehensive preventive programs on Oral Hygiene Practice education for the children at school, health care, and community level are needed.
Oral hygiene practice, Middle school children, Low-income countries
OHP: Oral Hygiene Practice; OCMHS; Orotta College of Medicine and Health Sciences; MOH: Ministry of Health; MOE: Ministry of Education; WHO: World Health Organization; SPSS: Statistical Package for Social Sciences; M ± SD: Mean Plus/Minus Standard Deviation; LMICs: Low- and Middle-Income Countries; GNI: Gross National Income
Oral hygiene is the condition or practice of maintaining the tissues and structures of the mouth in a healthy state [1]. Maintaining good oral hygiene is considered to be a lifelong habit, and these oral habits are said to begin in an early stage of life [2]. Good oral hygiene is the foundation of a healthy mouth and prevents 80% of all dental problems [3].
Keeping the mouth clean prevent common oral health diseases, is necessary, especially in children who live in developing countries [4]. The quality of a child's oral hygiene practices and the parents' ability to withhold carcinogenic snacks are also factors associated with dental caries [2,5,6]. Socio-economic factors such as income, education level, and family size impacted oral disease prevalence [7-10].
The negative impact and burden of oral diseases restrict activities in schools and homes, leading to the loss of many potential working hours and more than 51 million school hours, respectively [2,11].
Oral health is defined as "a state of being free from chronic mouth and facial pain, oral and throat cancer, oral sores, congenital disabilities, gum disease, tooth decay, tooth loss, and other diseases that affect the oral care" [12].
Oral health is a very low priority in the African Region with extreme poverty; limited resources are available to the health sector services. The little assigned health sector is mainly directed towards life-threatening conditions such as HIV/AIDS, tuberculosis, and malaria rather than oral diseases [13].
Many oral health conditions can be detected early and are preventable with appropriate care. Oral health is an essential component of general health and well-being. But, this can be impeded by the cost, poor access and inequitable distribution of the dental workforce, undue fear, anxiety, self-blaming, low oral health literacy, beliefs, negative attitudes, and poor behaviors towards oral health [14].
Oral hygiene maintenance may be an ignored practice in people of the low socio-economic class of developing countries [15]. The majority (90%) of the students had experienced dental cavities and could lead to tooth loss at a very young age [16]. WHO recommended Oral health promotion through schools for improving knowledge, attitude, and behavior related to oral health prevention and control of oral health problems among school children [17]. Children and adolescents who develop good oral hygiene practices were more likely to maintain their health behaviors in adulthood. Similar studies have shown children in low- and middle-income countries (LMICs) may have limited access to some of the tools for practice in addition to lacking access to routine dental care [18,19].
Various environmental and lifestyle factors such as nutritional status, tobacco smoking, alcohol, poor oral hygiene, stress, and systemic conditions were linked to oral diseases [4]. Oral and dental hygiene is essential to good health in general and prevents many diseases [20]. Another study has identified that Dental caries and periodontal problems were due to poor oral hygiene practices [21]. Previous study findings indicated that the best way to avoid oral disease and tooth decay is to promote oral hygiene practices [22]. The development and implementation of preventive programs are necessary to introduce a healthy lifestyle and self-care oral practices, especially for the children of developing countries [16].
Although there is abundant literature on OHP, little is being known about practice among middle school children's in Eritrea in relation to their socio-demographic variables. In Eritrea, Dental caries was ranked as the highest disease in 2013, and 2014 and the second-highest reported illnesses during 2011, 2012, 2015, and 2016 respectively [23]. Dental caries is a more common public health problem among 12 years old in developing countries. There is a Gap in dental health service utilization, dental health practices, and suboptimal water fluoride levels that have contributed to poor dental health among school-age children in Eritrea [23].
This research will provide recommendations to organize oral hygiene education strategies to improve oral hygiene practices in the schools and communities of low-income countries. Therefore, this research presented key findings and recommendations regarding middle school children's level of OHP in low-income countries in Asmara, Eritrea.
A descriptive, cross-sectional was applied to assess the level of OHP and its association with socio-demographic characteristics among 572 middle school students in low-income countries in the capital city of Eritrea, Asmara. This study was carried out from February to June 2019 in the selected middle schools among 12 to 15 years old children. Asmara is more populated than other cities in Eritrea having the nine ethnicities from different regions. Children in urban areas have more access to sweat, food, and fluids than those in rural areas [23]. Furthermore, they identify many contributing factors to a high prevalence of dental caries [23]. Therefore, determining the pattern of their oral health practice can prevent most oral diseases and its complication even to their general health. The population of Eritrea is 3,497,117 as of 2019. Middle school (6th, 7th, and 8th) is a governmental academic institution that gives service since the independence, 1991, to 12-15 years old children. The total number of students targeted for this study in Asmara were 8336.
This study targets middle school students (6, 7, and 8th grades) from the age of 12-15 years old. After checking Inclusion and exclusion criteria, a multi-stage random sampling technique was used to recruit the study participants. First, the four administrative sub-zones were selected using simple random sampling from the thirteen zones of the central region Asmara, Eritrea. They were Arbate Asmara, Edaga Hamus, Tsetserat, and Godaif. Then, from the selected sub-zones, six schools were selected using proportionate to random sample size. These were Bahtimeskerem and Embatekera from Edaga Hamus sub-zone, whereas Bana and Gnbot 24 from Godaif, Arbate Asmara (within it), Hadnet from Arbate Asmara, and Tsetserat middle schools, respectively. Then, in the middle schools proportionate to the size, systematic random sampling was used to select the study participants from the three grades of each school.
The researchers collect the Data using a predetermined questioner by administering it through a face-to-face interview in the six randomly selected middle schools. At last only 572 (98.6%) questionnaires were found to be correctly filled and entered for data analysis in the SPSS.
The tool and its scoring system was adopted and modified by the researchers to suit the study design & setting from worldwide conducted studies, especially in developing countries [12,15,24-26]. First, a preliminary draft of the questioner was distributed to a panel of colleagues, dental therapists, and lecturers in OCMHS by providing the study's aim and objectives. After that, based on their comments and feedback, it was piloted if the tool could assess the level of OHP and its association with the socio-demographic characteristics. Finally, the researchers do appropriate modifications & corrections done according to their feedback, study objective, and setting.
Moreover, to reduce data entry errors, a Census and Survey Processing System (CSPro, Version 7.0) software package entry program used to automatically check the data structure using skip patterns and a range of valid values. Necessary modification was done after reviewing the reliability coefficient, validity, and normality of the study tool, for data collection for this study.
The Research tool has two parts that include socio-demographic and Oral Hygiene Practice questionnaires.
Socio-demographic information section: This section includes twelve items: The participant's school name, age, gender, grade, place of residence, ethnicity, family size, religion, father's & mother's occupational and educational status.
Oral hygiene practice section: The researchers used sixteen questions to measure the level of OHP and association with socio-demographic characteristics in middle school children. Each correct response was given one mark and zero score to an incorrect & none response question. The composite practice scores totalled from all sixteen questions, providing an ideal minimum and maximum score of 0 and 65, respectively. The Oral Hygiene Practice score was expressed in percentile form for better interpretation, believing as scores increase and practice also do.
Hence, the total score was calculated by adding all correctly answered items, with a maximum expected value of 65. Then, the obtained values were converted to 100 percent using SPSS version 22 (sum score × 100 divided by 65) to declare as having good or poor Oral Hygiene Practice with a minimum score of 50% (Figure 1) and (Table 1).
 Figure 1: Status of oral hygiene practice.
View Figure 1
Figure 1: Status of oral hygiene practice.
View Figure 1
Table 1: Level of OHP score difference with its socio-demographic variables (N = 572). View Table 1
Data analysis was carried out using both descriptive and inferential statistics with the help of Statistical Package for Social Sciences, version 22. After recording and entering the raw data, the researchers cleaned and checked the normality of the data to select an appropriate statistical analysis method. Descriptive statistics such as mean, frequency, and proportion were used to describe the data. Besides, inferential statistics like Pearson's chi-square test, & multiple binary logistic regression were also used to assess significance of difference and correlation between OHP and socio-demographic characteristics, respectively. The statistical significance was set at a 95% confidence interval and P-value < 0.05 level.
Level of Oral hygiene practices: This is an activity undertaken by the children to protect, promote, maintain oral health, or prevent dental diseases and bad breath.
Good oral hygiene practice: This is cleaning mouth, tooth, and tongue (oral cavity) using the proper tool, technique, and timing among middle school children, measured by the proportion of all questions responded correctly by the participants.
Good Oral Hygiene Practice = sum score of correct response × 100 divided by 65
Poor oral hygiene practice: This is either improper use of the tool, technique, or timing to maintain oral health among school children, measured by the proportion of questions responded incorrectly by the participants.
Poor Oral Hygiene Practice = sum score of incorrect response × 100 divided by 65
Associated factors: Are Socio-demographic variables that influence Oral Hygiene practices of middle school students by either facilitating or hindering them.
Middle school: An intermediate school (6th, 7th, and 8th) grades between an elementary and high school.
Student/s: A Child from 12 to 15 years old enrolled in formal academic middle schools.
Low-income countries: According to the World Bank, low-income countries have less than $1,026 per capita gross national income (GNI).
The face and content validity of the questionnaire was checked through reviewing the English and Tigrigna version by experts in the panel at the Department of Nursing and Dentistry in Orotta College of Medicine and Health Sciences. The research tool's construct validity was confirmed using a predetermined questionnaire from previous studies and WHO standardized children oral health assessment questioner for middle school students [12,15,24-26]. The study tool was tested for reliability by computing Cronbach's alpha (r = 0.726).
A pilot study was conducted in a different middle school, Fithi primary School, in Asmara, among 115 (10% of sample size) children to assess the feasibility of the study, validity, sensitivity, and understandability of the questionnaire used by researchers & participants.
A descriptive cross-sectional study was used to determine the level of OHP and its association with socio-demographic characteristics among middle school children in the central region of Eritrea. A total of 580 participants were enrolled in this study initially. But eight of them dropped due to different reasons. At the end, 98.6 % (n = 572) of middle school children's responses were used for data collection and analysis.
This research revealed around half of them were (52.4%) males and the remained were females with a mean age of 13 ± 0.9. The majority of the children's religion was Christian (94.2%), those who lived in the urban were 93.4%, and they had more than six members (62.2%. As to the parental occupational status, less than half of them (42.5%) reported that their Father's as being governmental employees, mothers as being housewives (62.8%), and their paternal &Mother's educational status as being primary level or below was 40.4% & 46.3%, respectively (Table 2).
Table 2: Socio-demographic characteristics of the children participated in the study (N = 572). View Table 2
Tooth frequency and cleaning tools used by the participants: Regarding the frequency of tooth cleaning, only 201 (35.2%) of the students washed their teeth two times or more a day, whereas less than one-fourth (22.4%) cleaned once a day (Figure 2). The most frequently used cleaning tools were a toothbrush and local Chew-stick utilized by 97% & 70% of participants, respectively (Figure 3). Only a few 2.8%, used dental floss for a dental cleaning once a day. The majority of the participants (97.4%) used toothpaste during tooth cleaning (Figure 3), but (89%) of them were unaware of the presence of fluoride in their toothpaste (Table 3). Out of the students who used toothpaste, only 164 (29.4%) applied toothpaste to a total length of the bristles. Regarding the frequency of changing toothbrushes, around one-third of the children, 197 (34.4), changed their brush every three months, while 202 (35.3) of them changed their toothbrushes when bristles got frayed up (Table 3).
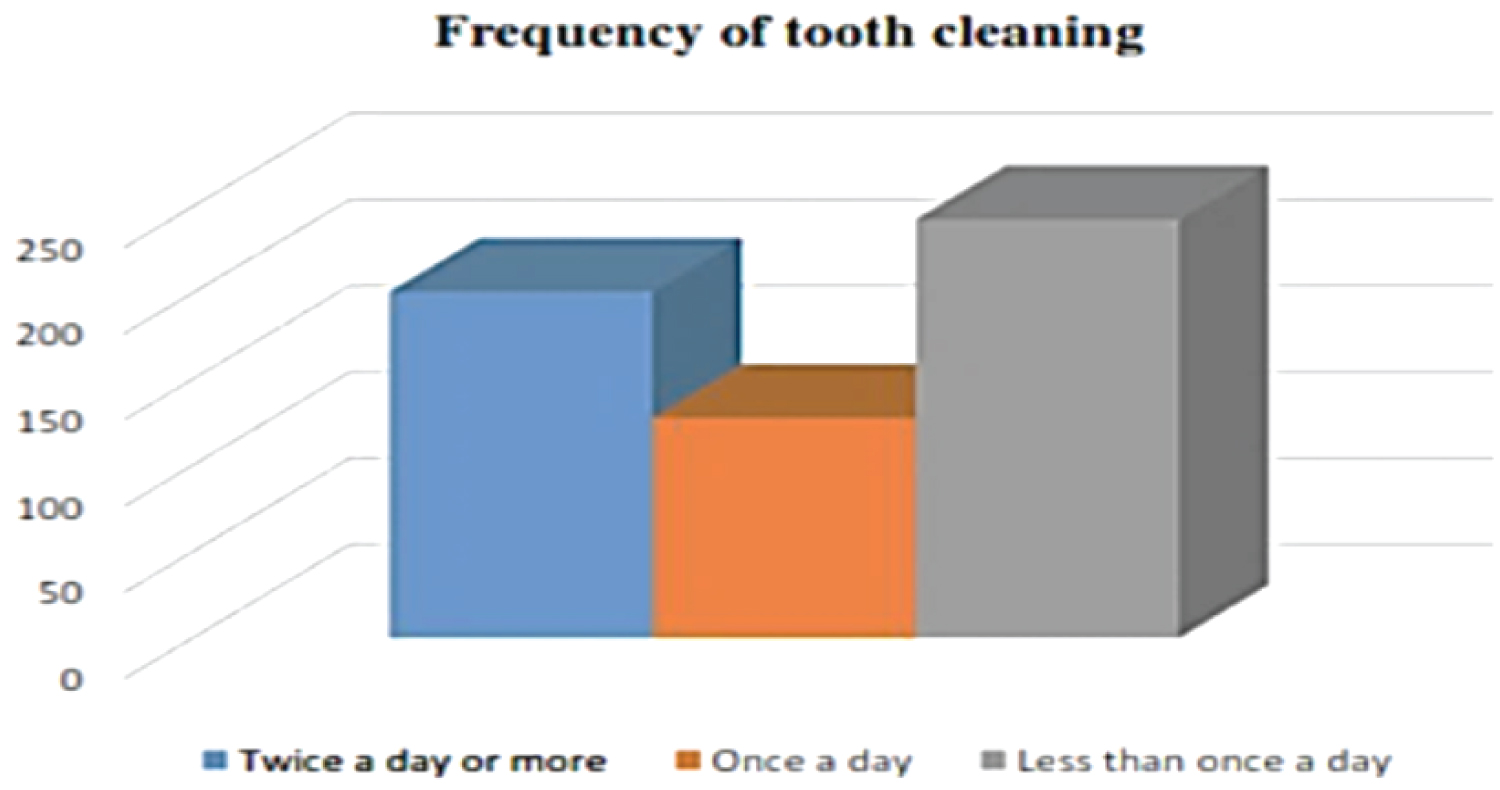 Figure 2: Frequency of tooth cleaning.
View Figure 2
Figure 2: Frequency of tooth cleaning.
View Figure 2
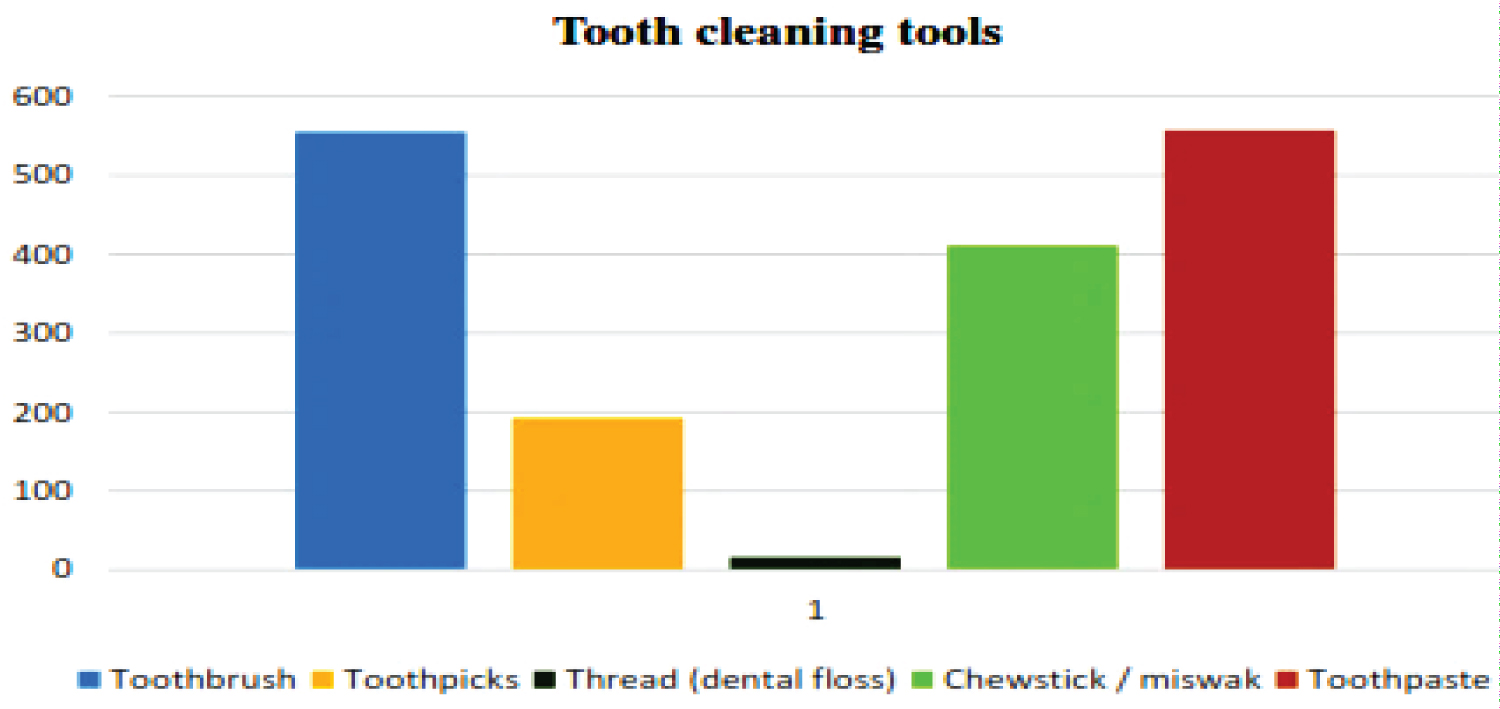 Figure 3: Tooth cleaning tools used by the participants.
View Figure 3
Figure 3: Tooth cleaning tools used by the participants.
View Figure 3
Table 3: Oral hygiene practice of middle school children (N = 572). View Table 3
More than half of the respondents (54.9%) brushed their teeth after meals, (15.7 %) brushed before meals, those who touched their teeth both before were (20.5%) & after meals. Two-third of the respondents (62.5%) brushed their teeth for the length of two or more minutes, for one or less than a minute was practiced by 28.2%, and those who were unaware about the time elapse to brush their teeth were 9.6% (Table 3).
Techniques of oral hygiene practice: In the current study, about half (50.9%) of the respondents applied both in horizontal and vertical directions, and more than a quarter used horizontal strokes (26.6%). A few of them applied circular strokes during brushing their teeth (12.6%). A similar proportion of the children, less than half of them, rinsed their mouth always and sometimes after each meal (Table 3).
Prevalence of tongue cleaning among participants: Almost half of the respondents (n = 280) cleaned their tongues using different tools (Figure 4). From the respondents, those who used proper tongue cleaner were only 9.3%, toothbrush (74.3%), fingers (10.3%), and other materials like salt and chew-stick were 8.9%.
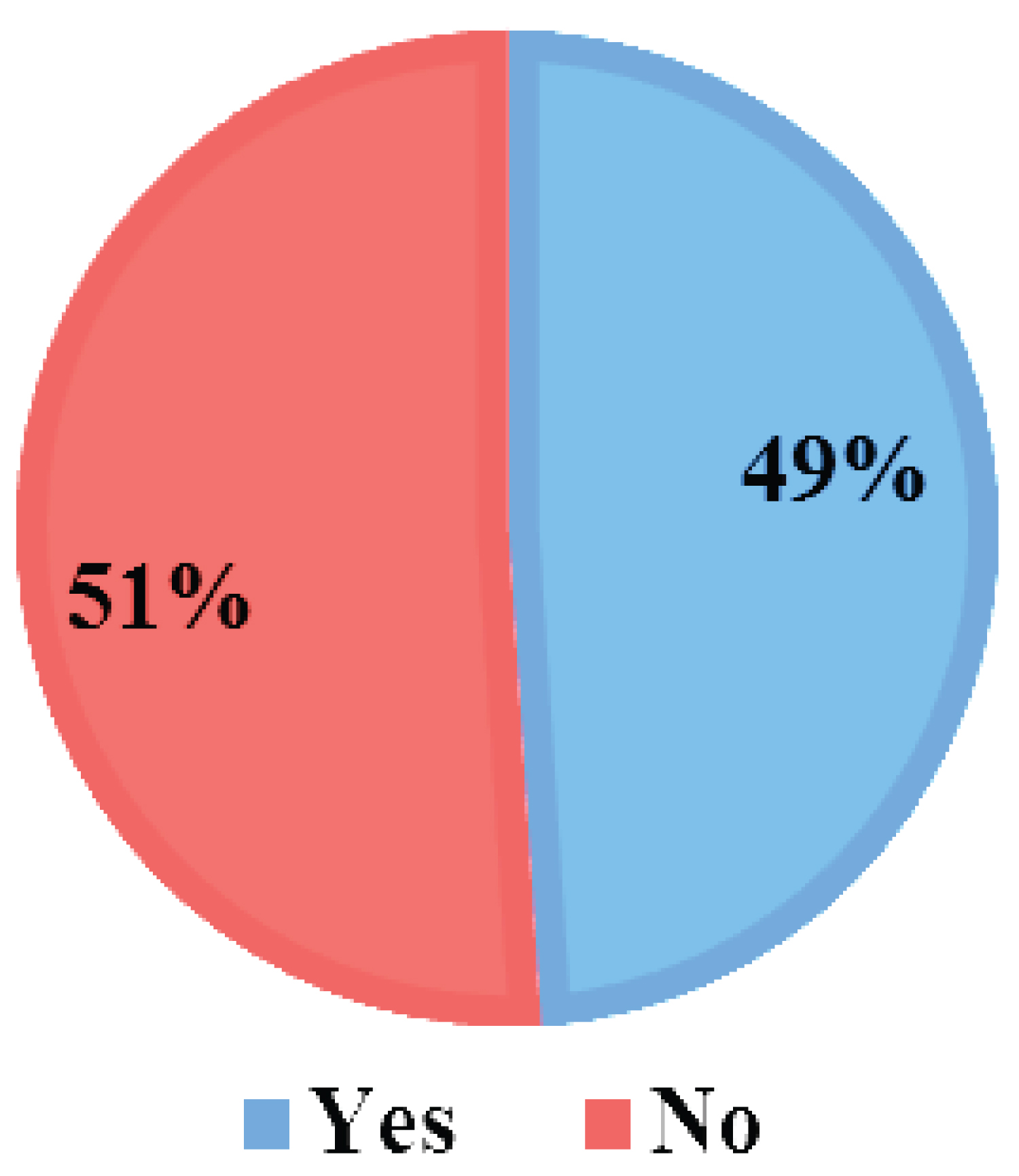 Figure 4: Prevalence of tongue cleaning among participants.
View Figure 4
Figure 4: Prevalence of tongue cleaning among participants.
View Figure 4
Frequency of consumed sugary foods and drinks: The practice of eating sugary food and drinks was another area that assessed. The most frequently consumed were bread and biscuits, sugar-containing chewing gum, and tea cited by (96.5%), (46%) and (89%) of respondents, respectively (Figure 5).
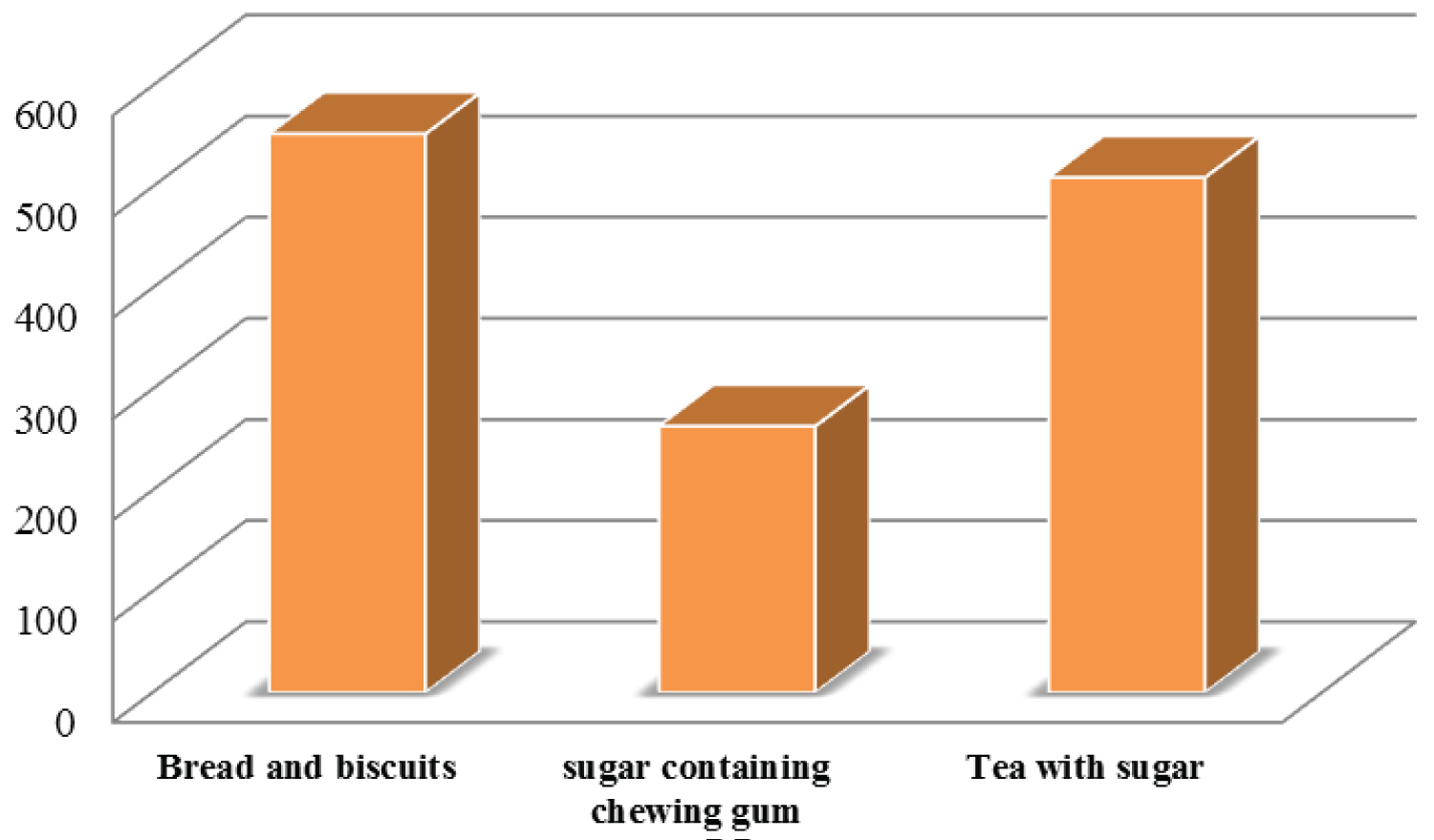 Figure 5: Frequency of consumed sugary foods and drinks.
View Figure 5
Figure 5: Frequency of consumed sugary foods and drinks.
View Figure 5
Frequency of dental visit of the participants: This study revealed that only 112 (19.5%) of the middle school children visited a dentist during the past twelve months; very few of them visited two times or more (8.5%) and saw once (11%). Besides, 114 (20%) didn't see a dentist in the past twelve months, whereas more than half (60.5%) never visited a dentist at all (Figure 6).
 Figure 6: Frequency of dental visit of the participants.
View Figure 6
Figure 6: Frequency of dental visit of the participants.
View Figure 6
Reason for a dental visit among participants: The reason for a dentist visit was due to pain or a problem with a tooth cited by a few of the total participants (17.8%) for treatment or follow-up 8%, and only one percent was for routine check-up of tooth or cleaning (Figure 7).
 Figure 7: Reason for dental visit among participants.
View Figure 7
Figure 7: Reason for dental visit among participants.
View Figure 7
Level of oral hygiene practice among middle school children: Overall, the practice of middle school children was poor. About two-thirds of them were found to have Poor Oral Hygiene practices (69.6%), and one-third had good practices (30.4%) (Figure 1).
Socio-demographic characteristics associated with oral hygiene practice: Levels of Oral Hygiene Practice scores, poor and good practice, were used to find the significance of difference to their socio-demographic variables. Both Gender (χ2 = 7.711, P = 0.005) and school name (χ2 = 14.578, P = 0.012) had a significant score of difference in OHP. Hence, Arbaete Asmara and Bahtimeskerem had better oral hygiene practices, whereas Hadnet and Bana had a higher proportion of children with poor Oral Hygiene practices than the other schools. However, there was no significant score difference in OHP among the other socio-demographic characteristics (P > 0.05) (Table 1).
Multivariate binary logistic regression: The result of multivariate binary logistic regression indicated a significant association between OHP and Gender, AOR = 0.636 (0.441-0.918, P = 0.016). Female children were 0.636 times more likely to have good OHP than males. In addition, there was a significant association between practice and the two schools, AOR = 0.426 (0.197-0.920, P = 0.012). Children from Bana middle school were 0.426 times more likely to have poor Oral Hygiene Practice than Arbate Asmara (Table 4). However, there was no significant association between OHP and the other socio-demographic characteristics (P > 0.05) (Table 4).
Table 4: Multiple binary logistic regression of computed variables (N = 572). View Table 4
Oral Hygiene Practice is an essential aspect of oral and general health to be discussed in middle school children, particularly in low-income countries. Children in developing or low-income countries are prone to oral health problems due to poor access to health, low resources, environmental factors, and activities like promotion, prevention, and maintenance. Oral Hygiene Practice may not be carried in middle school [16]. This cross-sectional study aimed at assessing the level of OHP in association with socio-demographic characteristics among middle school students in Asmara, Eritrea.
As other similar studies indicated, More than half of respondents in this study were males, and fewer than of them were females, similar to the finding of [27-29]. The mean age of the respondents was thirteen same as [28,30]. More than half of the participant's family size falls in the category of 5 to 7 members consistent [27]. About two-thirds of children reported their Mother's occupation was housewife lower than a study done in Harinavi, South 24 Parganas, West Bengal [31]. Less than half of them reported in this study as their Father's occupation was a Governmental employee.
Furthermore, Less than thirty percent reported that their Father's education was secondary level, and less than half of their Mother's education was secondary level. On the contrary, a study in West Bengal found higher parental educational level as a graduate or postgraduate [31].
The level of Oral Hygiene Practice among the respondents was assessed using different related questions adopted and modified accordingly. Most middle school children have demonstrated a poor practice of preventing, promoting, and maintaining oral health, similar to a study on oral hygiene among secondary school students in West Bengal [31]. Previous study findings indicated that the best way to avoid tooth decay and oral disease is to promote oral hygiene practices, including regular tooth brushing using fluoride, mouth rinse with fluoride, dental flossing, and dental visits. These practices were associated with a reduction in dental decay. Furthermore, compliance with practices enhances individual self-esteem, social acceptability among peers, and general health [22]. This study found that more than one-third of children cleaned their teeth two times a day or more, and less than one-fourth cleaned once a day indicates a low proportion of children were practicing oral hygiene. A study conducted in Qatar, 2016 showed the comparable practice of brushing teeth twice a daily [26], whereas more than half cleaned once daily higher than the current study. But, other studies found a higher proportion than this practice of brushing their tooth [22,28,29,32]. This variation could be due to the economic status and knowledge of the children and parents and dental service access for promotion, prevention, and maintenance of oral hygiene in a different setting.
A study was done on Oral hygiene practices in Rural-Urban Disparities among Primary School children in Lilongwe, Malawi. Found that most of them cleaned their tooth by brushing [33]; similar to this study. The most commonly utilized oral hygiene tools in the present study were toothbrushes and chew-stick followed by toothpicks and thread. Other studies in Nepal, 2014, and Iran, 2015 [32,34] found similar tools use, respectively. Moreover, a study conducted in India, 2012, [35] showed a similar proportion utilized dental floss and toothbrush with toothpaste, but a higher proportion used a toothpick. In a previous study done in Eritrea in 2017 among 12 years old school children, a similar proportion used local chew sticks. In contrast, a lower ratio than this finding used toothbrushes [23] implies it's improved.
Nevertheless, a study done in Nigeria reported lower utilization of chew stick as tooth cleaning means. Chew-stick is highly utilized in developing countries, including this study, due to low socio-economic status, easy accessibility, and frequent use by the children in the communities. The use of floss was negligible in this study, attributed to the lack of knowledge and practice regarding the importance and technique of flossing due to limited access to dental care services in Eritrea.
Most children in this study had a poor practice of changing toothbrushes every three months and around two-thirds changed when bristles frayed up congruent to study done in and south-eastern India [36]. On the contrary, a study carried out in 2019 in eastern India [31] revealed lower proportion changed their brush within three months. Another study done among primary school children in selected rural areas of Bangladesh in 2012 reported a high prevalence of poor oral hygiene depicted by the presence of plaque, calculus, caries, gingival bleeding in the study population [37]. Inadequate knowledge of the children & parents and socio-economic barriers could affect the interval of changing brushes.
The toothbrush with toothpaste was the most common oral hygiene aid used for cleaning the tooth. Many students brushed their teeth having toothpaste twice daily, higher than a study done in Malawi [33]. The majority of the respondents in this study used toothpaste during tooth cleaning. However, almost all of them were unaware of the presence of fluoride in their toothpaste. A study was done in Tamilnadu, south-eastern India, in 2016 found that a similar number of participants used toothpaste while brushing, but much higher than this study that used fluoride-containing toothpaste [36]. Similar studies on oral hygiene found many discrepancies in the use of tooth-cleaning compared to this study due to the limited knowledge and accessibility regarding fluoride use [23,25,30]. From the students who used toothpaste around, two-thirds applied toothpaste to a total length of the bristles less than the study done in Davangere [38]. Increased report of toothpaste utilization from this study was due to the annual provision of paste by the schools because the schools in Asmara provide toothpaste for each student yearly. After the completion, they were provided toothpaste by their parents.
Length of time during brushing is the skill children need to master during childhood through learning and practice. This study found that two-thirds of the study participants brushed their teeth for two minutes or more, consistent with a study done in Chandigarh, India [4]. However, a study done in Malaysia by Lian showed a higher result than this study [39]. In the present study, half of the respondents applied both horizontal and vertical strokes, whereas few applied circular strokes during tooth brushing. A similar number of children used the same technique for Appling toothbrushes, But a higher proportion of circular approach and combination of the other three methods was reported [30]. This practice gap was due to a lack of education and demonstration by parents and caregivers for middle school children. Less than half of the students always rinsed their mouths after each meal, inconsistent with these studies [27,29].
Furthermore, fifty percent of the respondents cleaned their tongues using a toothbrush. In contrast, only some of them utilized tongue cleaner as a recommended tool, lower than the study done by Vishwanathaiah S [38]. This poor practice of tongue cleaning could be due to the lack of awareness regarding the importance of oral hygiene. So, increasing children's understanding through oral education in schools or visiting the professional team could improve their tongue cleaning practice.
The most frequently consumed foods and drinks were bread and biscuits, followed by sweets and candy and soft drinks, as cited in this study. Studies were done in Iran, and Malaysia [4] reported different results than this finding. Children who live in urban areas like Asmara have more access to sweet foods such as bread and cakes and are frequently consumed as part of their regular diet. So, empowering children and parents with the knowledge of the carcinogenic effect of these foods and the importance of cleaning following each meal will reduce the risk of oral diseases. Getting better oral care access, especially for a dentist, is vital to improving OHP for children. This current study found that two-thirds had never visited a dentist during the past twelve months; different results were reported concerning visiting a dentist by [15,30,32]. Furthermore, [30] found that the reason for the visit was that toothache was lower and routine check-ups were higher than this study but very similar to a previous study done in Asmara, Eritrea, in 2017 [23]. This unsatisfactory utilization of dental visits could be due lack of accessible dental services, inadequate knowledge, or low economic status.
Integrating oral health education into the school curriculum can increase awareness among children and proper utilization by providing affordable and accessible services that could increase dental visits, improve oral hygiene practices, and reduce oral and systemic diseases [15].
This study cited gender and school, where the children studied, associated with OHP in low-income countries. Females had better Oral Hygiene Practice than males, similar to a study done in Iran that found females had practiced it more than males [34]. This finding may explain that females exhibit better health practices and attach more importance to their health as quantified by more frequent tooth cleaning [14].
Moreover, children from Arbate Asmara had better practice than Bana. The schools they attend could determine the practice level through the educational type, dental care aids supplying, and regular dental visits. How a female gender affects the practice better than males needs more further study.
At last, this study discovered that the other socio-demographic characteristics have no significant statistical association with the oral hygiene practice of middle school children (Table 4).
This research study has found a prevalent poor Oral Hygiene Practices among middle school children in low-income countries. Almost all children utilized toothbrushes and toothpaste during tooth cleaning, but with a wide gap of oral hygiene practice. Gender and the schools they were attending influenced their OHP. Hence, the development and implementation of Comprehensive preventive programs on Oral Hygiene Practice education for the children at school, health care, and community level are needed to promote, prevent and maintain oral health is imperative for middle school children.
Although this study provided essential information about middle school children OHP at the capital city of Eritrean, Asmara, it should be interpreted given the limitations of descriptive cross-sectional study. Besides, the data for this analysis was collected from middle school students in Asmara only, assuming their Practice would be low in urban than rural areas. Therefore, this result could not represent the practice of students out of the study setting, that might be even lower than this findings.
The finding of this study has an implication particularly to Child/Pediatric Nursing & Dental education, practice, researchers, and policymakers of low-income countries. Moreover, this study can be used as a baseline to launch further studies on children's oral hygiene education, practice, and management in Eritrea's educational sectors, hospitals, and other low-income countries.
Ethical clearance was granted from the Ethical Committee of Orotta College of Medicine and Health Sciences and MOH. Researchers acquired Permission by directing formal letters and thoroughly explaining the study objectives to school authorities. Confidentiality and anonymity were maintained, and written informed consent was obtained from participant's families or guardians, stating that the data would be used only for statistical purposes. The dignity of participants was maintained, and intrusive questions to the participants were avoided.
Datasets used to support this study are not publicly available because participant's ethical approval and consent prohibit sharing the raw data publicly. However, when deemed necessary, the corresponding author is available to discuss issues regarding data requests.
The authors declare that there is no conflict or competing of interest regarding the publication of this paper.
There was no special fund allocated for this study. The authors conducted the study as part of their employment in the ministry of health and the Orotta College of Medicine Health Sciences.
"T.O analyzed, interpreted the data, and prepared the manuscript regarding the OHP". AH, BM, BT, and LH performed the data collection, clearing, and entering SPSS. T.O was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
The authors wish to extend our appreciation to the Orotta College of Medicine and Health Sciences, Department of Nursing, Ministry of Health, and Education. Furthermore, our thanks go to Mrs. Paraksamma, who gives us constructive ideas for the research paper development. The authors also wish to thank the school authorities, the children, and parents for their kind participation.