Collagenous sprue, a rare and poorly understood disease of the small bowel is characterized by progressive weight loss, chronic diarrhoea and malabsorption. Due to its rarity, it is often misdiagnosed as celiac disease as it presents in similar manner. However, collagenous sprue unlike celiac disease is often refractory to gluten free diet and has poor prognosis. The key distinction between collagenous sprue and celiac disease lies in the biopsy of the small bowel where collagenous sprue shows prominent sub epithelial collagen deposition. As it has the potential to progressively deteriorate resulting in severe malnourishment, timely diagnosis through microscopic and macroscopic evaluation is crucial for early intervention. Herein, we present the diagnostic odyssey of an 89-year-old female patient who came in with a 6 months history of weight loss and chronic diarrhoea. She was eventually diagnosed with collagenous sprue, however she had passed away 2 months later following her initial diagnosis.
Collagenous Sprue (CS), an extremely rare disease affecting the small bowel with slightly over a hundred case reports published in the literature, was histologically characterized in 1970 [1,2]. CS affects more females than males (2:1), and most affected patients were middle age or elderly patients [3].
Clinically, this condition presents similarly to Celiac Disease (CD) with chronic diarrhoea, progressive mal absorption and weight loss [4], however CS is poorly responsive to a Gluten Free Diet (GFD), unlike CD [5]. Patients with CS may contain serological markers of CD such as anti-endomysial antibodies [6]. Furthermore, the histological result of both CD and CS may show intra-epithelial lymphocytosis and villous atrophy, making the distinction between CD and CS even more complicated. The key distinguishing factor between both entities is that CS has a prominent subepithelial collagen band with a thickness of more than 10 µm, and entrapment of the dilated capillaries [7]. Given the similarities and differences between CS and CD, the relationship between both has been controversial [5].
Prognosis of patients for CS remains relatively poor with high morbidity and mortality. Many suffer from relentless malabsorption, diarrhea and weight loss which ultimately lead to a fatal outcome [5]. Unfortunately, the aetiology of this condition has not yet been well understood given its rarity. From the existing literature, CS is most associated with CD where 50% of the cases occurred in CD patients, CS can also be associated with other co-existing autoimmune conditions [8]. Interestingly, there have been reports of pharmacologically induced CS associated with non-steroidal anti-inflammatory drugs and angiotensin receptor blockers use, in which cessation of these drugs have resulted in clinical improvement and histological resolution of the villous atrophy and collagenous subepithelial bands [9-11].
Currently, long term - high dose corticosteroids is the mainstay treatment for CS however it comes with deleterious side effects. Other options for CS include immunotherapy and nutritional support which is used in refractory celiac disease [12]. The efficacy of these have yet to be verified through clinical trials, but there have been successful cases of remission reported with the use of these agents [13,14]. The mechanism behind CS has been poorly understood which accounts for the lack of effective treatment options for this condition. More studies are required to elucidate the aetiology and treatment strategies for CS.
This case report describes a 89-year-old female who was brought in by ambulance with a 3 day history of lower abdominal pain associated with worsening diarrhoea and anorexia for the last 2 weeks associated with 8 kg weight loss over the last 6 months. This occurred on the background of known diverticular disease, Grave’s disease, ischemic heart disease, hypertension and osteoarthritis. She was on various medications for her co-morbidities: Olmesartan, paracetamol, aspirin and metoprolol, however, there has not been any recent changes to her medications. On physical examination, she was febrile to 38.5 Degrees Celsius, however remained haemodynamically stable. She had loss of skin turgor with dry mucous membrane secondary to her hypovolemic state. There was tenderness in the left iliac fossa with local guarding and no rebound tenderness. CT abdomen and pelvis showed evidence of mild diverticulitis and she was subsequently treated with gentamicin/ampicillin/metronidazole.
Computed Tomography (CT) of the abdomen and pelvis was ordered which reported colonic wall thickening and pericolic inflammatory change suggestive of acute diverticulitis involving the mid sigmoid colon. The small bowel and large bowel were of normal calibre. The surgical team reviewed the findings and commented that there was gas filled small bowel loops and diffuse thickening of sigmoid colon which was in keeping with colitis/enteritis. Laboratory results revealed raised inflammatory markers with faecal calprotectin (2190 ug/g), CRP (97 mg/L), however blood cultures, polymerase chain reaction of stools, and stool cultures were negative. She had severe electrolyte derangement requiring IV replacement, indicating ongoing gastrointestinal loss of fluids and her micro-nutrient screen including iron (2.6 umol/L), transferrin (1.2 g/L), albumin (18 g/L), vitamin A (0.4 umol/L) levels were low suggestive of mal absorptive disorder.
Following her discharge, she represented 4 days later with ongoing diarrhoea, poor oral intake and weight loss. There were no other infective symptoms. She appeared cachetic and dehydrated with dry oral mucosa. Infective screen of patient’s plasma was done to investigate her diarrhoeal illness which revealed presence of low CMV viral load (170 copies/mL) using polymerase chain reaction. She had raised creatinine of 140 umol/L suggesting acute kidney injury in keeping with her hypovolemia. She was given intravenous fluid replacement, and anti-viral (valaciclovir) initially to cover for possible CMV colitis. An urgent gastroscopy/colonoscopy was ordered to investigate her unintentional weight loss with biopsy taken from the stomach, duodenum, ileum and colon.
Initial endoscopic appearance of oesophagus and stomach was normal, while duodenum has mucosa that appeared flat, raising the possibility of coeliac disease. Patient was therefore presumptively treated as coeliac disease and was commenced on high energy and protein gluten free diet, resulting in mild improvement in her diarrhoea, however her oral intake and weight remained poor. Coeliac screen was carried out which was negative for coeliac markers (gliadin igG deaminated antibodies, transglutaminase igA antibodies immunoglobulin). She was subsequently discharged after her renal function has improved and follow ups were arranged with the community dietician, general practitioner and the gastroenterologist to review the biopsy and for repeat endoscopy following period of gluten free diet. Endoscopic features were relatively unremarkable (Figure 1a), while biopsy of the duodenum revealed sub epithelial collagen deposition typical of collagenous sprue (Figure 1b). The rest of the biopsy result from the stomach, terminal ileum and colon appeared within normal limits. Given that GFD was relieving her diarrhoea frequency from 6-10 times to twice per night, she was encouraged to continue with the diet. She was subsequently commenced on dexamethasone 4 mg daily as part of the treatment for CS. Despite treatment with corticosteroid and GFD, patient continued to lose weight with ongoing diarrhoea and was subsequently referred to the palliative care service. She passed away 2 months following her initial presentation to the emergency department.
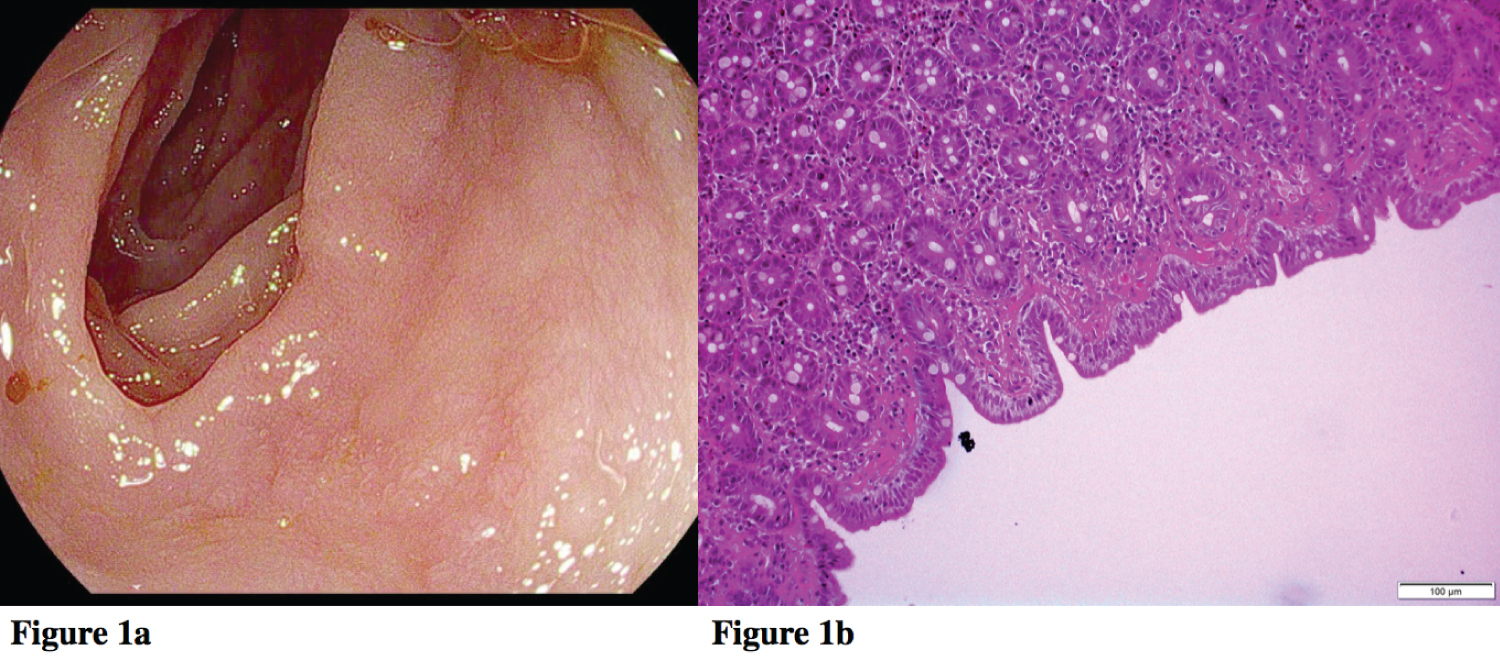 Figure 1: Esophagogastroduodenoscopy results of patient: 1a) Image of duodenum; 1b) Duodenal biopsy of the patient with band of subepithelial collagen deposition, subtotal villous atrophy with crypt hyperplasia and focal patchy increased intra-epithelial lymphocytes on Van Gieson’s staining.
View Figure 1
Figure 1: Esophagogastroduodenoscopy results of patient: 1a) Image of duodenum; 1b) Duodenal biopsy of the patient with band of subepithelial collagen deposition, subtotal villous atrophy with crypt hyperplasia and focal patchy increased intra-epithelial lymphocytes on Van Gieson’s staining.
View Figure 1
While Collagenous sprue was formally characterized in 1970, unfortunately little is known regarding the pathogenesis of the disease given its rarity [1,2], which impedes the formulation of a gold standard treatment plan. Clinically, CS is characterized by chronic diarrhea, mal absorption and weight loss. The current treatment for CS includes GFD, corticosteroid, immunomodulators and the suspension of relevant drugs [12,15]. Efficacy of these treatment options in achieving remission of CS has been variable. Initial case reports reported dismal outcome, despite strict GFD and/or corticosteroid administration [1,16], which is similar to the case we report.
On the other hand, Xiao, et al . reported having no response to GFD, but a successful outcome in terms of ameliorating gastrointestinal symptoms and resolution of collagenous deposit with the following treatment regimen: High dose prednisolone that was tapered down, with the subsequent addition of 5 amino-salicyclic acid and budesonide along with parenteral nutrition [12]. While, Jimbo, et al. reported having a successful outcome in a 3-month-old infant with CS after 3 months of prednisolone, 6-mercaptopurine and parenteral nutrition [17]. Thereafter, prednisolone and parenteral nutrition was stopped while mercaptopurine was continued for subsequent 9 months, and the patient was able to tolerate normal diet with adequate weight gain. Others have shown success in treating CS with immune modulators such as cyclosporine and thioguanine [13,14]. Interestingly, there is a strong association between use of Angiotensin receptor blockers (ARB) and CS. Cessation of ARB could potentially reverse the outcome of the condition [11]. Unfortunately, Olmesartan was not stopped for this patient as the working diagnosis was CD, and while awaiting for the biopsy results, the patient has already had significant cachexia with 13 kg weight loss over the last 6 months.
In conclusion, as CS presents similarly to CD with mal absorption, diarrhoea and weight loss, there is often a delay in diagnosis for CS given its rarity. Nonetheless, the two disease entities can be distinguished based on duodenal biopsy where CS would have prominent sub epithelial collagen deposition [7]. It is important to consider CS early in patients who are poorly responsive to gluten free diet as early intervention is crucial. CS has a rapidly fatal outcome with progressive mal absorption and weight loss such as that seen in this case report and previous literature. While no gold standard treatment has been established thus far, early immune modulatory therapy seems to be the most commonly used therapy based on the limited successful cases that have been reported [8,13,14].
Whilst speaking patient’s husband 3 months following the patient’s passing, it is still difficult for him to accept the diagnosis that the medical profession had made. Understandably so, as CS is a rare occurrence with only hundred over case reports published around the world, giving it a prevalence of < 0.0001%. In his perspective regarding his wife’s management, the medical community had failed in making an accurate diagnosis, and labelled it as CS which is currently a poorly understood disease with dismal outcome to begin with. This perhaps highlights the need for better psychosocial support and provision of information to patients and their next of kin in dealing with the diagnosis of an extremely rare condition.
There are various take home messages in this case. Firstly, CS should be recognized as a separate entity from CD given that its management and outcomes are vastly different, with CS being responsive to immunosuppressant, and CD being responsive to GFD. Hence it should be a differential diagnosis to consider when a patient comes in with weight loss, mal absorption and chronic diarrhoea. Secondly, as CS has a rapidly progressive course, where this patient suffered from 8 months of weight loss and mal absorption, out of which she had severe diarrhoea in her last 2 months, this necessitates urgent biopsy to differentiate between CD and CS, so that appropriate treatment could be trialled and hopefully alter the outcome.
Thirdly, medications should be reviewed, given that certain medication such as Olmesartan might be a reversible cause for the progression of CS. Thirdly, this case highlights the diagnostic challenges a patient with rare disease experience, with frequent representations to the hospital and being offered different diagnosis by various specialists. Better psychosocial support should be provided for the carer and their next of kin throughout this difficult journey which few understands.
Nan Fang Wang and Nam Gu Kang are the authors for the case report, and contributed to the writing of the manuscript. The corresponding author confirms that all listed authors have met the authorship criteria, and no others who have contributed were omitted.
Both authors have completed the ICMJE form and declared that there was no support from any external authorities or financial relationships/interest involved in the submission of this manuscript.