Castleman disease (CD) is a rare lymphoproliferative disorder, originally described by Dr. Benjamin Castleman, characterized predominantly by enlarged mediastinal lymph nodes with unknown etiology. While it commonly affects mediastinal lymph nodes, occurrences in neck lymph nodes are less frequent, and presentation in the extremities is exceptionally rare. This report presents a case of a 55-year-old female with a 15-year history of a solitary swelling in her right arm. The swelling was initially painful but later the pain subsided gradually. Fine Needle Aspiration Cytology (FNAC) of the swelling showed a haemorrhagic background with singly scattered small mature lymphocytes, occasional transforming lymphocytes, and sinus histiocytes, leading to an initial suspicion of lymph nodal enlargement. A subsequent biopsy and Histopathological Examination suggested the possibility of Castleman disease of the hyaline vascular type. This case highlights the diagnostic challenges in atypical presentations of CD, especially in rare locations such as the extremities, and underscores the importance of including CD in differential diagnoses for persistent limb swellings.
Extranodal castleman disease, Hyaline vascular type, HVCD
Castleman Disease (CD) was first described by Dr. Benjamin Castleman in 1950 as a localized enlargement of the mediastinal lymph nodes. Characterized by an increase in lymphoid follicles, germinal center involution, and marked capillary proliferation with follicular and interfollicular endothelial hyperplasia, CD's pathology was further elaborated by Flendrig in 1969, who identified three histopathological variants: The Hyalinized type, Plasma cell type, and Mixed type [1-3]. In the mid-1980s, CD was clinically divided into Unicentric CD, affecting a single lymph node or a single region of lymph nodes, and Multicentric CD, involving multiple lymph node stations [4]. Notably, some reports have identified an association between Human Immunodeficiency Virus (HIV) and Multicentric Castleman Disease [5]. This manuscript presents a case of Hyaline Vascular Castleman Disease (HVCD) manifesting as a solitary subcutaneous mass in the right arm, highlighting an atypical presentation of CD and contributing to the broader clinical understanding of this disease.
A 55-year-old female presented to the surgery outpatient department (OPD) in December 2021 with a solitary swelling in her right arm. The patient was referred from the surgery OPD to the cytopathological section of the Department of Pathology, Government General Hospital Nizamabad, for fine needle aspiration cytology (FNAC). The patient's medical history indicated the presence of the swelling for 15 years, initially small in size and gradually enlarging to its current dimensions of 3 cm × 3 cm. Initially painful, the discomfort associated with the swelling diminished over time. Physical examination revealed a mobile swelling, soft to firm in consistency, with normal overlying skin (Figure 1A). No other subcutaneous swellings or lymphadenopathy were noted.
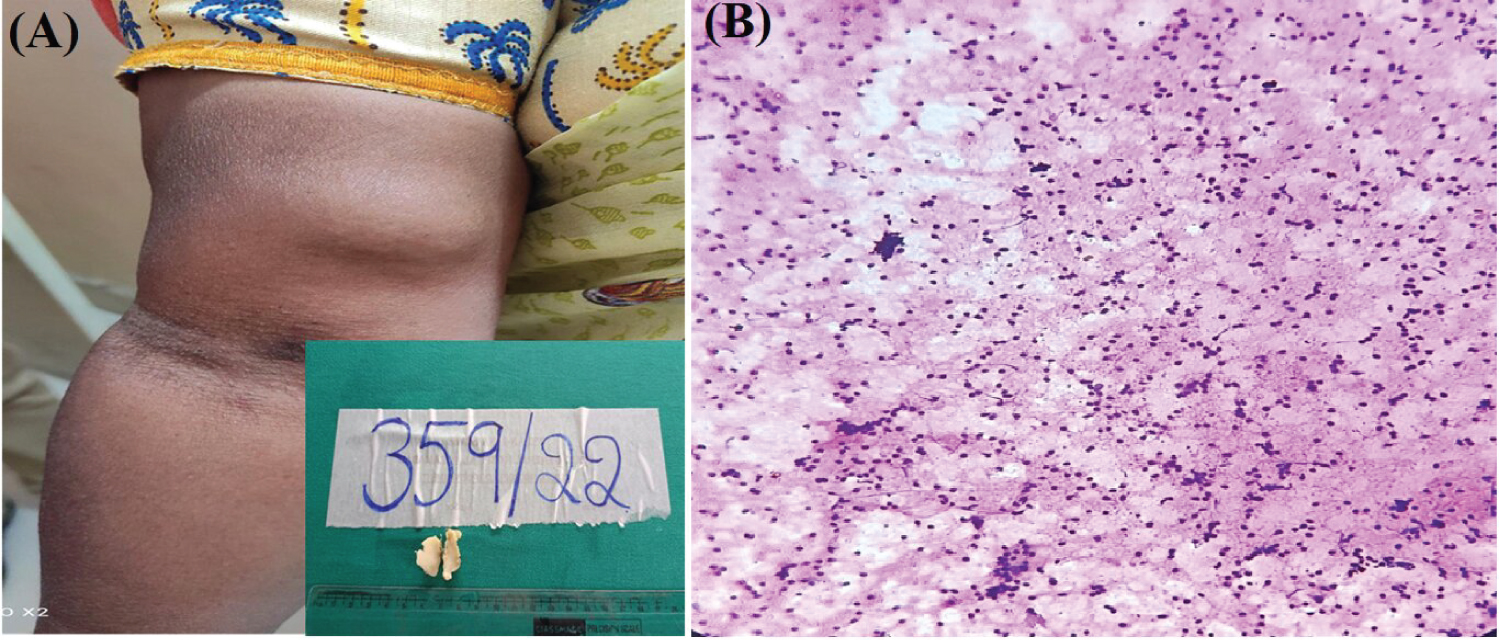 Figure 1: (A) Swelling over flexor aspect of right arm m/s 3 × 3 cms. Inset shows soft tissue mass measuring 2 × 1.5 × 0.5 cm. cut section homogenous grey white; (B) Cytosmear shows polymorphous population of mature lymphocytes, transforming lymphocytes and sinus histiocytes against hemorrhagic background.
View Figure 1
Figure 1: (A) Swelling over flexor aspect of right arm m/s 3 × 3 cms. Inset shows soft tissue mass measuring 2 × 1.5 × 0.5 cm. cut section homogenous grey white; (B) Cytosmear shows polymorphous population of mature lymphocytes, transforming lymphocytes and sinus histiocytes against hemorrhagic background.
View Figure 1
FNAC results showed a blood-mixed aspirate. Cytosmears indicated singly scattered small mature lymphocytes, occasional transforming lymphocytes, and sinus histiocytes against a hemorrhagic background, suggesting reactive hyperplasia of the lymph node (Figure 1B). An excisional biopsy was subsequently performed, and the specimen, a single grey-brown globular soft tissue mass measuring 2.6 × 0.8 × 0.6 cm, was sent for histopathological examination. The cut section of the specimen displayed homogeneous grey-white areas (Figure 1A Inset).
Microscopic examination revealed a well-circumscribed tumoral lymphoid tissue composed of lymphoid follicles - both primary and secondary, with germinal centres in a few and prominent hyalinised blood vessels. Germinal centres exhibited prominent mantle zones comprising small mature lymphocytes, while interfollicular areas contained mature lymphocytes, plasma cells, histiocytes, and numerous hyalinised blood vessels. Notably, onion skin rimming of lymphocytes in the mantle zone was observed (Figure 2A, Figure 2B, Figure 2C and Figure 2D). Aggregates of medium-sized cells with indented nuclei and abundant pale cytoplasm, surrounded by small lymphocytes, were noted. Given the rarity of extranodal lymphoproliferative disorders, differential diagnoses such as Kikuchi disease and Kimura disease were considered.
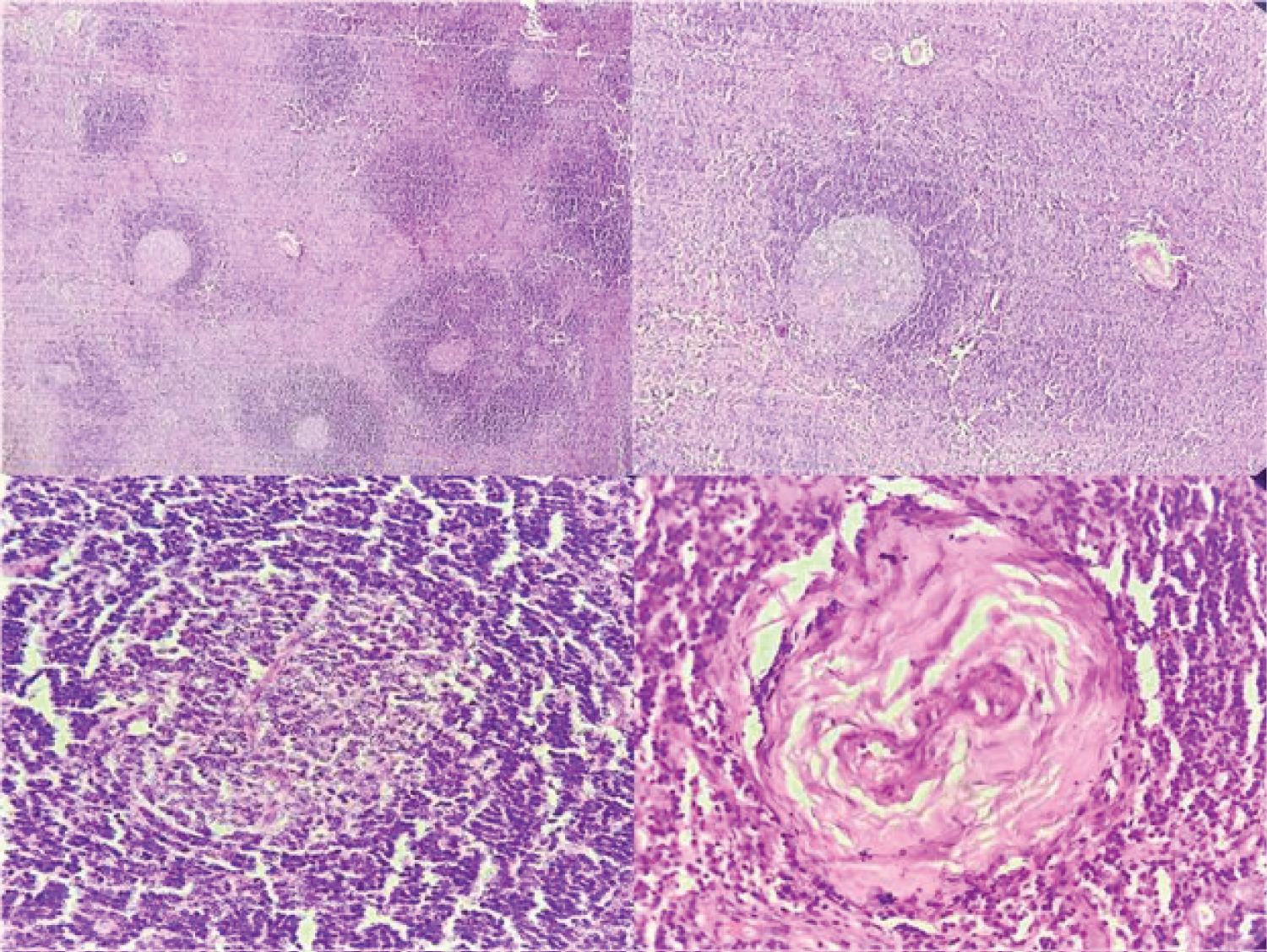 Figure 2: (A, B) Multiple lymphoid follicles with germinal centres showing prominent mantle zone with prominent hyalinised blood vessels; (C) Atrophic follicles with penetrating vessels and onion skinning of mantle zone; (D) Hyalinised blood vessel.
View Figure 2
Figure 2: (A, B) Multiple lymphoid follicles with germinal centres showing prominent mantle zone with prominent hyalinised blood vessels; (C) Atrophic follicles with penetrating vessels and onion skinning of mantle zone; (D) Hyalinised blood vessel.
View Figure 2
Immunohistochemistry (IHC) results showed positivity for CD23, highlighting the follicular dendritic meshwork (Figure 3C), germinal centres positive for CD20 (Figure 3B), T-cell-rich interfollicular areas positive for CD3 (Figure 3A), and vascular proliferation highlighted by CD34 (Figure 3D). Based on the clinical, histological, and IHC features, a diagnosis of Extranodal Castleman Disease of the hyaline vascular type was established.
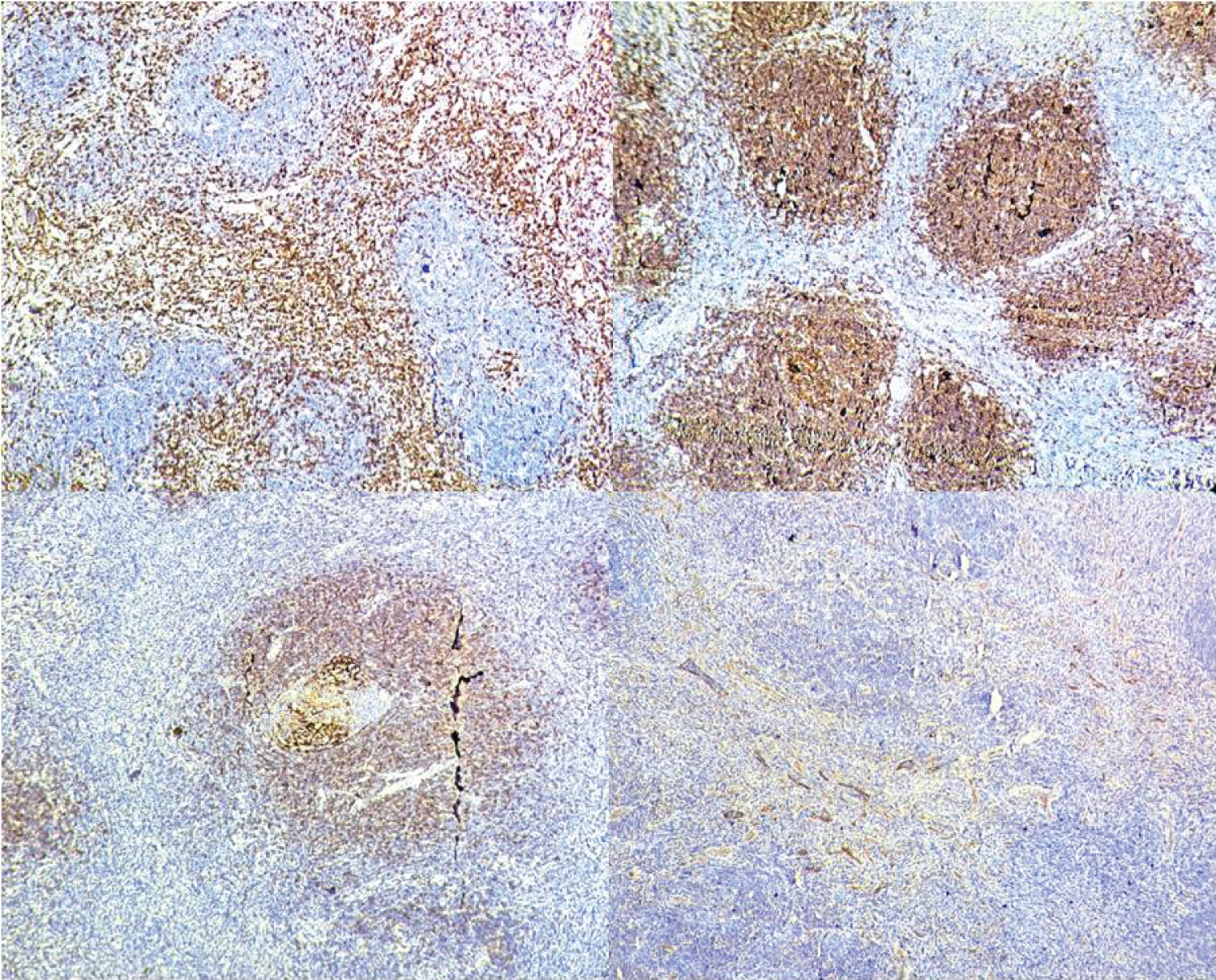 Figure 3: (A) Immunohistochemistry with CD3 stain highlighting the interfollicular areas rich in T cells; (B) Follicles and atretic Germinal centres positive for CD20; (C) CD 23 stain highlighting Dendritic cell meshwork; (D) CD34 stain positivity for vascular proliferation.
View Figure 3
Figure 3: (A) Immunohistochemistry with CD3 stain highlighting the interfollicular areas rich in T cells; (B) Follicles and atretic Germinal centres positive for CD20; (C) CD 23 stain highlighting Dendritic cell meshwork; (D) CD34 stain positivity for vascular proliferation.
View Figure 3
Castleman Disease (CD), also known as follicular lymphoreticuloma, giant lymph node hyperplasia, angiomatous lymphoid hamartoma, and angiofollicular lymph node hyperplasia, is a complex lymphoproliferative disorder [6]. Historically, patients with CD have predominantly presented with mediastinal masses [1]. In 1978, Gaba, et al. reported the first instance of Multicentric CD, characterized by multiple retroperitoneal and axillary lesions with histological features akin to those in Castleman's original series [4].
The pathogenesis of CD, particularly in association with HIV infection, involves a fundamental role of Human Herpesvirus 8 (HHV-8) [7]. Interleukin-6 (IL-6) also plays a critical role in the pathogenesis of CD, with its overproduction favoring the proliferation and maturation of B cells into plasma cells and contributing to increased vascular proliferation [8]. Extranodal involvement in CD is uncommon, and skin involvement is extremely rare, with only eight cases reported to date. These cases predominantly involve subcutaneous or intramuscular areas, localized to regions such as the right shoulder, left arm, left elbow, and wrist. Our case presented with a lesion on the right arm above the elbow. However, in Multicentric CD (MCD), widespread involvement of the trunk and extremities has been observed, with systemic symptoms and concurrent lymph node involvement reported in five cases [9]. Among the seven cases of CD reported in the extremities, the mean age of presentation is 18 years, ranging from 15 months to 29 years, with a female predominance. There seems to be a predilection for the proximal portion of the extremities, as exemplified by our current case localized to the right arm.
In cases where skin involvement is present and lesions exhibit increased vascular proliferation and lymphoid component histologically, the differential diagnosis for CD includes conditions such as angiolymphoid hyperplasia with eosinophilia, Kimura disease, sinus histiocytosis, and angioimmunoblastic lymphadenopathy. Based on clinical presentation and histological features, low-grade cutaneous B-cell lymphomas such as primary cutaneous marginal zone lymphoma (PCMZL) and primary cutaneous follicle center cell lymphoma (PCFCL) should also be considered [10].
This case highlights the diagnostic challenge of extranodal Castleman Disease, particularly in atypical presentations such as solitary masses in the extremities. It underscores the importance of considering CD alongside other lymphoproliferative disorders for accurate diagnosis and effective treatment, especially in female patients.