Objectives: This systematic literature review addresses the use of magnetic resonance imaging (MRI) signal intensity (SI) for the characterization and differentiation of maxillomandibular odontogenic lesions.
Design and methods: Databases were searched for original research studies up to August 2023. The following keywords were used: "magnetic resonance imaging" combined with "maxillofacial pathology," "oral pathology," "odontogenic tumors," "dental tissue neoplasms," and "odontogenic cysts," as well as the histologic denomination of benign odontogenic lesions according to the World Health Organization classification. No language restrictions were applied.
Primary results: Sixteen investigations were identified regarding distinct odontogenic lesions such as ameloblastoma, odontogenic keratocysts (OKCs), and dentigerous cysts. Researchers used various terminologies to describe SI, which influenced the findings of the review.
Principal conclusions: MRI SI can be useful in the differentiation of multicystic ameloblastomas from other odontogenic lesions; notably, multicystic ameloblastomas exhibit heterogeneous SI in T2-weighted images, such that cystic components exhibit higher SI compared with solid content. Dentigerous cysts exhibit high SI in T2-weighted images, while OKCs eventually exhibit lower SI. The terminology used for description of SI is heterogeneous and requires standardization to improve communication among researchers and clinicians.
PROSPERO registration number CRD42021276536.
Magnetic resonance imaging, Neoplasm, Odontogenic tumors, Odontogenic cysts, Dental tissue neoplasms
Odontogenic lesions originate from tooth-producing tissues or their remnants, in conjunction with maxillofacial structures [1]. They represent a wide range of histopathological types and demonstrate various degrees of differentiation and aggressiveness [1]. These lesions are frequently detected initially by panoramic radiographs or cone-beam computed tomography examinations.
Panoramic radiographs and cone-beam computed tomography have limitations inherent to the technique, such as superimposed structures and inadequacy for accurate observation of soft tissues, respectively. Cone-beam computed tomography is widely used in surgical planning for odontogenic lesions, where it provides three-dimensional views of lesions and adjacent anatomic structures, as well as comprehensive assessments of bone tissue [2]; magnetic resonance imaging (MRI) is also increasingly applied for the assessment of odontogenic lesions because MRI can provide fundamental information for differential diagnosis [3].
Thus, the assessment of odontogenic lesions contents and margin features by MRI have been extensively explored by researchers, particularly concerning lesion characterization according to signal intensity (SI) in T1-weighted, T2-weighted, and short TI (or Tau) inversion recovery (STIR) images. However, because the lesions features previously published exhibit considerable heterogeneity, with diverse histological types and classifications, their SI findings are not presumed to exhibit common patterns. Additionally, SI is often regarded as a qualitative assessment; it is typically described using various terms, such as "high SI" [4-13] as a synonym for "hyperintense" [14-17], "low SI" [4,5,8,11-13,15] as a synonym for "hypointense" [14,16,17], or both terms concurrently [18].
The objective of this systematic review was to summarize the SI features of odontogenic lesions and to discuss the terminology used in published descriptions of those lesions. The following questions were considered: The following questions were addressed: 1. "What is the SI of odontogenic lesions according to MRI assessment?" 2. "What is the terminology applied by the investigators to describe lesions SI?"
This systematic review was registered at the National Institute for Health Research, International Prospective Register of Systematic Reviews (PROSPERO), with the registration number CRD42021276536. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was followed when writing this manuscript [19].
The selection of studies potentially eligible for inclusion in this systematic review was performed using PubMed (United States National Institutes of Health’s National Library of Medicine), Embase (Excerpta Medica Database), Scopus (Elsevier), and Web of Science (Institute of Scientific Information-Clarivate Analytics) databases. These databases were searched without language restrictions; articles published on or before September 10, 2021 were included. Keywords were selected considering Medical Subject Headings at the time of the search. Search strategies were established for each database based on the following search keywords: "odontogenic tumors" AND "magnetic resonance imaging"; "dental tissue neoplasms" AND "magnetic resonance imaging"; "maxillofacial pathology" AND "magnetic resonance imaging"; "oral pathology" AND "magnetic resonance imaging"; "ameloblastoma" AND "magnetic resonance imaging"; "squamous odontogenic tumor" AND "magnetic resonance imaging"; "calcifying epithelial odontogenic tumor" AND "magnetic resonance imaging"; "adenomatoid odontogenic tumor" AND "magnetic resonance imaging"; "ameloblastic fibroma" AND "magnetic resonance imaging"; "primordial odontogenic tumor" AND "magnetic resonance imaging"; "odontoma" AND "magnetic resonance imaging"; "dentinogenic ghost cell tumor" AND "magnetic resonance imaging"; "odontogenic fibroma" AND "magnetic resonance imaging"; "odontogenic myxoma" AND "magnetic resonance imaging"; "cementoblastoma" AND "magnetic resonance imaging"; "cements-ossifying fibroma" AND "magnetic resonance imaging"; "odontogenic keratocystic tumor" AND "magnetic resonance imaging"; "odontogenic keratocyst" AND "magnetic resonance imaging"; "radicular cyst" AND "magnetic resonance imaging"; "inflammatory collateral cyst" AND "magnetic resonance imaging"; "dentigerous cyst" AND "magnetic resonance imaging"; "lateral periodontal cyst" AND "magnetic resonance imaging"; "botryoid odontogenic cyst" AND "magnetic resonance imaging"; "glandular odontogenic cyst" AND "magnetic resonance imaging"; "calcifying odontogenic cyst" AND "magnetic resonance imaging"; "orthokeratinized odontogenic cyst" AND "magnetic resonance imaging"; "gingival cysts" AND "magnetic resonance imaging". Because odontogenic keratocysts were previously regarded as "keratocyst odontogenic tumors," the keyword "keratocyst odontogenic tumor" was also used in the search.
Types of studies: Original research studies were considered eligible for inclusion. Abstracts, case reports, oral presentations, and literature reviews were excluded. Research investigations were also excluded if they only used dynamic contrast enhanced MRI (DCE-MRI), contrast-enhanced images (CE), diffusion-weighted magnetic resonance imaging (DWI), and/or apparent diffusion coefficient (ADC).
Types of lesions: Observational studies involving odontogenic maxillofacial lesions, which used MRI and provided descriptions of SI, were included in the data selection.
Data extraction and selection were performed using "Rayyan QRI" [20]. Two reviewers with (Oral radiologists with MRI training) initially screened the titles and abstracts; they then evaluated the full text of each study to choose eligible publications. Disagreements between the reviewers were resolved by discussion; when an agreement could not be reached, other collaborators were consulted. The following data were extracted and summarized: Author information, including the author’s location (country), and the year of study publication; histological type and number of lesions evaluated; investigation objective; lesion SI in MRI; and study main results and conclusions. The data search keywords and results from the databases consulted in this study are summarized in a PRISMA flow chart (Figure 1) [21]. The main literature findings are shown in Table 1 and Table 2.
 Figure 1: Prisma flow chart with the literature search.
View Figure 1
Figure 1: Prisma flow chart with the literature search.
View Figure 1
Table 1: Summary of studies included in this review. Authors and year of publication, country of investigation origin, magnetic resonance imaging (MRI) equipment and potency (in Teslas - T); number of lesions assessed in the study (n); odontogenic lesions assessed according to histological classification; main objective results and conclusions of the selected study. View Table 1
Table 2: Lesion signal intensity in T1-weighted images, T2-weighted images, and STIR images, when available in the studies included in this review. Terms used by the authors to describe signal intensity were maintained. View Table 2
The risk of bias among selected studies was evaluated using the Joanna Briggs Institute risk of bias assessment tool for observational studies [22]; the results are shown in Table 3.
Table 3: Risk of bias among the included studies, according to the joanna briggs institute assessment tool [22]. View Table 3
In total, 1291 studies were initially identified in the database search using all keywords. After the application of inclusion and exclusion criteria, as well as the removal of duplicate articles, 1275 studies were excluded. Finally, 16 studies [4,5,7-18,23,24] were included in the review. A PRISMA flow diagram (version 2020) for study selection is shown in Figure 1 [21]. A summary of the selected studies is provided in Table 1, along with each study’s main objective, results, and conclusions.
The oldest study included was from 1996 [4] and the most recent study was from 2021 [18]. The MRI equipment strength ranged from 0.064T [4] to 3T [13,17,18]. Researchers also considered the use of other MRI techniques, such as T1-weighted images with intravenous contrast injection [5,8,9], DCE images [9], and DWI [11,12,14,17,18].
The numbers of lesions analyzed ranged from five [23] to 127 [18]. The histological types of lesions assessed were (in order of frequency): ameloblastomas [4,7-9,11,13,14,17,18,23], OKCs [4,5,8,10-12,14,17,18], dentigerous cysts [5,8,11,12,14,17,18], radicular cysts [12,16,24], nasopalatine duct cysts [5,12], odontogenic myxomas [14,15], and odontogenic glandular cysts [5]. Solid and cystic contents of multicystic ameloblastomas were separately evaluated in some investigations [4,7,9,11,14], while other investigations evaluated such lesions as single entities [8,13,23].
The terminology used to describe SI differed among studies, as indicated in Table 1, Table 2 and Table 3. To describe SI uniformity (visual pattern homogeneity), the terms "homogeneous" and "heterogeneous" were used by most researchers [4-13,15,17,18,23,24]. The term "inhomogeneous" [16] was sometimes used to describe a mixed pattern lesion; this term was not used in many studies [4,11,14,17,18]. Concerning SI itself, the following terms were used: "high SI" [4-13] or "hyperintense" [14-18], with variations such as "slight high" [5-7,9], "bright high" [23], "markedly high [8,9]," "extremely high" [18]; "intermediate SI" [5-10,15,23] or "isointense" [18]; and "low SI" [4,5,8,11-13,15] or "hypointense" [14,16-18], with variations such as "moderately low" [13] and "slight low" [9]. Table 2 shows the SI terms used by each author. STIR images were described by four authors [9,10,12,24] and the use of T2-weighted imaging with fat suppression was mentioned by five other authors [11,16,18,23]. Figure 2 and Figure 3 show representative SI terms, selected by the authors of the present review, using the most recent terms applied in the literature.
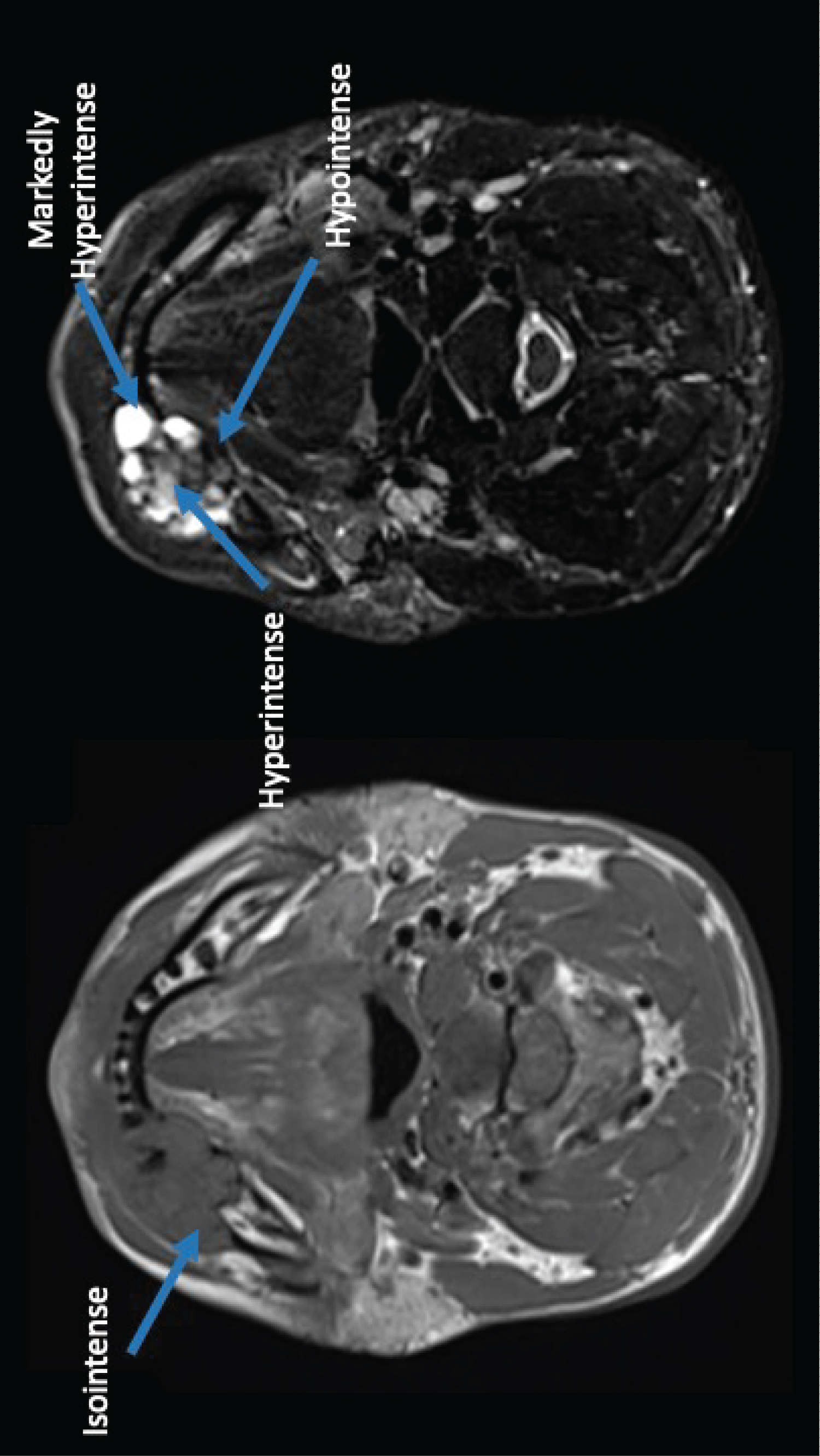 Figure 2: Representative terms for signal intensity, selected by the authors of the present review, using the most recent terms applied in the literature. Case of multicystic ameloblastoma. From the left to the right: First image is a T1WI image, axial slice, shows an isointense area which has similar intensity compared to muscle. Second image is a STIR image, axial slice, demonstrating hyperintense, hypointense and markedly hyperintense areas.
View Figure 2
Figure 2: Representative terms for signal intensity, selected by the authors of the present review, using the most recent terms applied in the literature. Case of multicystic ameloblastoma. From the left to the right: First image is a T1WI image, axial slice, shows an isointense area which has similar intensity compared to muscle. Second image is a STIR image, axial slice, demonstrating hyperintense, hypointense and markedly hyperintense areas.
View Figure 2
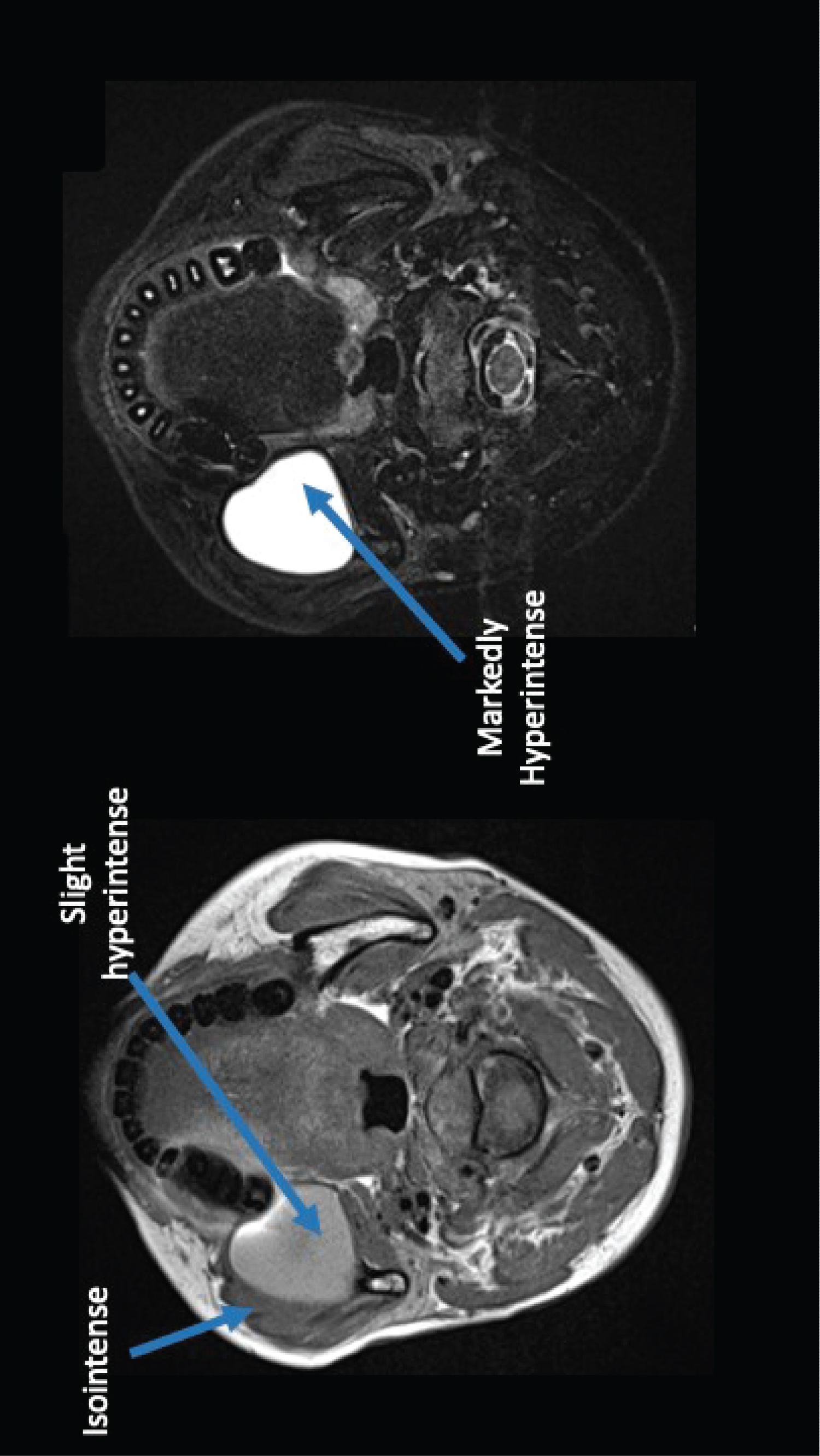 Figure 3: Representative terms for signal intensity, selected by the authors of the present review, using the most recent terms applied in the literature. Case of unicystic ameloblastoma. From the left to the right: First image is a T1WI image with isointense and slight hyperintense areas. Second image is a STIR image with a markedly hyperintense area.
View Figure 3
Figure 3: Representative terms for signal intensity, selected by the authors of the present review, using the most recent terms applied in the literature. Case of unicystic ameloblastoma. From the left to the right: First image is a T1WI image with isointense and slight hyperintense areas. Second image is a STIR image with a markedly hyperintense area.
View Figure 3
The risk of bias assessment is shown in Table 3. Confounding factors included the lack of information concerning MRI equipment, use of various types of equipment, and the absence of histopathology confirmation. Two articles did not report the MRI equipment strength [15,16].
MRI is essential for non-invasive diagnosis involving soft tissue; its applications have been widely studied in dentistry [25]. MRI uses a powerful and uniform static magnetic field with radio frequency pulses to create images of target tissues [25]. In particular, T1- and T2-weighted images reflect distinct stages of the pulse sequence [26]; the SI in these images is determined by tissue features, such as the presence of water molecules and adipocytes. T1-weighted images are useful for evaluation of normal and pathological tissues with high fat content or hyperintense SI [27], T2-weighted images are useful for the identification of pathological tissues with high water and fat content or hyperintense SI [28], and STIR imaging is a fluid-sensitive sequence with fat suppression [29].
Considering the differences in SI among T1-weighted images, T2-weighted images, and STIR images, a lesion is likely to exhibit distinct SI in each type of images. Each lesion’s histopathological features are also likely to exhibit distinct SI, as demonstrated in the investigations included in this review. Although this argument appears logical, lesions with the same histopathological characteristics and classification varied among patients, as indicated by the heterogeneous findings in Table 2.
Multicystic ameloblastoma, which comprises 90% of all ameloblastom as diagnosed in the oral cavity [30], frequently exhibited heterogeneous SI in T2-weighted images; SI was also increased in cystic contents within the lesion [8,13,23]. For this particular lesion, MRI allows the observation of cystic and solid contents [7], thus enabling differentiation from other purely cystic lesions (e.g., OKCs, unicystic ameloblastomas, and dentigerous cysts). The cystic contents of ameloblastomas often exhibit higher SI in T2-weighted images, compared with T1-weighted images [4,7,11,14], because of its high water content. For example, Apajalahti , et al. [23] reported that multicystic ameloblastomas had homogeneous SI in MRI.
In our review, all unicystic ameloblastomas and dentigerous cysts exhibited variations of high SI in T2-weighted images [5,8,9,11,12,14,17,18]. In contrast, some OKCs exhibited low SI in T2-weighted images [17,18] and other OKCs exhibited heterogeneous SI in T2-weighted images [5,8,17]. The diversity of SI among OKCs is related to the materials contained inside the lesions [31]; for example, the considerable amount of keratin sometimes associated with hyaline [5] is likely to reduce the quantity of water molecules and corresponding SI in T2-weighted images.
The lack of a specific SI pattern prevents differentiation among odontogenic lesions using qualitative SI assessment alone. Hence, complementary MRI techniques (e.g., DWI and DCE images or CE-T1-weighted images) are needed to differentiate among odontogenic lesions. DCE and CE-T1-weighted images are reportedly useful in the differentiation of odontogenic cysts [5,8,9]. DWI can also aid in differentiating unicystic ameloblastomas from OKCs [11] and OKCs from dentigerous cysts [12]; this method does not require the use of contrast [3].
Concerning lesion identification using STIR images, only a few studies have described the use of this MRI parameter [9,10,12], although five studies mentioned the use of T2-weighted images with fat suppression [11,16,18,23]. STIR sequence reconstruction produces images that are similar to T2-weighted images; however, because the fat signal is suppressed, non-fatty tissues exhibit higher SI, which may result in higher SI in fluid or fluid-containing areas [29]. This approach facilitates assessment of odontogenic lesions with cystic content because these lesions are highlighted in the resulting images.
Another important consideration is the diverse terminology used to describe the odontogenic lesions. We maintained the SI terms used in each study because we were unable to distinguish some terms, particularly those derived from "high" or "hyperintense" and "low measurement" or "hypointense." For example, "bright high" may be a synonym for "extremely high" or "markedly high," but it is unclear whether "intermediate to high" is a synonym for "slight high." The qualitative classification approach is subjective to observer bias. Hence, a quantitative SI approach could provide allow more accurate detection of slight color variances among images produced using each MRI protocol. Notably, quantitative values were analyzed by Fujita, et al. [32] using the "SI uniformity" approach; this confirmed that cystic components of ameloblastomas (e.g., unicystic ameloblastomas) could be differentiated from OKCs in both T1-weighted and T2-weighted images.
This review had some limitations. Although the use of SI in the diagnosis of the odontogenic lesions was first published in 1996 [4], we found relatively few studies that fulfilled the inclusion criteria for this review. Furthermore, each study included a small number of lesions. Finally, the heterogeneous SI terminology may have influenced the lesion assessments.
MRI SI can be useful in the differentiation of multicystic ameloblastomas from other odontogenic lesions; notably, multicystic ameloblastomas exhibit heterogeneous SI in T2-weighted images, such that cystic components exhibit higher SI compared with solid content. Dentigerous cysts exhibit high SI in T2-weighted images, while OKCs eventually exhibit lower SI. The terminology used for description of SI is heterogeneous and requires standardization to improve communication among researchers and clinicians.
We thank Ryan Chastain-Gross, Ph.D., from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Authors declare no conflict of interest.
Not applied.
No funding was available for this research.
Luciana Munhoz idea, databases research, manuscript writing, Shunsuke Okada critical review, manuscript drafting; Miki Hisatomi manuscript correction, figures, critical review; Mariko Fujita critical review, idea, manuscript writing,; Yudai Shimizu critical review, main concepts, Yoshinobu Yanagi critical review; Emiko Saito Arita critical review, Jun-ich Asaumi critical review and main concepts.