Background: Mobile C-arm units are portable fluoroscopy systems that allow real-time images of the internal structures of the body. The equipment is designed to be very maneuverable. The versatility of the terminologies introduces significant communication barriers between the surgeon and the radiographer.
Objective: The objective of the review is to identify the commonly used c-arm communication terminologies and determine the prevailing issues of not having a uniform c-arm communication terminology between the radiographer and surgeon inside the OR.
Method: A systematic search of the literature published in 2007-2022 was conducted using PubMed, Google Scholar, and Cochrane Library. Participants of the study in the selected research articles should be radiographers and orthopedic surgeons only. A dedicated data extraction tool was developed and used to collect relevant information from the eligible studies.
Results: Out of 72 articles identified through database searching, 63 duplicate studies were excluded. Of the 9 remaining records, three of them are not in full text. A total of 6 full-text articles were assessed for eligibility. 2 articles were removed since they failed to meet the eligibility criteria. A total of four studies were included in the review.
Conclusion: The findings from this systematic review indicate that there is no standard universal c-arm language. Poor communication exists between the orthopedic surgeon and radiologic technologist who lead to confusion, surgical delays, mutual frustration, and increased exposure to ionizing radiation. Adoption of a common c-arm language might potentially address the issues relating to poor communication.
C-arm language, Orthopedic surgeon, Radiologic technologist
Mobile C-arm units are portable fluoroscopy systems that allow real-time images of the internal structures of the body [1]. The equipment is designed to be very maneuverable. The C-arm itself is attached to a beam located on the base of the C-arm that can be raised, lowered, or extended as needed [2]. The emergence of this X-ray technique has facilitated the acquisition of almost any view of the desired anatomy necessary for orthopedic surgeries such as fracture reduction and instrumentation to foreign body removal [3,4]. Though manufacturers have given names to the various movements of the C-arm unit in operating manuals, these have not been popular among orthopedic surgeons or radiographers [5]. The versatility of the terminologies introduces significant communication barriers between the surgeon and the radiographer.
In the survey conducted by Palley and Kreder [6], it was reported that the vast majority of orthopedic surgeons and radiographers denied having been taught a standard universal language for c-arm use during school or training. Currently, no consistent and widely used set of terms exists to facilitate communication regarding the positioning of the fluoroscope. Hence, surgeons rely on their personal judgment in assigning terminology to specific c-arm maneuvers. The radiographers then rely on their personal judgment in interpreting the meaning of directions given by the surgeon. Poor communication between orthopaedic surgeons and radiographers during the use of C-arm leads to surgical delays, mutual frustration, and increased exposure to ionizing radiation [7].
The objective of this review is to identify the commonly used c-arm communication terminologies and determine the prevailing issues of not having a uniform c-arm communication terminology between the radiographer and surgeon inside the OR. Thus, concerns related to incoherent and ambiguous instructions for C-arm movements might be addressed. Moreover, this will aid in the composition of uniform c-arm communication terminologies and eventually be included in course content of radiologic technology program as well as its implementation in the actual practice. More so, this systematic review has been designed with the aim of answering the following questions:
1. What is the range of existing literature surrounding the use of C-arm communication terminologies between radiographers and orthopedic surgeons?
2. How does non-uniform C-arm language affect communication between radiographers and surgeons?
3. What are the outcomes of having a uniform C-arm language in the Operating Room?
Inclusion and exclusion criteria are presented in Table 1.
Table 1: Study inclusion and exclusion criteria. View Table 1
Electronic search for the studies relating to c-arm language was performed using three databases namely PubMed, Google Scholar, and Cochrane Library for studies published in English from 2007 to 2022. Studies were identified by searching subject headings and text words of the concepts “C-arm language”, “orthopedic surgeon”, and “radiologic technologist”.
The researcher independently screened titles and abstracts of all potentially relevant citations against the detailed inclusion and exclusion criteria listed in Table 1. The screening process is presented using the PRISMA flow diagram to outline search results, depicting the number of studies included or excluded (Figure 1).
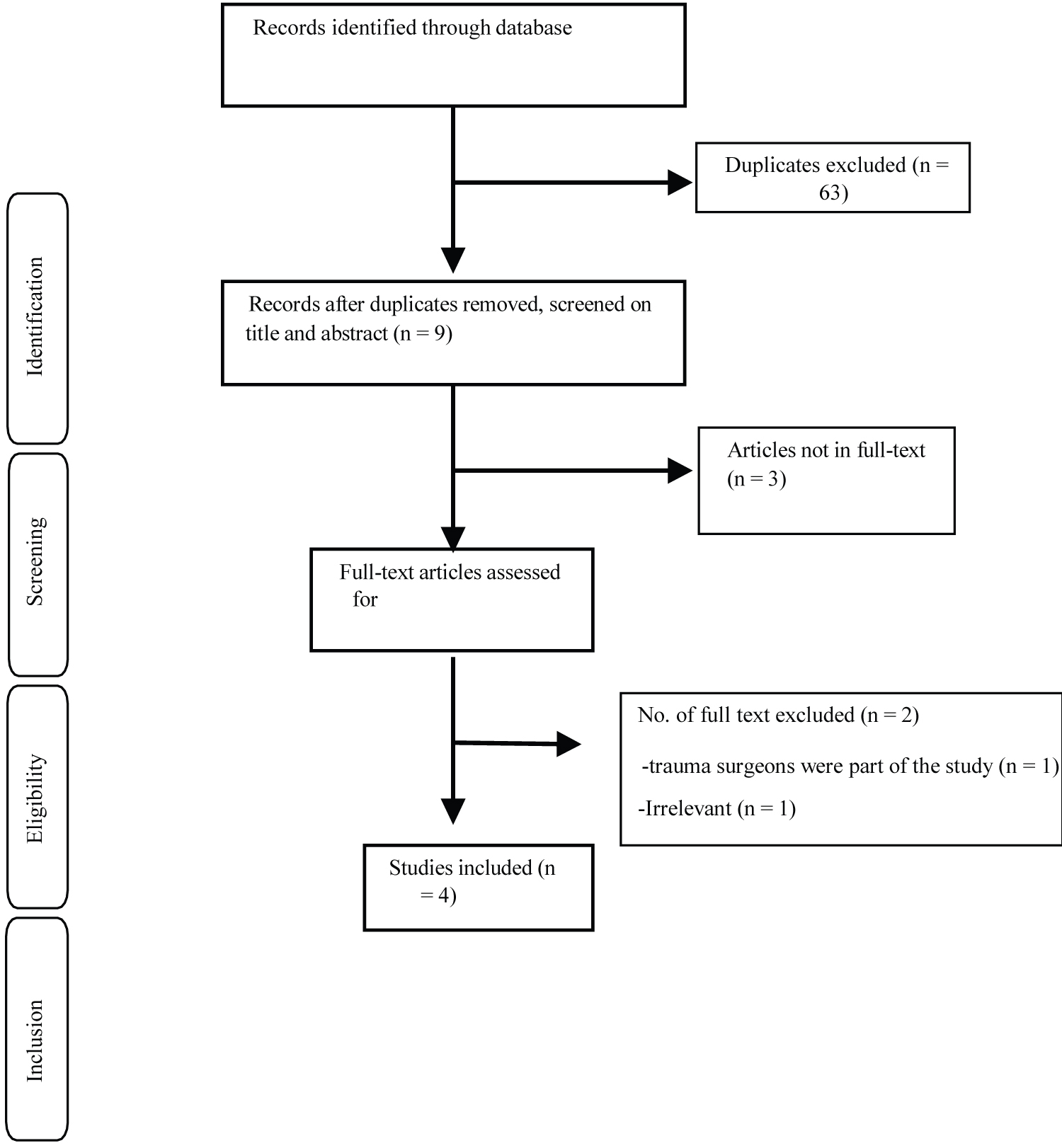 Figure 1: PRISMA flowchart: Outline of the study selection process using inclusion and exclusion criteria.
View Figure 1
Figure 1: PRISMA flowchart: Outline of the study selection process using inclusion and exclusion criteria.
View Figure 1
The following relevant information was extracted for each study: Author/s (Year), country, study design, study population, identified c-arm movement communication terminology, and key findings (Table 2).
Table 2: Description of included studies. View Table 2
The researcher independently performed the data checking by comparing all the included full-text articles to the data extraction sheet.
The synthesis was performed in accordance with the Cochrane guidelines for diagnostic test accuracy reviews.
The results of the study selection process are illustrated in Figure 1.
Of the four included studies, one employed a prospective, cross-sectional survey design, while the other three used a descriptive, non-experimental design. All of the included articles had orthopaedic surgeons and radiologic technologists as their population sample.
The quality of the selected studies was assessed using a standardized research literature appraisal tool from Yale New Haven Health, Nursing Research and Evidence-Based Practice Committee. The checklist is provided in Appendix A.
According to the study conducted by Stirtonetal, et al. [7], there is no standard universal c-arm language. Hence, there is a tremendous in consistency in the language used by orthopaedic surgeons and radiation technologists [6]. As a result, confusion and miscommunication arise between surgeons and technologists. A common language and precision in command can avoid confusion and have the potential to improve theater time utilization [5]. A summary of relevant data from the studies is presented in Table 2.
Majority of orthopedic surgeons and radiologic technologists have not been taught a standard universal communication terminology for c-arm use during school or training. A study by Pally and Kreder wherein orthopedic surgeons and radiologic technologists were asked to write descriptors of diagrams illustrating different c-arm movements found that little to no consensus exists within or between these two groups in regard to what terminology should describe which c-arm movement. They found that the terminology used to direct the fluoroscope to be tremendously diverse since identical language was used by different respondents to indicate different movements.
Without a standardized c-arm language, poor communication between orthopedic surgeons and radiologic technologists regarding the use of c-arm exists. This results in confusion, surgical delays, mutual frustration, and increased exposure to ionizing radiation. In the study conducted by [7] 91% of surgeons and radiologic technologists have witnessed unnecessary imaging taken in the OR as a direct consequence of confusion between surgeon and radiologic technologist. In the vast majority of cases where it exists, both patient and surgeon are exposed unnecessarily.
Using a pre-prepared communication strategy, it was proven that use of a common c-arm language could significantly improve the efficiency and safety of fluoroscopic C-arm uses [9]. For an effective communication between the orthopedic surgeons and radiologic technologists, it is important to use the names of the various c-arm movements. Moreover, introduction of a uniform c-arm language early in training would save much time and effort. Thus, efficient communication would hopefully become an unconscious part of operating the c-arm in every case. This review has a limitation that could be addressed in future research. It should be noted that this review is limited to orthopedic surgeons only.
The findings from this systematic review indicate that there is no standard universal c-arm language. As a result, poor communication exists between the orthopedic surgeon and radiologic technologist that lead to confusion, surgical delays, mutual frustration, and increased exposure to ionizing radiation. Adoption of a common c-arm language might potentially address the issues relating to poor communication.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
This paper was reviewed by the ethical committee of the Institutional Review Board, Holy Angel University. Please see Appendix B.
I wish to record my deep sense of gratitude and profound thanks to the following: Dr. Violeta Lopez, Dr. Carlo Bryan Borrico, and Abby Louisse Pearl Ventura for their keen interest, guidance, constant encouragement with my work during all stages, to bring this systematic review into fruition.