A 37-year-old male patient with a complaint of malaise applied to the internal medicine. The abdominal CT revealed an huge nonadenom adrenal mass lesion with 51 × 43 × 64 mm size. The significant finding was adreniform shape of gland was maintained in the lesion.
The adrenal lymphoma should be considered in patients with adreniform shape of nonadenom adrenal lesion on CT. The MRI enables differentiation of adrenal adenomas from other adrenal malignancies, but specific diagnosis might not be achieved with this modality.
Nod-Hodgkin lymphoma (NHL) frequently involves adrenal gland and to be usually bilateral. The computed tomography (CT) and magnetic resonance imaging (MRI) are the most important radiological imaging modalities for differentiating adenomas from malignant lesions like lymphoma of adrenal gland and prevent unnecessary surgical interventions to adrenal lymphoma.
A 37-year-old male patient with a complaint of malaise applied to the internal medicine. No significant findings were found in the blood tests. As he described a blunt pain in the left upper quadrant on physical examination, abdominal ultrasonography (US) was depicted a hypoechoic lesion adjacent to the upper pole of left kidney. The dynamic computed tomography (CT) with contrast material was revealed a huge adrenal mass lesion with 51 × 43 × 64 mm size. The lesion engulfed the adrenal gland without disturbing the shape of the normal gland (Figure 1a and Figure 1b). Within the lesion, both limbs and limb junction of the gland were easily selectable in their own densities. There was marked diffusion restriction on diffusion weighted imaging but we could not distinguish the appearance of adrenal gland within the lesion on any MRI sequence unlike CT (Figure 2). The washout values on the delayed phase of CT favored nonadenoma lesion without no calcification, fat and cystic area.
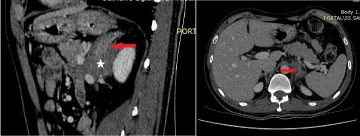 Figure 1: Portal phase images of CT in the sagittal (a) and axial (b) plan. Adrenal gland involvement of the lymphoma (white star) is presented while the gland with normal shape could be selected within the lesion (red arrow). View Figure 1
Figure 1: Portal phase images of CT in the sagittal (a) and axial (b) plan. Adrenal gland involvement of the lymphoma (white star) is presented while the gland with normal shape could be selected within the lesion (red arrow). View Figure 1
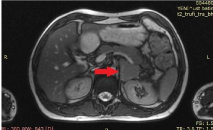 Figure 2: High-resolution, T2W sequence without fatsat in the axial plane. This sequence for anatomical orientation could not be revealed the gland within the lesion (red arrow). View Figure 2
Figure 2: High-resolution, T2W sequence without fatsat in the axial plane. This sequence for anatomical orientation could not be revealed the gland within the lesion (red arrow). View Figure 2
Due to absolute (32%) and relative washout (13%) values of the lesion on CT, it was evaluated in the group of non-adenoma adrenal lesion. The biopsy resultant of lymph node with high activity on PET CT (Figure 3) was B-cell acute lymphoblastic lymphoma and the adrenal lesion was primarily considered to be lymphoma. During the medical treatment, the size of the adrenal lesion was markedly decreased and it could be seen as an adreniform shape (Figure 4). Adrenal insufficiency did not develop in follows-up.
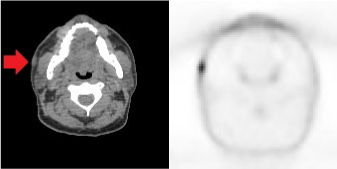 Figure 3: a,b) Axial images of PET CT. The lymph node under the skin adjacent to right masseter muscle (red arrow) was observed to be hypermetabolic. View Figure 3
Figure 3: a,b) Axial images of PET CT. The lymph node under the skin adjacent to right masseter muscle (red arrow) was observed to be hypermetabolic. View Figure 3
 Figure 4: The image of follow-up CT after treatment. The soft tissue lesion of the lymphoma is significantly regressed and the enlargement of the gland with the maintenance of the adreniform shape was observed (red arrow). View Figure 4
Figure 4: The image of follow-up CT after treatment. The soft tissue lesion of the lymphoma is significantly regressed and the enlargement of the gland with the maintenance of the adreniform shape was observed (red arrow). View Figure 4
A variety of CT appearances of primary adrenal lymphomas have been reported. A recent review of the CT appearance described an approximately even distribution of homogeneous and heterogeneous patterns, with the majority of tumors having a hypoattenuating appearance and slight to moderate enhancement [1]. In secondary adrenal lymphoma, the adrenals may appear normal, diffusely enlarge while maintaining a normal morphology, or demonstrate solitary or multiple masses [2]. Extensive retroperitoneal disease may engulf the adrenal. Secondary lymphoma tends to be homogeneous in attenuation with low-level enhancement and slow washout on delayed images. Calcifications are rare in the absence of prior treatment [3]. At MR imaging, primary and secondary lymphomas are hypointense to isointense on T1-weighted images and hyperintense on T2-weighted images when compared with liver [2]. Mild to moderate enhancement is commonly seen [4]. Given the highly cellular nature of lymphomatous masses, restricted diffusion is commonly seen [1]. 18F FDG PET is commonly performed for staging and treatment monitoring in lymphoma and may be helpful in evaluation of the adrenals [5].
The adrenal lymphoma could also infiltrate the gland which can be seen as an adreniform shape as in the post treatment image of this patient. Adreniform shape is caused by the infiltration of tumor cells and increasing the gland size with maintaining the gland shape. This appearance has also been reported in benign processes as cortical hyperplasia of the gland, nontraumatic hematomas, metastatic disease, tuberculosis and fungal infections [6].
Secondary involvement of the adrenal gland with NHL has been reported in as many as 25% of the patients with NHL [7]. In this case, we observed that the appearance of the lesion on CT may sometimes be a helpful clue in the differential diagnosis and may suggest the lymphoma as a priority. To avoid unnecessary surgery of adrenal lymphoma, in some cases, the appearance feature on CT may provide the presence of lymphoma at the top of your differential diagnosis list.